Article Text

Abstract
Objective: To examine the quality of HIV sero-surveillance systems in countries by 2002, as well as trends between 1995 and 2002.
Methods: The quality of countries’ surveillance systems was scored for five years: 1995, 1997, 1999, 2001, and 2002. Sero-surveillance data were compiled from the US Census Bureau’s HIV/AIDS Surveillance Database, the EuroHIV database, and from countries’ national HIV surveillance reports that were available to WHO/UNAIDS. The quality of systems was scored according to the level of the countries’ epidemic.
Results: There has been a large variation in the quality of HIV surveillance systems across the 132 countries by type of the epidemic and over time from 1995 to 2002. Over the 1995–2002 period the number of countries with a fully implemented system decreased from 57 (43%) in 1995 to 48 (36%) in 2002. The proportion of countries with a fully implemented system was 58%, 34%, and 10% in countries with a generalised, concentrated, and low level epidemic, respectively. In the 53 countries with generalised epidemics the number of countries with a fully implemented system increased from 24 (45%) in 2001 to 31 (58%) in 2002.
Conclusion: Many countries still have poor functioning HIV surveillance systems and require urgent strengthening. Countries should monitor and evaluate their own HIV surveillance systems and examine whether the systems are appropriate and adequate.
- MSM, men who have sex with men
- sero-surveillance
- HIV infection
- trends
- HIV estimates
Statistics from Altmetric.com
HIV surveillance constitutes a core function of national AIDS programmes worldwide. Surveillance data on HIV infection is important for numerous reasons, but most importantly to track the spread of HIV both within different populations in countries as well as across different geographic regions.1 Since 2000, UNAIDS and WHO have promoted the second generation surveillance framework.2 This more strategic approach to surveillance aims to improve understanding of the epidemic through the collection of information from different sources, including the spread of HIV infection and other STIs, risk behaviours, morbidity, and mortality. The second generation surveillance framework also aims to tailor surveillance systems to the countries’ type of epidemic. Ultimately, second generation surveillance aims to contribute to an improved response to the epidemic based on an improved analysis of surveillance data from a variety of sources. Information generated by second generation surveillance systems also allows better understanding of HIV dynamics and provides information to evaluate the impact of past and current HIV/AIDS programmes.
Countries’ HIV/AIDS surveillance systems have evolved over time. Most countries have initiated a sentinel HIV sero-surveillance component to study the distribution of infection among different populations and geographically, and to monitor trends in levels of infection over time. The analysis of trends in HIV sero-prevalence data over time is key to understanding the dynamics of the epidemic, but depends on the availability of sero-prevalence data collected repeatedly from the same sites. An analysis of HIV sero-surveillance systems through 1999 suggested that the quality of HIV sero-surveillance varied considerably across countries.3 Although the majority of countries most affected by HIV/AIDS had systems that could provide sufficient data for tracking the epidemic and making reasonable estimates of HIV prevalence, many countries had poor functioning systems.
In the past few years more resources have become available to countries, from a variety of sources including their own national budgets, the Global Fund for AIDS, Tuberculosis and Malaria (GFATM), the World Bank’s Multi-Country HIV/AIDS Program project, and bilateral sources, for their response to the HIV/AIDS epidemic. This increase in resources will place increased demands on monitoring and evaluation systems, including information generated by surveillance systems. HIV sentinel sero-surveillance data are a major building block for deriving national estimates of prevalence of HIV infection.4,5 The quality of the sero-surveillance data will determine the certainty of those estimates.
This paper examines the quality of HIV sero-surveillance systems in 132 low and middle income countries in 2002, as well as trends between 1995 and 2002.
METHODS
Data sources
An overall database of HIV surveillance data was developed by combining information from four sources. Data on HIV sero-surveillance were retrieved from the HIV/AIDS surveillance database developed by the United States Census Bureau.6 Data for countries in Europe came from a database maintained by the European Centre for the Epidemiological Monitoring of AIDS.7 These data were combined with national HIV surveillance reports that were available to WHO and UNAIDS. Finally, countries that had conducted a nationally representative population based survey including HIV prevalence had those data included in the overall surveillance database for review. We excluded high income countries from this analysis.
