Article Text

Abstract
Objectives A novel long-acting regimen (LAR) of cabotegravir and rilpivirine for HIV treatment requires dosing every 2 months instead of daily. We assessed what proportion of people living with HIV and physicians would be interested in trying and offering LAR respectively and why.
Methods 688 people living with HIV on treatment, and 120 HIV physicians completed web-based surveys in Germany, Italy, the UK and France during 2019. Balanced description of a hypothetical LAR regarding efficacy, administration and possible side effects were provided. The hypothetical long-acting injections were assumed to be cost-neutral to current daily oral antiretrovirals. Interest of people living with HIV in trying (‘very’/’highly’) and physicians’ willingness to offer (‘definitely’/’probably’) this LAR in different situations, with perceived benefits/concerns was measured.
Results Of people living with HIV, 65.8% were interested in trying LAR. The majority (~80%–90%) of those with unmet needs felt LAR would help, including those with strong medical needs (malabsorption and interfering gastrointestinal conditions), suboptimal adherence, confidentiality/privacy concerns and emotional burden of daily dosing. Of physicians, percentage willing to offer LAR varied situationally: strong medical need (dysphagia, 93.3%; malabsorption, 91.6%; interfering gastrointestinal issues, 90.0%; central nervous system disorders, 87.5%); suboptimal adherence (84.2%); confidentiality/privacy concerns (hiding medications, 86.6%) and convenience/lifestyle (84.2%). People living with HIV liked LAR for not having to carry pills when travelling (56.3%); physicians liked the increased patient contact (54.2%). Furthermore, 50.0% of people living with HIV perceived LAR would minimise transmission risk and improve their sexual health. The most disliked attribute was scheduling appointments (37.2%) and resource constraints (57.5%) for people living with HIV and physicians, respectively. Physicians estimated 25.7% of their patients would actually switch.
Conclusion Providers and people living with HIV viewed the described LAR as addressing several unmet needs. Alternative treatment routes and especially LAR may improve adherence and quality of life.
- adherence
- AIDS
- therapy
- treatment
- patients views
Data availability statement
Data are available on reasonable request. Requests should be directed to the corresponding author for consideration.
Statistics from Altmetric.com
Introduction
Improvements in antiretroviral therapy (ART) have helped reduce HIV-related mortality substantially.1 2 Suppression of HIV replication in people living with HIV is associated with lack of transmission to uninfected persons.3 Sustained HIV suppression is however contingent on optimal adherence to ART and requires consistent daily oral dosing which may be challenging for individuals with certain medical conditions/comorbidities, pill fatigue, inconvenient dosing schedules or confidentiality concerns.1 2 4 Confidentiality concerns often result from HIV-related stigma, a factor that may cause some people living with HIV to keep their HIV status secret which in turn may result in ART doses being missed, especially in settings where there is perceived risk of unwanted disclosure of HIV status.5 6
Most people living with HIV are very aware of the benefits of having an undetectable viral load and when this is not attainable for whatever reason, then this may impact their quality of life (QoL).4 7 Adherence, virological control and QoL among people living with HIV are so tightly intertwined that it is unlikely to achieve the latter without careful consideration of the others.8 9 This paradigm is becoming increasingly recognised in the HIV community as evidenced with the proposed fourth ‘90’ target (improving QoL), which directly incorporates the concerns, values and treatment preferences of people living with HIV.9 Achieving this fourth ‘90’ target calls for, in part, flexible treatment options beyond daily oral dosing—the current sole option. To help address unmet treatment needs, an injectable long-acting regimen (LAR) of cabotegravir (CAB) and rilpivirine (RPV) has been developed. Results from clinical trials that compared this regimen with continued daily oral therapy demonstrated non-inferiority.10 11 Studies also showed that the long-acting injectable treatment was well accepted and tolerated.12 With this new treatment, people living with HIV would receive a dual intramuscular long-acting injection every 2 months, instead of 365 days of oral dosing. The treatment is indicated for people living with HIV who are virally suppressed, with no resistance to integrase strand transfer inhibitors or non-nucleoside reverse transcriptase inhibitors.
