Article Text

Abstract
Objectives This study draws on qualitative insights on the barriers and facilitators to HIV testing, as well as perceptions of HIV self-testing (HIVST), to propose a framework to understand not only the benefits but also potential knock-on implications of introducing HIVST in the context of other STI testing.
Methods We conducted semistructured, in-depth interviews with 30 gay, bisexual and other men who have sex with men aged 18 and 39 years old in Singapore. Interview topics included barriers and facilitators to HIV and other STI testing, as well as perceptions of HIVST. Interviews were audio-recorded, transcribed, coded and analysed using thematic analysis.
Results For HIV testing, participants cited the perceived risk of acquiring, susceptibility to and symptoms of HIV as internal motivators, while social influence and accessibility of HIV testing services were external motivators. For STI testing, perceived symptoms and partner notification of STI were reported as internal and external motivators, respectively. Availability of bundle tests, starting a new relationship and instances of mandatory testing motivated both simultaneous HIV and other STI testing. The fear of a positive diagnosis and lack of confidentiality were cited as internal and external barriers to HIV testing, respectively, while low perceived severity of other STI and the cost of STI tests were cited as internal and external barriers to other STI testing, respectively. We identified pathways to HIV and other STI testing and discussed how the introduction of HIVST may reduce opportunities for other STI testing.
Conclusions The findings of this study suggest that introducing HIVST might weaken linkages to other STI testing if alternative strategies of promoting other STI testing are not simultaneously implemented. We recommend that future interventions address both the risks of HIV and other STI simultaneously, and that structural interventions promoting HIV and other STI preventions be balanced accordingly.
- HIV testing
- diagnosis
- gay men
- health services research
- HIV service delivery
Data availability statement
Data are available upon reasonable request. Data are available upon reasonable request from the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Gay, bisexual and other men who have sex with men (GBMSM) are disproportionately affected by HIV and other STIs relative to the general population in various settings around the world.1 In spite of this elevated risk of acquiring HIV and other STIs, rates of testing remain suboptimal, even in settings where concentrated epidemics among GBMSM prevail.2–5 Early detection of HIV and other STIs provides several benefits for both individuals and the communities that are disproportionately affected by them. Specifically, early diagnosis of HIV and initiation of treatment are associated with an improved life expectancy and delay in the onset of AIDS-related opportunistic infections,6 7 and prevent onward transmission of HIV when viral suppression is achieved among people living with HIV.8 Early diagnosis of bacterial STIs such as syphilis also reduces the risk of HIV acquisition and onward transmission to others via vertical or sexual transmission routes.9
Barriers and facilitators to HIV testing among GBMSM have been well established in the literature, including the anticipation of stigma, extent of sexual orientation disclosure, low-risk perceptions of HIV infection and fear of a positive HIV diagnosis; conversely, increasing age, educational attainment and a history of other STIs have been found to be positively associated with both ever and regular testing for HIV among GBMSM.10–16 A relatively novel intervention that may enable individuals to overcome such barriers involves the introduction of rapid result HIV self-testing (HIVST). The introduction of self-sampling methods arrived with the advent of over-the-counter home collection kits where blood specimen, collected outside of clinic settings, are sent to laboratories for testing. Then came rapid test kits that provided rapid results at clinical settings and, finally, kits that can be bought over the counter and be used outside of clinical settings to provide rapid results for individuals, which is now more commonly referred to as HIVST.17 Past studies have reported that GBMSM perceive a high acceptability towards HIVST, and it may be useful in reaching GBMSM who do not have access to facility-based testing.18–20 More efforts are also being made to better understand how the detection of other STI may also be introduced alongside HIVST as more testing takes place outside of clinical settings.21 22
In Singapore, despite established and ongoing HIV prevention efforts among GBMSM, the proportion of GBMSM who made up incident cases of HIV surpassed that of heterosexual men in 2011, and the trend has persisted since.23 At this point, HIVST has not been approved for use in Singapore, and HIV and other STI testing may only be conducted in clinical settings, or at a list of 10 government-sanctioned anonymous test sites based in nine general practitioner clinics and one site managed by a community-based organisation. These anonymous test sites were introduced to encourage HIV testing with the promise of anonymity, as all individuals who test positive for HIV in non-anonymous settings must, by law, be notified to the authorities under the Infectious Diseases Act in Singapore.24
While most studies have demonstrated the efficacy or the positive impact of HIVST on the early diagnoses of HIV among GBMSM, less efforts have been made to contextualise such findings in terms of its broader impact on other STI testing. Specifically, we explore how the introduction of HIVST would impact existing patterns of STI testing that are contingent on facility-based HIV testing by drawing on insights from a qualitative study on the motivators and barriers to HIV and other STI testing among GBMSM in Singapore, as well as their perceptions of HIVST. This is also the first published study on HIVST among GBMSM in Singapore and will help inform its implementation in time to come. We propose a framework to understand not only the benefits but also the potential knock-on implications of introducing HIVST in the context of other STI testing, as well as recommendations to strengthen sexual health promotion systems in view of these emerging health service gaps.