Defining appropriate HIV sero-surveillance
The definition of appropriate HIV sero-surveillance was based on the recommendations of the UNAIDS/WHO Working Group on Global HIV/AIDS and STI Surveillance.2 The epidemic state determines which data from which population groups will be most useful. Countries were classified as having low level, concentrated, and generalised epidemics based on the available surveillance data and/or previous estimates. In generalised epidemics (with a numerical proxy of HIV sero-prevalence being consistently over 1% among antenatal clinical attendees), HIV sero-surveillance should be conducted among pregnant women in urban and rural sites. In concentrated epidemics (with a numerical proxy of HIV sero-prevalence being below 1% among pregnant women but over 5% among populations with high risk behaviours) HIV sero-surveillance should be conducted among populations at higher risk of HIV and among pregnant women in major cities. For this analysis, injecting drug users (IDUs), female sex workers, men who have sex with men (MSM), and STI clinic attendees were considered appropriate populations at higher risk of HIV. Finally, in low level epidemics (with a numerical proxy of HIV sero-prevalence being below 5% among populations with high risk behaviour), HIV sero-surveillance is recommended only among groups at higher risk.
Defining the quality of sentinel surveillance systems over time
A coding scheme to represent the quality of the system was adapted from previous work on quality of surveillance.3 Like that work, this paper used four dimensions to capture the quality of surveillance systems. These dimensions were:
-
frequency and timeliness of data collection
-
appropriateness of populations under surveillance
-
consistency of the sites/locations and groups measured over time
-
coverage/representativeness of the groups for the adult populations (either groups at highest risk or general adult population).
Coding was done for alternating years between 1995 and 2002, that is for 1995, 1997, 1999, 2001, and 2002. The last 2 years were only 1 year apart, to allow inclusion of the most recent data.
Countries with generalised epidemics
Frequency and timeliness
The scoring for frequency and timeliness was a simple arithmetic operation. The number of times surveillance data had been collected was counted in the five year period preceding the year to be coded (range 0–5). As a measure of timeliness, countries that collected surveillance data in the last 2 years of this five year period were given a score of 1, those without data for the last 2 years of the five year period were given a score of 0. The sum of the two scores (range 0–6) was used as the overall measure of frequency and timeliness. In addition, for 44 countries in sub-Saharan Africa, the number of countries that had conducted a round of surveillance among pregnant women in each year between 1985 and 2002 was counted.
Appropriateness
An appropriate system was defined as one in which data had been collected in urban and rural sites for pregnant women and from at least one high risk group in the last 2 years. Countries with an appropriate system were scored as 1, all others were scored as 0. The appropriateness measure was based on the last round of surveillance data collected.
Consistency
A judgement about the consistency of data was made by reviewing the sites for pregnant women. The scoring judgement was made on a three point scale (0–2), with a score of 0 representing no pattern of consistency in urban and rural surveillance sites. A score of 2 was given if there was a clear pattern of repeating sites over each data collection cycle in both urban and rural areas. This does not mean that all sites had to be repeated because in many countries new sites are added over time, or in some cases groups of rural sites are alternated between data collection cycles. A score of 1 was awarded when there was some repetition of sites in either urban or rural areas, providing some trend information.
Coverage
The coverage scoring was based on a judgement of the likelihood that the surveillance sites provide results for a representative sample of pregnant women. Two pieces of data were used to make this judgement. Firstly, sites were organised as being either in urban or rural areas in the countries. Secondly, the ratio of the number of antenatal sites per million population was also reviewed to help make the judgement of coverage. As with the judgement of consistency, scores were given on a three point scale (0–2), with 0 representing very poor coverage, 1 representing fair coverage, and 2 representing coverage that included a good sample of sites in both urban and rural areas.
Overall quality of the sentinel surveillance systems
The overall quality of the surveillance system was the combination of the scores for each of the four dimensions. The sum of these four dimensions had a range from 0–11. The countries were then ranked based on the quality score. This distribution was reviewed to help determine categories of quality. Three categories were used. To be characterised as a fully implemented system, the system had to be judged to provide timely and consistent data that came from the appropriate populations and provided fairly representative data. The countries in this category had a total score of 8 or more. Countries’ surveillance systems were characterised as partially implemented if they had some of the features of a high quality system, but not all. For many countries, the weakness in the system was the timeliness of data collection. For others it was poor coverage or consistency. For countries in this category some data were available to track the epidemic, but improvements are needed. Countries were placed in the medium category when the total scores ranged 5–7. The poorly or non-functioning surveillance system category was applied to all other countries. In reviewing data for these countries, none was judged to have a system that produced even the basic information needed to track the epidemic.