As the implementation of this new LAR requires some adaptations in the clinic in terms of service delivery,13 14 data are needed to evaluate the potential number of people living with HIV who would be interested in LAR. Awareness, interest, evaluation, trial and adoption are the five steps through which diffusion and uptake of any innovation occurs.15 These five steps may be orchestrated by patient-provider communication, underlying medical factors as well as perceived benefits and concerns. To understand these issues better in relation to LAR, this study sought to answer the following three questions: (1) What are the prevalence and determinants of interest in trying this new treatment among people living with HIV, and why (benefits and concerns)? (2) What factors are associated with healthcare professional (HCP) willingness to offer this new treatment to their patients and why (benfits and concerns)? (3) Considering both medical needs and patients’ preferences, what percentage of patients are expected to actually switch to this new treatment?
Methods
Survey administration
This study was conducted from June to August 2019 in Germany, Italy, the UK and France. Participants comprised 120 (pooled) board-certified or board-eligible physicians with ≥5 years of practice as an internist or HIV/infectious disease specialist, and 698 people living with HIV (pooled, n=688 on ART) with confirmed HIV status. The design of the survey instrument followed standard methodology starting with qualitative open interviews to identify concepts of interest; we also performed discrete choice experiment to further validate the treatment attributes associated with unmet needs among people living with HIV. In addition, a key patient group (European AIDS Treatment Group) was involved in the review of the questionnaire to ensure the questions were unambiguous, the framing was relevant and the questionnaire overall was of appropriate length. All feedback and suggestions received on the wording or placement of questions were integrated in the final questionnaire. Finally, to ensure that what we intended to measure from the survey was what was being actually captured from respondents, we performed cognitive testing with a sample of people living with HIV before fielding the final survey. The HCP questionnaire comprised 33 items and the survey of people living with HIV, 60; each item was analysed independently.
HCPs were recruited from existing panels predominantly comprising physicians with larger caseloads of HIV+ patients. People living with HIV were recruited using a mix of approaches including existing panels of HIV+ patients (60%–70% of sample), supplemented with active recruitment of confirmed people living with HIV from patient service organisation and social media platforms. The panels from which HCPs and people living with HIV were recruited were independently maintained by third-party research organisations (Liberating Research, Opinion Health, Sermo, Ipsos and Medefield).16 To minimise bias, there was double blinding: the study sponsor (ViiV Healthcare) was not identified to participants and participants’ identities likewise were not revealed to ViiV Healthcare. Participants were however told the study was being conducted ‘on behalf of a pharmaceutical company’. On completion of the questionnaire, respondents were remunerated for their participation (approximately £20). Recruitment was closely monitored to ensure that the demographic characteristics of the sampled participants reflected the national distribution of all people living with HIV in the respective countries.
Study variables related to LAR (‘regimen Z’)
Both surveys (physicians and people living with HIV) referred to CAB+RPV LAR treatment as ‘regimen Z’, which was described as ‘a hypothetical new product for treating HIV infection’ (online supplemental table 1). In brief, each survey had a preamble that provided relevant facts (from clinical trials) as well as a few assumptions to orient the respondents about the long-acting treatment, including information on the route (‘injectable regimen’), frequency (‘every 2 months’), settings (‘given by a nurse, doctor or other healthcare professional’), effectiveness (‘as effective at keeping patients undetectable as other HIV treatments’), possible injection site reactions (‘mild pain’; ‘soreness’, which ‘typically lasts 3 days or less’) and assumed cost (‘at similar cost to you compared with your current treatment’).