Methods
Study design and participants
We conducted in-depth interviews (IDIs) with GBMSM who are between 18 and 39 years old and are Singaporean, permanent residents or have resided in Singapore for more than a year. The participants were purposively sampled for maximum variation of opinions and experiences and were recruited through a recruitment poster on display at the Department of STI Control, the Communicable Disease Centre and through the contacts of the community stakeholders such as people who work with or volunteer for HIV prevention, care and treatment among GBMSM, as well as opinion leaders within the GBMSM community. A summary of participant demographics is included in table 1.
Summary of demographics of IDI participants
Semistructured interview guides were developed and piloted with two self-identified GBMSM to ensure its appropriateness and ease of use. Topics explored include user experiences of current HIV and STI testing services, motivators and barriers to HIV and STI testing, and recommendations on ways to improve on these services. Participants’ views on HIVST were also explored. Demographic data of participants such as age, gender, educational level, occupation, number of sexual partners, frequency of condom use and HIV/STI testing, and HIV status were collected.
Data collection
Thirty IDIs were conducted between January and July 2016. All participants gave verbal consent to participate in the study and for the interviews to be audio-recorded. They were reimbursed US$90 (about US$67) for their time taken for the interview. Except for one interview that took place behind a screen, all IDIs were conducted face-to-face by two experienced qualitative researchers and took approximately 60 min each to complete. Study participants were recruited until theoretical saturation occurred, when the research team had reviewed the interview data and were satisfied that no new themes were generated from subsequent interviews.25
Data analysis
Audio recordings were transcribed verbatim (OZL and BCHC), reviewed for accuracy by two other researchers (YYC and MABI), and reread by the study team to familiarise themselves with the data. To achieve intercoder agreement, we adopted a subjective assessment method26 where, using a preliminary structural codebook, five researchers coded a randomly selected transcript independently and the coded transcript was reviewed section by section to discuss coding discrepancies and amend the master coding document accordingly. The five researchers then coded another transcript using a revised codebook. This process occurred iteratively until a fourth and final codebook was developed and used to code all the remaining transcripts. Codes were then organised using QSR International’s NVivo V.10 qualitative data analysis software, summarised in relation to the study objectives and analysed using thematic analysis.26
Results
Table 2 summarises the themes and subthemes of motivators and barriers towards HIV and other STI testing. These motivators and barriers were organised as either internal or external factors, depending on whether they had originated from the individual or from an external source.
Motivators and barriers towards HIV and other STI testing
Motivators to HIV testing
Participants highlighted three main internal motivators to testing for HIV. First, participants articulated how a heightened sense of risk following sexual encounters led to their decision to test for HIV:
I: So I remember seeing that, so you have done a HIV in the past 6 months and what makes you decide to get yourself tested?
IDI05: I had unprotected sex.