Countries with concentrated and low level epidemics
Scoring surveillance system quality for countries with low level or concentrated epidemics focused on systems generating information from groups at higher risk of HIV infection. The same four dimensions as for generalised epidemics, that is frequency and timeliness, appropriateness, consistency, and coverage, were used as the basis of the coding system.
Scoring surveillance system quality
In categorising the quality of surveillance systems for countries with low level and concentrated epidemics, the four dimensions of quality were scored in slightly different ways compared with generalised epidemics. Frequency and timeliness were again captured as the number of times sero-surveillance data had been collected in the five year period preceding the year to be scored. Appropriateness and coverage were combined and defined by which populations had been under surveillance. In low level and concentrated epidemics it is not necessary to have full geographic coverage, as high risk groups are often concentrated in urban areas. Therefore, both appropriateness and coverage were defined by the groups from which data had been collected. For countries with low level epidemics, data should be collected from all groups at highest risk for infection. In all countries this includes sex workers, MSM, and attendees of STI clinics because it was assumed that these groups are present in all countries. In addition, where significant injecting drug use is present in a country there should be surveillance among this population as well. For countries with concentrated epidemics, there should also be surveillance among pregnant women in urban areas. For countries with concentrated epidemics to get the highest score on coverage (2), at least three higher risk groups and pregnant women in urban areas would have to be included in surveillance. For a score of 1, the countries surveillance system must include at least three groups, two of which must be from the three core higher risk groups of sex workers, MSM, or IDUs. All other countries received a score of 0 for coverage. Consistency was again judged by reviewing the sites (for each population) over time. Again, the judgements were performed through joint review. A three point scale was used to judge consistency, with 2 given for consistent use of data sources, 1 for those with some consistency, and 0 for those with no or very little consistency. For countries with low level epidemics the scoring procedure was the same except that data from pregnant women was not required for appropriate coverage.