Supplemental material
‘Level of interest in trying’ among people living with HIV
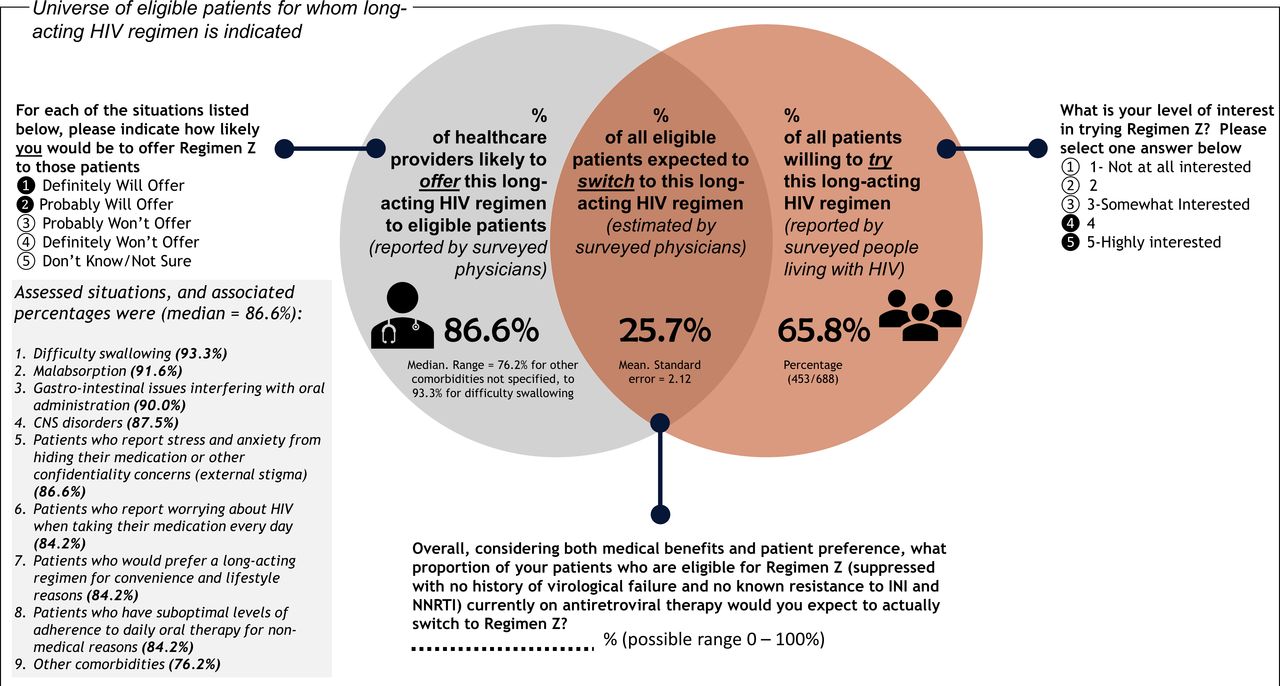
‘Level of interest in trying regimen Z’ was assessed on an ordinal scale of increasing interest, from 1 to 5; we recoded this variable as 1 (strong interest: scores ≥4), or 0 (absence of strong interest, scores 1–3) (figure 1). Participants further indicated what attributes they liked the most and their top concerns with the treatment. Those who reported specific unmet needs (medical needs, adherence barriers, confidentiality concerns and emotional challenges) were further asked if they thought LAR could help them.