Second, many participants also highlighted how they felt that they were susceptible to HIV, and so had scheduled regular or routine testing for HIV:
IDI04: I know I should, given my sexual history I should probably go every two or three months but erm, six months is probably too long already, for me. I would say three months.
Participants also highlighted how they were motivated to test for HIV when they had perceived themselves to be having symptoms of HIV:
IDI07: At that point of time, I think, because I was feeling a bit uneasy, whether I had HIV or not […] I was having fever from ups and downs. Fever – and I felt a bit uneasy; I also started to itch a lot, and so just to know what’s happening, I went for the test.
Participants also described two external factors that applied to HIV but not STI testing. First, many felt that they were motivated to test through influence or encouragement from their friends:
IDI15: Because I had one or two like unsafe encounters prior to that so I was quite worried. So after confiding in my friends, one of whom volunteers for [community-based organisation], like erm, they finally convinced me to go get tested.
Second, participants also articulated how HIV testing was often free and easily accessible through mobile testing sites and community-based venues:
IDI27: When I signed up for it, they gave me a test… A free [HIV] test coupon … And I guess because that I wanted the test to be free of charge, so I agreed to it. And I went to get a free test.
Motivators to other STI testing
In the context of testing for other STI, participants highlighted one internal as well as one external motivator. First, like HIV, participants were motivated to test for other STIs when they had perceived themselves to have symptoms:
IDI26: I had symptoms of it. Erm, yellow discharge, peeing razor blades. Erm, sharp pains when you're peeing. Yup… swollen testicles.
Second, participants had recalled how they were motivated to test for other STIs when they were notified by their partners for having been diagnosed with STI:
IDI25: It’s because my, my partner tested positive for Gonorrhoea. Ok, so I thought, maybe I should check whether I had Gonorrhoea, which I did, but I wanted to do a comprehensive test as well because might as well do it since I'm there already. So, that was the time when I was surprised with my result. Because I really didn't expect it.
Motivators to simultaneous HIV and other STI testing
Participants highlighted several situations in which they had tested for both HIV and other STIs simultaneously; these were typically driven by three external motivators. First, several participants articulated how they had either, or both HIV and other STI tests done in the course of mandatory screening, such as in the case of pre-employment medical check-ups or conscription for national service:
IDI04: Well my last full panel check was… my last full panel check [including HIV and other STI] was probably my medical check-up for employment.
Second, participants also described how they had wanted to test for HIV and other STIs for a clean slate of health when they were entering new romantic, committed partnerships with others:
IDI03: Primarily for um, like reassurance. Because, at that point of time, I was getting into a relationship. […] So I did want to find out if I was [HIV] negative […] I had unprotected sex before the relationship so I wanted to be able to commit to my partner.
Finally, several participants also reported testing for both HIV and other STIs in situations where tests were sold or offered as bundles at the clinics:
IDI15: So like I decided to go ahead and get STI testing since like it could be done concurrently with the HIV testing.
Barriers to HIV testing
Participants shared two main barriers to testing for HIV. First, several participants highlighted there was a fear of receiving one’s potential diagnosis of HIV. One participant shared:
IDI25: I think he had a feeling that he [my ex-partner] had it [HIV]. He just didn’t want to, I don’t know. I think he just… I don't know how to say this but, he, he’s too busy to have time for it. Like, one of the problems where you just wanna put it aside first.
Second, anonymity and confidentiality was a major concern among most participants. One participant cited the need for confidentiality of HIV testing services:
IDI09: That’s also the other reason why they don’t want to do HIV test at (local sexual health specialist clinic], because they are afraid their particulars will be taken, will be recorded and such.
Barriers to other STI testing
Participants shared two main barriers to testing for other STIs. First, several participants described how they had not felt the need to test for other STI as they had perceived other STIs to be less severe as HIV, attributing this lowered sense of severity to the perception that STIs are generally curable:
IDI01: But, but I think that STIs are milder in a sense than HIV […] So I don’t see any symptoms. Because my main concern was, has always been HIV, I mean… If you get that then everything goes downhill. But if it’s STI, it’s probably curable.