The combined scores from the surveillance systems in countries with low level or concentrated epidemic ranged 0–10. Countries with combined scores of 8 or better were rated as having fully implemented sero-surveillance systems. Countries with a combined score of 4–7 were rated as partially implemented systems, and all other countries rates as having poor or non-functioning systems.
India and China
Because these two countries have very large populations of over one billion each, as well as variation in the level of the epidemic in the different states and provinces, a decentralised approach was used. Each state and province was scored separately, with the Indian states of Andrah Pradesh, Karnataka, Maharashtra, and Tamil Nadu being scored as generalised epidemics. Scores for each state and province were then weighted by population to arrive at a summary score for the country. The summary scores for these two countries were then used to judge overall quality of the surveillance systems, with a score of 8 or above rates as fully implemented, scores of 4–7 as partially implemented, and a score of 3 or less as poor or non-functioning systems.
RESULTS
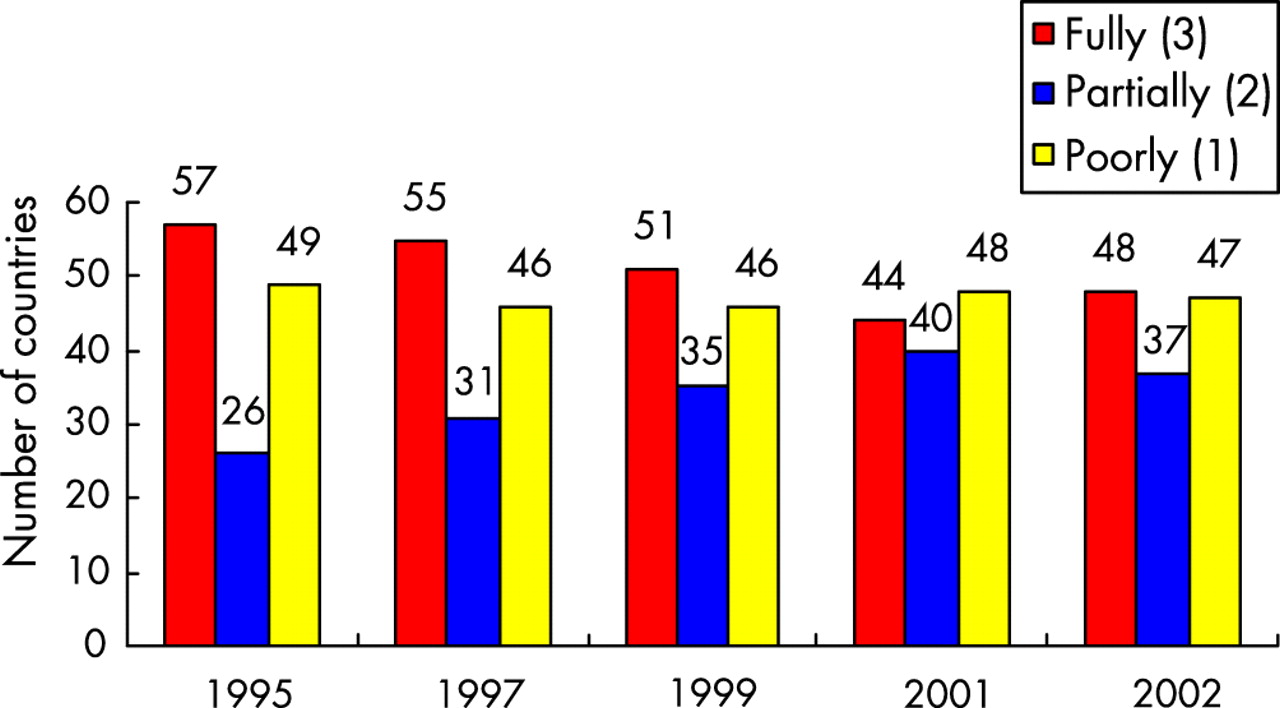
In the 1995–2002 period there has been a large variation in the quality of HIV surveillance systems between countries and over time (see table 1). During the early 1990s most of the countries have developed HIV surveillance systems, with 57 (43%) of them having fully implemented systems by 1995 (see fig 1). However, over the 1995–2002 period, there has been a decline in the quality of HIV sero-surveillance, with only 48 countries (36%) having fully implemented systems by 2002. The number of countries that have poorly functioning systems has remained relatively constant with between 46 and 49 countries in that category over the study period.
Quality of HIV sero-surveillance systems in low and middle income countries with generalised, concentrated, or low level epidemics, 1995–2002

: Trends in the number of countries with fully and partially implemented, and poorly or non-functioning, sero-surveillance systems in 132 countries, 1995–2002.
Generalised epidemics
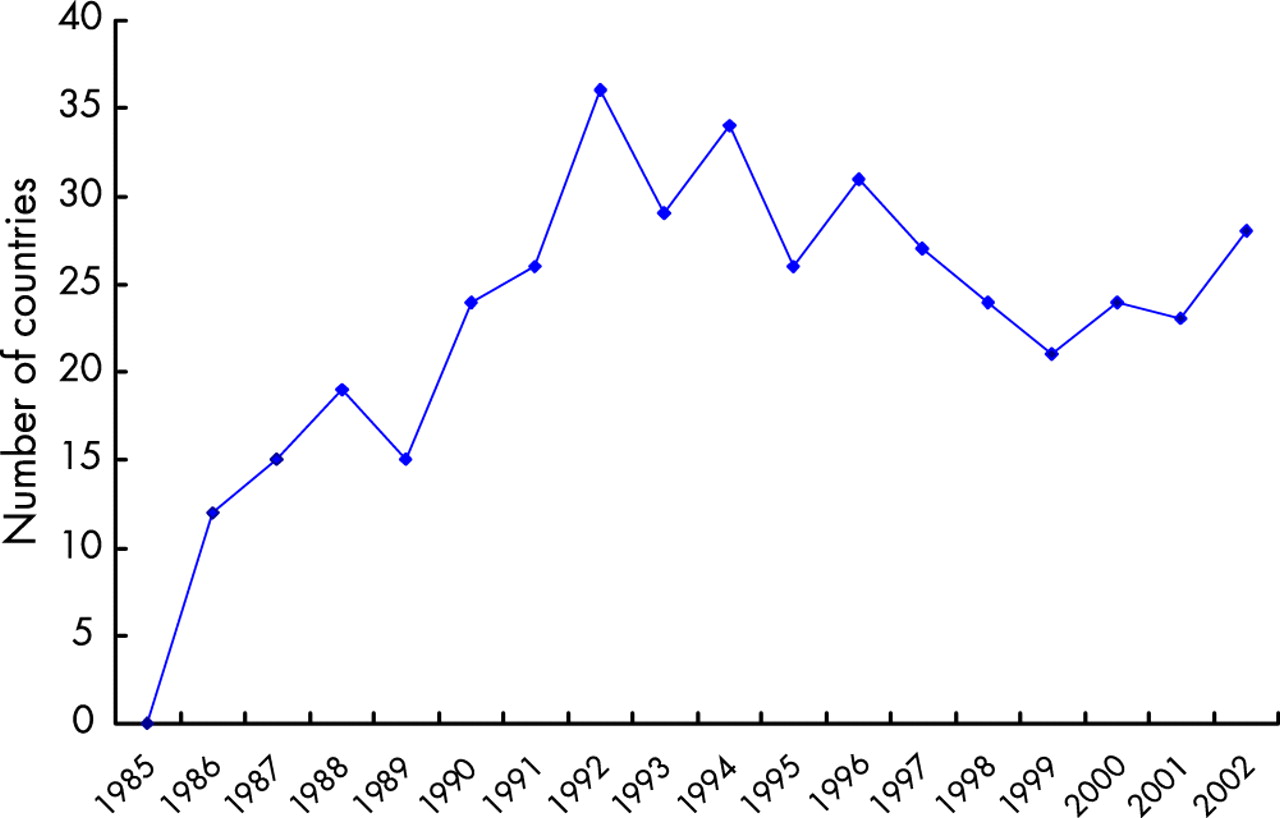
Following a decline in the late 1990s, the 53 countries with generalised epidemics have recently improved their HIV surveillance systems with the number of countries with fully implemented systems increasing from 24 (45%) in 2001 to 31 (58%) in 2002 (see fig 2). However, the number of countries with poorly or non-functioning systems increased from 4 to 9. In addition to their sentinel surveillance activities, eight countries have recently conducted national household surveys that have measured HIV prevalence: Burundi, Dominican Republic, Kenya, Mali, Niger, South Africa, Zambia, and Zimbabwe. Fig 3 shows the number of countries in sub-Saharan Africa that conducted a round of sero-surveillance among pregnant women in each year between 1985 and 2002. The number increased rapidly starting in 1996 to a high 36 in 1992, then declined to a low of 21 in 1999, and increased again to 28 in 2002.

