Article Text

Statistics from Altmetric.com
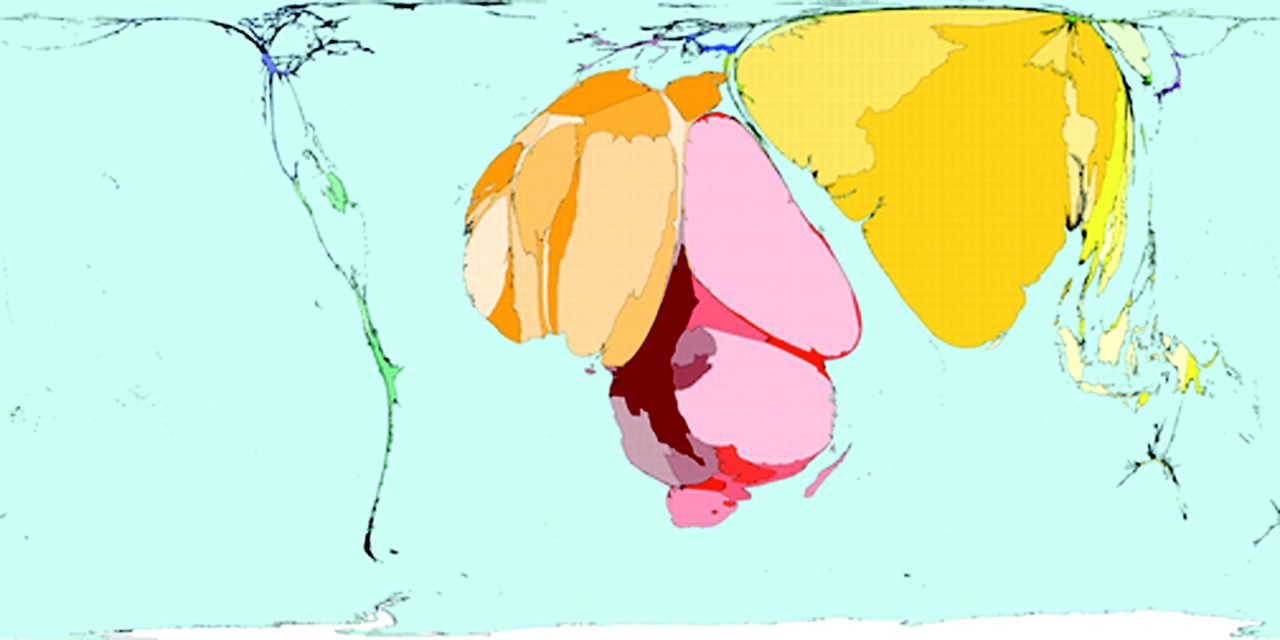
An overwhelming majority of the global burden of morbidity and mortality caused by sexually transmitted infections (STI) and HIV is borne by the world’s poorest countries (fig 1). In a world increasingly “shrunk” by modern communications, what are the common issues preoccupying the international community of researchers in our field? In planning this themed issue, published on World AIDS Day 2007, we sought papers on all topics of global relevance: migration, international travel, the extent and impact of antiretroviral rollout programmes, and wide-reaching strategies for the prevention of STI and HIV transmission. We took the opportunity to seek out international diversity in STI and HIV research. Despite our intention to travel far afield, we have found ourselves closer to home than we had hoped, in respect of the authorship, and ownership of the diversity of studies relating to the populations of the world’s poorer countries. Our 13 original articles include 9 studies conducted in the countries of sub-Saharan Africa,1–6 south and south east Asia,7,8 Latin America,9 and 4 in Europe.10–13 The provenance of the articles, however, does not reflect their scope (fig 2); the e-mail addresses of corresponding authors of seven of these papers are in the United Kingdom,1,5,8,10,12,13 and another five are in the United States, Canada and Australia.2,4,6,7,9 on exploring this further, we found that the pattern of the published content was not the result of the selective acceptance of papers authored from the north; we saw the same pattern in papers that were rejected. Neither is ours an isolated experience. In the six leading tropical medicine journals in 2002, 12.5% of the first and 9.4% of the last authors came from countries with the lowest human development indices (usually poor) compared with 50.6% and 58.8% from high human development index (usually rich) countries.14 Within the increasingly global research community, it is essential that local research capacity is developed in its fullest form. This means that opportunities must be created for local scientists to be full and active partners in the design, analysis, interpretation and presentation of STI and HIV research with a view to the ownership of research by those whose own destiny lies within those countries.14

World map of the distribution of authors of scientific papers. Territory size shows the proportion of all scientific papers published in 2001 written by authors living there. Source: http://www.worldmapper.org/display.php?selected=205. Reproduced with permission.