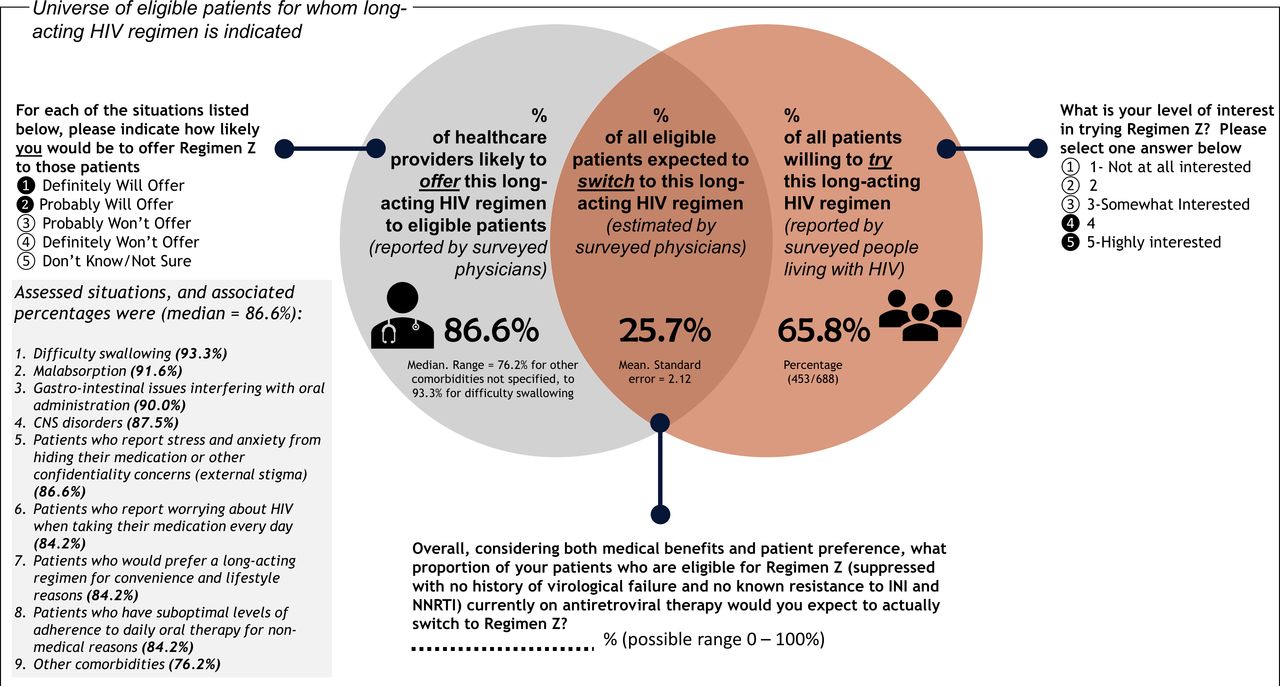
Attitudes towards long-acting HIV treatment among surveyed people living with HIV on antiretroviral treatment (n=688) and HIV physicians (n=120), 2019.
Various emotional challenges were assessed, including adherence anxiety, perception that daily oral ART was disruptive/stressful and concerns about long-term negative impacts of ART. We have previously reported the prevalence of these specific challenges16; in this paper however, we were interested in examining how interest in LAR varied by the presence or absence of these emotional challenges.
Level of interest ‘to offer’ among HCPs
Physicians were presented with several categories of patient needs, and for each situation, asked to ‘please indicate how likely [they] would be to offer regimen Z to those patients’. The situations were: (1) ‘malabsorption’, (2) ‘difficulty swallowing’, (3) ‘gastrointestinal issues interfering with oral administration’, (4) ‘central nervous system (CNS) disorders’, (5) ‘suboptimal levels of adherence to daily oral therapy (50%–90%) for non-medical reasons’, (6) ‘for patients who report stress and anxiety from hiding their medication or other confidentiality concerns’, (7) ‘for patients who report worrying about HIV when taking their medication every day’, (8) ‘for patients who would prefer a LAR for convenience and lifestyle reasons’.
For each situation, HCPs indicating they ‘definitely will offer’ or ‘probably will offer’ were classified as being willing to offer the new treatment to their patients.
HCP estimate of how many of their eligible patients would ‘actually switch’
HCPs were asked:
‘Overall, considering both medical benefits and patient preference, what proportion of your patients who are eligible for Regimen Z (suppressed with no history of virological failure and no known resistance to Integrase Strand Inhibitors and Non-nucleoside Reverse Transcriptase Inhibitors) currently on antiretroviral therapy would you expect to actually switch to Regimen Z?’ Possible response options ranged from 0% to 100%.
Sociodemographic characteristics and other covariates
Among people living with HIV, other variables assessed included gender, sexual orientation, current relationship status, education, employment, domicile, current age, age at diagnosis and country of origin. Among HCPs, information was collected on gender, primary medical specialty, primary practice setting, primary practice location, current staff grade, years of experience as well as number and profile of managed patients with HIV.