Trends in the number of countries with fully and partially implemented, and poorly or non-functioning, sero-surveillance systems in countries with a generalised epidemic, 1995–2002.

Trend in the annual number of countries in sub-Saharan Africa that conducted sero-surveillance among pregnant women, 1985–2002.
Concentrated epidemics
Over the 1995–2002 period, out of 29 countries, the number of countries with fully implemented sero-surveillance systems remained stable, ranging 10–13. Over the same period the number of countries with poorly or non-functioning systems decreased from 9 to 5 (fig 4).

Trends in the number of countries with fully and partially implemented, and poorly or non-functioning, sero-surveillance systems in countries with a concentrated epidemic, 1995–2002.
Low level epidemics
Among 48 countries with low levels of HIV infection only five presented fully implemented systems in 2002, down from 10 in 1999. Over the period the number of countries with poorly or non-functioning systems ranged 32–35 (fig 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Trends in the number of countries with fully and partially implemented, and poorly or non-functioning sero-surveillance, systems in countries with a low level epidemic, 1995–2002.
DISCUSSION
The current review of countries’ sero-surveillance systems indicates a large variation in the quality of these systems as of 2002, across the different types of epidemic. The review also indicates an overall declining trend in the quality over the 1995–2002 period. However, there are signs of a reversal of that trend in the most recent period in countries with generalised epidemics.
It is clear that the countries with generalised epidemics perform better than those with concentrated and low level epidemics: in 2002 the proportion with fully implemented systems was 58%, 34%, and 10% for countries with generalised, concentrated, and low level epidemics, respectively. Also, sero-surveillance systems are of higher quality in countries with a high HIV burden: the 31 countries with a generalised epidemic that had a fully implemented system in 2002 represent 74% of the global HIV burden. It is reassuring that many of the high burden countries are well prepared to track trends over time in their epidemic. Conversely, it is of great concern that most countries with low level epidemics do not have an appropriate surveillance system in place that could serve as early warning in case of growth in the epidemic.