Second, several participants, in contrast to HIV testing, highlighted how testing for other STIs was often costly, which deterred them from testing:
IDI05: I wanted to go for [an STI] test to see if it was actually, or it was a skin condition or anything like that. Yeah… then the cost part like deterred me.
IDI04: I would say do… make the other test more affordable and accessible as well for the non-HIV panel. I would say the panel includes, chlamydia, syphilis, gonorrhoea, as a, all three in one.
HIV self-testing
Consistent with the reported barriers to HIV testing, most participants described two main benefits of the HIVST kit. First, many participants felt that the self-testing kits were convenient:
IDI03: Um… I think most people will be ok with getting it.
I: Why do you say so?
IDI03: It’s like convenient. And it’s pretty easy to use.
Second, participants felt that the HIVST kit accorded individuals more privacy or confidentiality in accessing HIV testing:
IDI20: I think most people would genuinely want to test themselves […] especially because people at anonymous testing are not really anonymous since a lot of the volunteers are also in the gay community and they all know each other.
Pathways to HIV and other STI testing
We developed a conceptual framework in figure 1 based on the barriers and facilitators to HIV and other STI testing, as well as participants’ perceptions of HIVST. This figure illustrates how the introduction of HIVST along, at present, would lead to a potential reduction in clinic-based STI testing that may result from the availability of bundle tests that currently motivate the uptake of other STI alongside HIV testing among GBMSM in the present setting. On the other hand, existing pathways to other STI testing that are precipitated by the motivators mentioned previously will likely not be affected by the introduction of HIVST in the present setting.
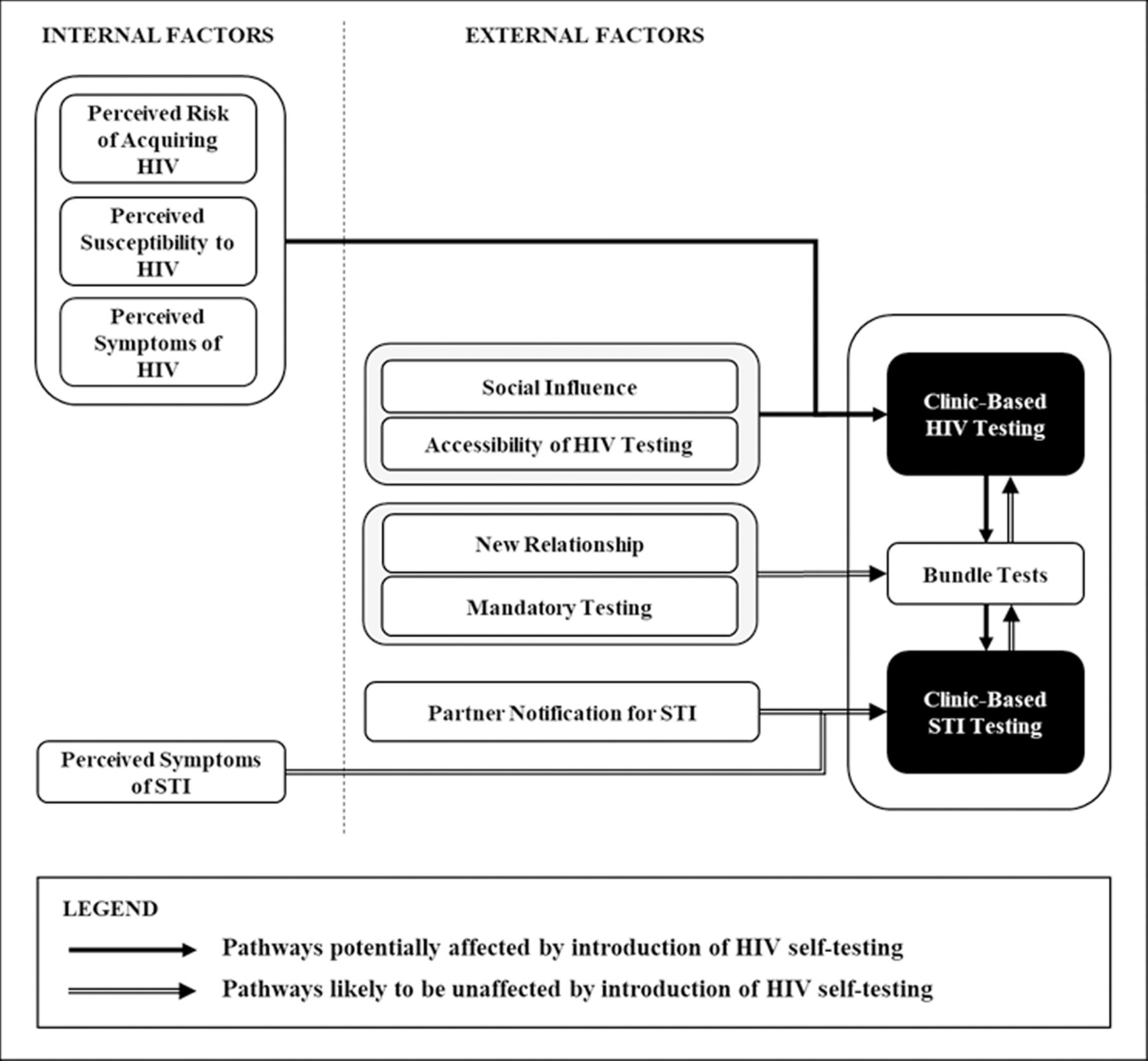
{kind=link}
Pathways to HIV and other STI testing affected by the introduction of HIV self-testing.
Discussion
Participants reported several internal motivators to HIV testing that were less commonly spoken about in the context of other STI testing. These included the perceived risk of acquiring and perceived susceptibility to HIV as GBMSM. These findings are unsurprising, given that other STIs are often perceived to be less serious or severe than HIV among GBMSM.27 Correspondingly, such attitudes can be seen in the social and structural environments that these participants were embedded; participants shared about how their friends had encouraged each other to test for HIV, and that HIV testing services were either free or widely accessible, which was not a perception that was commonly articulated in the context of