Analyses
We estimated the following: (1) percentage of people living with HIV interested in trying LAR (among all on ART, n=688); (2) percentage of HCPs willing to offer LAR for each unmet need assessed (among all HCPs, n=120); (3) the percentage of their patients that HCPs estimated would actually switch to the new treatment, considering both medical benefits and patients’ preferences. Analyses further examined perceived benefits and concerns relative to the new treatment. Differences in proportions were assessed with χ2 test at p<0.05. Using exploratory logistic regression, we further examined which clinical and demographic factors were associated with interest in trying LAR adjusting for age, country and gender. Factors associated with HCP-reported estimate of what proportion of all their eligible patients are expected to actually switch to the new treatment (count variable, percentage points) were explored using Poisson regression, adjusting for years of practice, country and gender. Analyses were conducted with R V.3.6.1.
Results
HCPs reported managing a median (IQR) of 300 (150–400) patients, of whom 90% (80–98) were currently on ART (online supplemental table 2). Among all surveyed people living with HIV, mean (SD) age was 43.9 (11.0) years and 99.0% (688/698) were currently on ART.
Supplemental material
Perspective of people living with HIV on ART: level of interest in trying LAR
Overall, 65.8% were strongly interested in trying LAR assuming it was priced similar to current oral ART (table 1). Within bivariate analyses, interest in trying LAR differed by sexual orientation and age, but not by education.
Overall and stratified percentages of people living with HIV on treatment who reported being interested in trying a novel long-acting HIV treatment (n=688)
The majority (~80%–90%) of those with unmet needs felt LAR would help them with those issues, including those with strong medical needs (malabsorption and interfering gastrointestinal conditions). Others with specific unmet needs who felt LAR would help them with those issues included those with suboptimal adherence, 80.5% (301/374); those with confidentiality/privacy concerns, 87.6% (458/523) and those with emotional burden from taking pills every day, 79.0% (240/304).
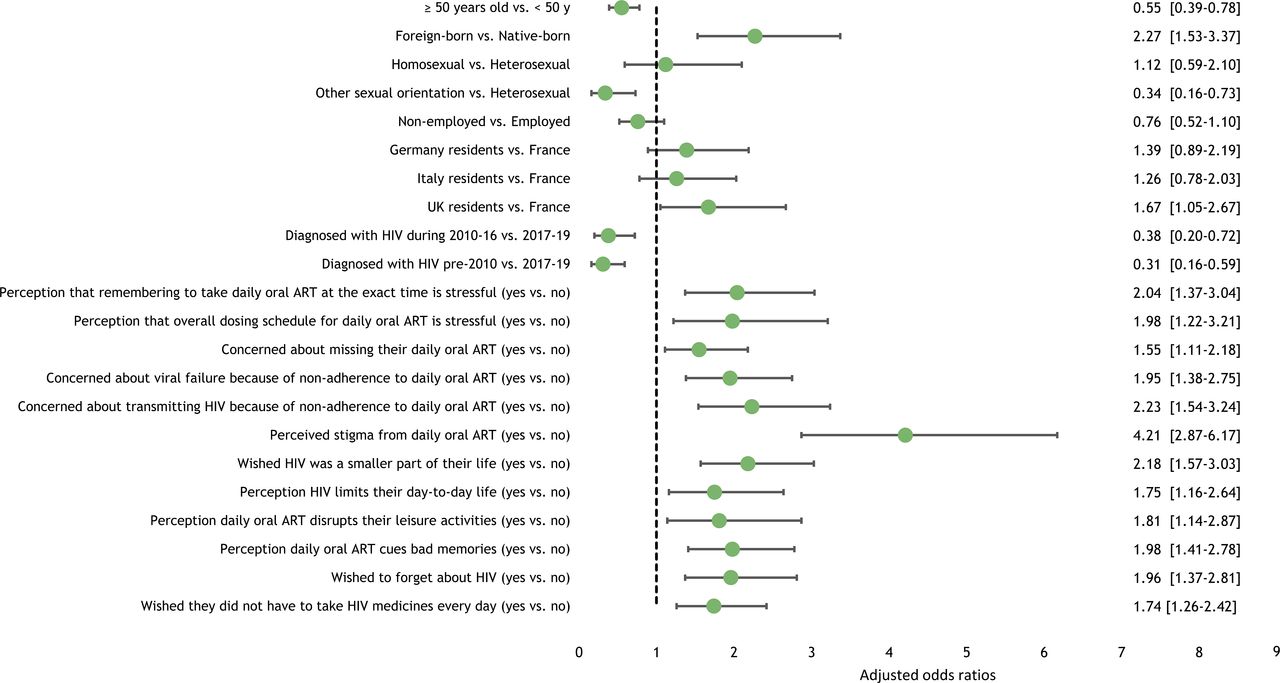