The control of HIV infection, and the reduction of associated morbidity in severely affected countries is a major theme. Boulle and Ford15 from South Africa give an overview of the benefits and challenges of scaling up antiretroviral therapy in resource-poor settings. Encouragingly, they cite some evidence that in South Africa and Brazil death rates and AIDS-related hospital admissions are decreasing at a population level. Vaginal microbicides are a hotly pursued option for HIV prevention, but the failures and closures of clinical trials, despite extensive safety testing, have dampened enthusiasm recently. Martin Hilber and colleagues16 suggest that the missing link is a proper understanding of the role of women’s use of vaginal products and practices to tighten, dry, warm and clean their vaginas. The goal, they say, is to achieve a safer vaginal environment.
The new global strategy of the World Health Organization (WHO) for the prevention and control of STI17 is summarised by Lewis and colleagues.18 It lists the components of comprehensive STI case management, including correct diagnosis, effective treatment, and condom promotion. The need for new technologies to contribute to STI control is further developed by Jones et al,2 who show in a randomised controlled trial, that allowing women in Gugulethu, South Africa, to take specimens for STI at home and mail them to the laboratory is a feasible and acceptable alternative to going to a clinic. In the same vein, Romoren et al.3 used decision analysis to show that the use of point of care tests for diagnosis and azithromycin for treatment of chlamydia could improve the management of chlamydia in pregnant women, but would cost an additional US$38 per case cured. Although systematic review of the evidence for the effectiveness of condom promotion interventions in Africa and Asia supports the WHO strategy, Foss and colleagues10 also draw attention to the need for better evaluation designs using biological outcomes. In practice, levels of risk-taking behaviour remain high and condom use low, as O’Farrell et al1 show in a study of men attending an STI clinic in Durban, South Africa.
An immediate priority of the WHO strategy is the implementation of targeted interventions against STI and HIV in high-risk and vulnerable populations. The Avahan Project is a US$258 million complex HIV prevention intervention aimed at sex workers and drug users in the six most heavily affected states in India. Boily and colleagues8 describe a novel approach to evaluating the effects of this programme in sex workers. They will collect STI, HIV and behavioural data over time from intervention areas and use mathematical models to predict what would have happened to the HIV epidemic in the absence of the intervention. There will be no quick answer though; the evaluation will take over seven years.
The potential of voluntary testing and counselling is also explored. Arthur et al5 observed some reduction in risk behaviours of 401 people interviewed six months after an HIV test in Kenya, but only 55% of those testing HIV positive disclosed the result to their partner. The benefits of an HIV test in sex workers in Senegal are even less clear, because women who had had an HIV test in the past were less likely to use condoms with their regular partners.6 Prost et al13 conducted focus groups with Africans living in London and concluded that a voluntary counselling and testing approach used in health centres in Kenya could be feasible in the United Kingdom. Promoting HIV testing among Africans in the United Kingdom would certainly be worthwhile. Sadler et al12 report a prevalence of 14% in a community-based survey of 1359 adults from sub-Saharan Africa, of whom 66% were unaware of their infection.
Finally, Mercer et al11 explored the potential of travel for disease transmission, showing that HIV prevention advice in the United Kingdom needs to be targeted to Britons travelling abroad as well as to migrants arriving from high-prevalence HIV countries. Analysis of the second National Survey of Sexual Attitudes and Lifestyles shows that a substantial minority of young single adults reports sex abroad, with its associated risks.
As Peter Piot said in his recent interview with STI, “it is important that young people enter [STI research] because there is still so much work to be done.”19 We hope that this collection of articles contributes to global and local efforts for the prevention and control of STI and HIV to provide a safer sexual environment for all.
{kind=link}
{kind=link}
World map of distribution of deaths due to STI. Territories are sized in proportion to the absolute number of people who died from STI other than HIV in one year. Source://www.worldmapper.org/display_extra.php?selected=375. Reproduced with permission.
REFERENCES
Footnotes
-
We thank Professor Danny Dorling for alerting us to the map used in figure 2, and for permission to reproduce these.