other STI testing. On the other hand, participants reported only testing for other STI when they had perceived themselves to have symptoms of such STI, or when their past sexual partners had notified them of their own diagnoses. This further validates the perception that GBMSM in the present setting viewed other STIs to be less severe than HIV, such that they would only test for other STIs, given circumstances that placed them at almost certain risk for other STIs. Finally, participants reported several pathways through which they were incentivised to test for both HIV and other STIs simultaneously. These included the availability of bundle tests at facility-based testing sites, mandatory testing or when they were starting new relationships.
Taken in tandem, the results suggest that due to the heightened perceived risk or susceptibility towards HIV as GBMSM, participants correspondingly reported more internal and external factors that motivated HIV testing, which collectively reflected individual, social, and community or structural adaptations to such perceptions of HIV since the start of the epidemic. In contrast, other STI testing were underpinned by factors that illustrated participants’ higher tolerance for other STIs vis-à-vis HIV.
Given the barriers to HIV and other STI testing reported by participants, many participants described how the introduction of HIVST would address certain barriers such as the lack of convenience or confidentiality in facility-based HIV testing. Furthermore, given that different factors may underpin regular or episodic patterns of testing for GBMSM,28 we would expect that the availability of HIVST may provide additional incentives for both regular and episodic testing, especially among GBMSM, who face barriers in accessing facility-based testing.
However, our results also indicate potential knock-on implications for other STI testing, as indicated in figure 1. Participants in this study highlighted how most pathways leading to other STI testing were encountered in situations when there is almost certain risk of acquiring other STI, or when they felt compelled to do so by external factors like mandatory tests or starting new relationships. While they were also incentivised to test for other STIs when they were given the opportunity to do so at facility-based testing sites, alongside testing for HIV in bundled tests, we hypothesise that the introduction of HIVST would potentially reduce such opportunites to do so. While other studies have found that the introduction of HIVST did not lead to a reduction in testing for other STIs,29 we caution that the sociocultural context in Singapore, where GBMSM may be disincentivised to test for HIV and other STI due to stigma, may lead to a different outcome.