Odds of being interested in trying LAR were 4.21 times higher among those reporting versus not reporting that taking their HIV treatment less often “would reduce the shame or stigma I feel for having HIV” (95% CI 2.87 to 6.17) (figure 2). Furthermore, compared with those not reporting the following concerns, interest in trying was significantly higher among those reporting that they were: stressed by their daily oral dosing schedule (adjusted OR (AOR) 2.04, 95% CI 1.37 to 3.04); concerned about missing a dose (AOR 1.55, 95% CI 1.11 to 2.18), afraid of experiencing virological failure from missing a dose (AOR 1.95, 95% CI 1.38 to 2.75), worried of transmitting HIV from missing a dose (AOR 2.23; 95% CI 1.54 to 3.24) or wishing HIV was a smaller part of their life (AOR 2.18; 95% CI 1.57 to 3.03). Odds of being interested in trying were 2.27 higher among the foreign-born versus native-born (95% CI 1.53 to 3.37). Conversely, odds of being interested in trying were lower among those ≥50 years old than those aged <50 years old (AOR 0.55; 95% CI 0.39 to 0.78), and those diagnosed during 2010–16 (AOR 0.38; 95% CI 0.20 to 0.72) or pre-2010 (AOR 0.31; 95% CI 0.16 to 0.59) versus during 2017–19. Current ART type was not associated with interest in trying LAR.
{kind=link}
{kind=link}
Multivariable logistic regression analyses of factors associated with interest in trying a long-acting HIV treatment among surveyed people living with HIV on antiretroviral treatment (ART) (n=688), 2019. Note: because of collinearity, each independent variable was analysed separately, adjusting for age, gender and country of residence.
The most liked attributes of LAR among people living with HIV were increased ease of travel because of not having to take HIV medication on trips (56.3%); 2-month uninterrupted drug efficacy (56.0%); reduced frequency of medication intake (52.9%); no risk of missing a dose, which minimises the risk of treatment failure (51.3%) or of HIV transmission (50.0%) (online supplemental figure 1). Drawbacks however included having to schedule appointments (37.2%) and injection pain (35.3%).
Supplemental material
HCP perspective: likelihood to offer LAR and estimated percentage of patients that would switch
Of HCPs, the percentage willing to offer LAR was as follows for the following situations: strong medical need (dysphagia, 93.3%; malabsorption, 91.6%; interfering gastrointestinal issues, 90.0%, CNS disorders, 87.5%); confidentiality/privacy concerns (hiding medications, 86.6%); suboptimal adherence (84.2%) and convenience/lifestyle (84.2%) (figure 2, online supplemental figure 2).
Supplemental material
HCPs reported several perceived benefits and concerns with the new treatment. While most liked the opportunity for more patient contact (54.2%), they were also concerned about the resource implications from increased patient visits (57.5%). Besides the general population of patients, HCPs perceived the new treatment would benefit those with multimorbidity (25.0%), and those at higher risk of transmitting disease (eg, unprotected sex workers and recreational drug users, 16.7%).