We are mindful of several limitations in this study. As participants were recruited through the help community stakeholders, the sample might better reflect the perspectives of GBMSM who have greater engagement with HIV and other STI testing services. While we sought to mitigate this by recruiting participants based on their past HIV and other STI testing behaviours, perspectives among GBMSM who might be less comfortable disclosing their sexual orientation may not be reflected as well in the study, especially since heavy stigma towards GBMSM and HIV prevail in Singapore.15 Furthermore, as participants largely comprised those aged below 30 years old, the findings around perspectives towards HIVST in this study may not typify those of older GBMSM, and should thus be interpreted with this bias in mind. Nonetheless, this study is the first published study on perspectives towards HIVST among GBMSM in Singapore and contributes to the understandings of how HIVST may in fact have negative implications for other STI testing without proper considerations around the existing pathways to testing.
In sum, the findings of this study suggest that the introduction of HIVST might weaken linkages to clinic-based STI testing if alternative strategies of promoting other STI testing are not simultaneously rolled out, such as the development and roll-out of STI self-testing through rapid diagnostic tests instead of the prevailing self-sampling kits, as well as other incentives to STI testing. While this present study cannot establish the magnitude of such an impact that HIVST would have on clinic-based STI testing, our findings nonetheless suggest that HIVST should be implemented with corresponding interventions that address such emerging gaps to testing for other STIs as well. This is especially important, given the rising incidence of syphilis in various settings and antimicrobial-resistant gonococcal infections, which may lead to severe health problems if left undetected, and especially if such infections remain asymptomatic for certain individuals.30 31 We recommend that future interventions attempt to address both the risks of HIV and other STIs simultaneously, and that structural interventions which promote HIV and other STI prevention be balanced accordingly.
Key messages
We conducted a qualitative study comprising in-depth interviews with 30 gay, bisexual and other men who have sex with men (GBMSM) in Singapore.
We explored the potential impact that HIV self-testing (HIVST) would have on HIV and other STI testing among GBMSM.
We delineated the barriers and facilitators to HIV and other STI testing, as well as perceptions towards HIVST among GBMSM in Singapore.
Given existing testing patterns, we found that introducing HIVST might weaken linkages to clinic-based STI testing if alternative strategies of promoting STI testing are not simultaneously rolled out.
Data availability statement
Data are available upon reasonable request. Data are available upon reasonable request from the corresponding author.
Ethics statements
Ethics approval
Ethical approval was obtained from the National Healthcare Group’s Domain Specific Review Board (reference number 2014/00586).
Acknowledgments
The study team would like to thank all the participants who participated in the study. This study was funded by Ministry of Education - Singapore (Grant number: R-608-000-072-112). This publication was supported by National Centre for Infectious Diseases (NCID).
References
Footnotes
Handling editor Adam Huw Bourne
Contributors RKJT: data curation; formal analysis; writing, original draft; writing, review and editing; visualisation. YYC: formal analysis; data curation; writing, review and editing; project administration. MABI: formal analysis; data curation; writing, review and editing; project administration. LPH: resources; writing, review and editing; visualisation. OZL: investigation; resources; formal analysis; data curation; writing, review and editing; project administration. BCHC: investigation; resources; formal analysis; data curation; writing, review and editing; project administration. MT-WC: resources; writing, review and editing; supervision; funding acquisition. MI-CC: conceptualisation; writing, review and editing; supervision; funding acquisition; project administration. CMW: conceptualisation; methodology; formal analysis; data curation; writing, review and editing; supervision; funding acquisition; project administration.
Funding This study was funded by Ministry of Education - Singapore (Grant number: R-608-000-072-112).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.