Of all their eligible patients, the proportion that HCPs expected to switch, considering both medical benefits and patients’ preferences, was 25.7% (figure 1). Within multivariable analyses, HCP-estimated number of patients that would actually switch was higher among male than female HCPs (incidence rate ratio [IRR] 1.25, 95% CI 1.16 to 1.36), and among registrars/associates than consultants/professors (IRR 1.30; 95% CI 1.18 to 1.43) (table 2). Also, HCPs reporting a higher (>10%) patient burden for the following conditions, were likely to estimate more of their patients actually switching, than those with ≤10% of patients with the indicated condition: malabsorption (IRR 1.38; 95% CI 1.27 to 1.50), dysphagia (IRR 1.20; 95% CI 1.11 to 1.31), interfering gastrointestinal issues (IRR 1.24; 95% CI 1.15 to 1.34) and CNS disorders (IRR 1.60; 95% CI 1.48 to 1.74). Conversely, lower estimates of patients expected to actually switch were reported by HCPs with high patient loads between 220 and 350 (IRR 0.80; 95% CI 0.73 to 0.87), or >350 patients (IRR 0.75, 95% CI 0.68 to 0.83) versus those with <220 patients. Compared with HCPs in academic/specialist institutions, estimated number of patients was lower among those in general hospitals (IRR 0.68, 95% CI 0.58 to 0.80) or other settings (IRR 0.71, 95% CI 0.63 to 0.80). HCPs in smaller towns (IRR 0.84, 95% CI 0.77 to 0.91) estimated lower number of patients that would actually switch than those in metropolitan areas. Compared with HCPs in France, lower expected switching numbers were estimated by HCPs in Italy (IRR 0.85, 95% CI 0.77 to 0.94) and the UK (IRR 0.58, 95% CI 0.52 to 0.65). HCPs who saw a larger share (≥20%) of non-European patients with HIV estimated a lower number of their patients would actually switch than those who saw predominantly European patients (IRR 0.80, 95% CI 0.72 to 0.88).
Healthcare providers’ best estimate of how many of their patients would switch to a novel long-acting HIV treatment (n=120), 2019
Discussion
The three main findings from this study were: (1) 65.8% of people living with HIV on ART were interested in trying LAR assuming it was priced similar to current oral ART. Participants felt the treatment would help with malabsorption, interfering gastrointestinal conditions, suboptimal adherence, confidentiality/privacy concerns and emotional burden from daily dosing. Interest in trying LAR was not associated with specific ART regimens, indicating that LAR may not necessarily replace one type of regimen in particular but rather may come from across the range of current therapies. (2) HCPs believed that the described LAR could provide benefits to their patients and were willing to offer LAR to patients under varying medical and non-medical situations. Taken across a range of assessed situations of patient unmet needs, the median percentage for HCP willingness to offer LAR to those patients was 86.6%. (3) HCPs estimated that 25.7% of their patients would likely switch to LAR, considering both medical benefits and patients’ preferences. Significantly higher estimates of patients expected to switch to LAR were reported by HCPs with fewer patients in care, those who were metropolitan based, male HCPs and more junior HCPs. While the most liked attribute of LAR among people living with HIV was that it made travelling easier from not having to carry along pills, HCPs highly favoured the opportunity for increased patient contact.
Some of the LAR-related concerns reported by HCPs revolved around resource allocation and the logistics of scheduling, administering and tracking patients. Consistent with the observation that the greatest concern regarding LAR among HCPs was resource-related, we found that HCPs with larger patient loads, those in smaller healthcare facilities or in smaller towns, all estimated fewer of their patients actually switching to LAR. These HCP concerns need to be addressed using implementation science frameworks drawing on lessons from injectable drug routines for other medical conditions. Key issues include optimal communication strategies, logistics, human resource planning, evaluation metrics and integration into health systems.13 17 Addressing these issues will open a window for ‘customizable’ ART treatment to fit the lives of people living with HIV.18
Many people living with HIV comfortably manage their daily oral dosing and may even feel empowered by daily oral dosing in that it reassures them that their viral load is being kept under control.19 Yet, for others, alternatives to daily oral dosing may improve adherence and quality of life. Our previous analyses showed that of the current study population, 23.7% felt daily oral dosing limited their daily life; 27.3% reported they found their daily oral dosing stressful, 40.1% were worried about missing their daily doses and half (50.3%) wished HIV treatment was a smaller part of their life.16 Such emotional, psychosocial and lifestyle constraints/unmet needs are leading causes of non-adherence among people living with HIV4 and should be considered when planning to start or switch treatments. LARs provide an option for providers to help people living with HIV who are either unwilling or unable to take oral tablets for a variety of medical or non-medical reasons. Ensuring holistic care is critical, especially within the context of polypharmacy20 as well as to accelerate progress towards targets for eliminating AIDS as a global threat and achieving the AIDS response target of the Sustainable Development Goals.21–25
Some limitations exist to this study. First, the data are cross-sectional and only associations can be drawn. Second, despite efforts to ensure the sampled population resembled the target population during the sampling stage, the findings may not be fully generalisable because of the web-based survey administration and the non-probabilistic sampling. Third, there may be measurement bias (overestimation or underestimation) as some questions were framed in a non-neutral manner, which might make one answer more likely than another.
Conclusion
Of people living with HIV on ART, 65.8% were interested in using LAR assuming it was priced like current oral ART. HCPs estimated that of their eligible patients, 25.7% would switch to LAR, considering both medical needs and patients’ preferences. HCPs gave more weight to potential role of the medication in filling medical reasons for suboptimal adherence whereas people living with HIV strongly considered QoL. Both people living with HIV and HCPs viewed LAR as the solution for a series of unmet needs. Providing LAR among people living with HIV can increase choice, improve quality of life and limit transmission risk.
Key messages
Of people living with HIV, 65.8% were very/highly interested in trying long-acting regimen for HIV treatment assuming the long-acting regimens were priced similar to current antiretroviral therapy.
Of their eligible patients, physicians estimated that 25.7% would actually switch to the described long-acting regimen, considering both medical needs and patients’ preferences.
The majority (~80%–90%) of those with unmet needs felt long-acting regimens would help, including those with strong medical needs (malabsorption and interfering gastrointestinal conditions), suboptimal adherence, confidentiality/privacy concerns and emotional burden of daily dosing.
Also, 50.0% of people living with HIV perceived that long-acting regimen would minimise transmission risk and improve their sexual health.
Of physicians, the percentage indicating they will offer long-acting regimen, by type of unmet need, was: strong medical need (dysphagia, 93.3%; malabsorption, 91.6%; interfering gastrointestinal issues, 90.0%, central nervous system disorders, 87.5%); suboptimal adherence (84.2%); confidentiality/privacy concerns (hiding medications, 86.6%) and convenience/lifestyle (84.2%).
Interest in trying a long-acting HIV regimen was highest among younger aged people living with HIV <50 years (69.8%), those recently diagnosed with HIV during 2017-2019 (84.1%), those with perceived stigma from their daily oral ART (83.3%) and those stressed by their daily dosing schedule with oral ART (78.0%).
Data availability statement
Data are available on reasonable request. Requests should be directed to the corresponding author for consideration.
Ethics statements
Patient consent for publication
Ethics approval
This study was deemed exempt research by the Pearl Institutional Review Board (Study number 19-IPSO-125). All participants provided informed consent.
Acknowledgments
The authors would like to thank Zatum for statistical analysis and helping in medical writing.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Anna Maria Geretti
Contributors NV conceptualised the study. All authors contributed to study design, analyses, drafting of the manuscript and substantial revisions. All authors gave final approval for the manuscript to be submitted.
Funding This work was supported by ViiV Healthcare.
Competing interests The following coauthors are employees of ViiV Healthcare or GSK: JS, MB, PR, FV, LR, GN, LF, VC and NVdeV.
Provenance and peer review Not commissioned; externally peer reviewed.