Many resource constrained countries have depended heavily on external resources to finance their HIV surveillance systems. It is likely that a significant proportion of countries with fully implemented sero-surveillance systems up to the mid-1990s had benefited from international interest in tracking of the novel HIV infection with, for example, WHO’s Global Programme on AIDS (GPA) providing important amounts of resources in support of surveillance activities. The number of countries with a fully implemented system with a generalised epidemic declined steadily since 1995 and reached a low in 2001. Since the measure of frequency relates to the past 5 years, this may well be an effect of the disappearance of GPA in 1995. Many of the countries with poorly or non-functioning systems have been unable to build these systems because of long term political strife. In the past few years there has been renewed international interest and support for surveillance from multilateral and bilateral international agencies, for example, among others, the US Centers for Disease Control and Prevention’s Global AIDS Program (http://www.cdc.gov), the UNAIDS/WHO’s second generation surveillance project (http://www.who.int/hiv/strategic/surveillance/en), and the World Bank (http://www.worldbank.org/afr/aids/map.htm). The present analysis identifies countries with poorly or non-functioning systems where efforts for strengthening HIV surveillance should be focused, and for many countries external support may be a crucial part of these efforts.
For countries with generalised epidemics, national population based surveys that have included testing for HIV were included in the scoring of the quality of sero-surveillance systems, regardless of the quality of those surveys. These surveys are potentially an important source of sero-prevalence data, including distribution by gender, age group, and geographic entity, and they can be used to calibrate the data from sentinel surveillance systems. However, the quality of national population based surveys has varied. National surveys with high non-response rates overall or in specific population groups have only limited value in calibrating HIV prevalence estimates derived from sentinel surveillance.8 In these and future surveys, the monitoring of the level of non-response and its determinants is extremely important, in addition to the quality of the sampling, interview, and specimen collection and testing.
HIV sero-surveillance systems in countries with concentrated and low level epidemics are clearly of lesser quality than in countries with a generalised epidemic. HIV surveillance systems in countries with concentrated epidemics are essential to monitor HIV trends among population groups that have higher exposure to HIV and the possible network that can disseminate HIV among other populations. For countries with low levels of HIV infection, sero-surveillance systems are in part warning systems, which will allow detection of any rise in prevalence among groups at high risk of HIV infection. Appropriate surveillance systems for population groups at high risk of HIV infection present additional challenges to those in generalised epidemics. While sero-surveillance among attendees of antenatal clinics and STI clinics is facility based, HIV sero-surveillance for other groups, including IDUs, MSM, or sex workers presents additional challenges related to access to these communities.9 It takes political will and appropriate methods to successfully establish surveillance among these population groups.
UNAIDS and WHO have published HIV estimates at global, regional, and country levels since 1998.10–13 These estimates have been based on the information collected by HIV sero-surveillance systems. The quality and quantity of the HIV prevalence data generated by sero-surveillance systems are major determinants of the precision of those estimates. The improvement in the quality of surveillance systems in the past few years in countries with generalised epidemics is expected to contribute to HIV estimates of higher quality and improved precision. In addition, the end of 2003 estimates have used the present analysis of the quality of HIV sero-surveillance for the construction of ranges of certainty around the estimates of people living with HIV/AIDS, new HIV infections, and AIDS mortality,14 as described in the accompanying paper.15
The current analysis presents a number of limitations. Firstly, while efforts were made to include all available information, it is inevitable that for some countries the information used may have been incomplete, resulting in a lower score. Secondly, although the quality of laboratory testing for HIV antibodies is a crucial element of the quality of sero-surveillance,16 it was not part of the scoring criteria because insufficient information was available. Thirdly, countries were categorised according to standard international definitions but the reality is that many countries may have diverse HIV epidemics in different geographical regions, many countries may be borderline with elements of two categories of HIV epidemics, and, finally, countries may change from one category to another over time. Finally, some of the countries with concentrated or low level epidemics and strong health systems may have sufficient data to track the status and trend of the epidemic if their HIV case reporting system is of sufficient quality and if individuals at high risk of HIV infection make regular use of HIV testing.
CONCLUSION
The quality of HIV sero-surveillance varies considerably among regions and epidemic states and over time. Overall HIV surveillance in countries has been declining in the 1995–2002 period, but there is some improvement in countries with generalised epidemics in recent years. Many countries still have poorly functioning systems and require urgent strengthening. Analysis of the quality of surveillance is an important tool both for evaluating the quality of HIV/AIDS estimates and for prioritising country support. Countries should monitor and evaluate their own HIV surveillance systems, examine if the systems are appropriate and adequate, and modify them according to their evolving needs.
Acknowledgments
We wish to express our appreciation to the national HIV/AIDS programmes in countries that have made their data available. We would also like to acknowledge the work of the staff of the regional and country offices of WHO and UNAIDS for their work in compiling data on HIV/AIDS surveillance. Finally, our appreciation goes to the European Centre for the Epidemiological Monitoring of AIDS and the United States Census Bureau for creating and maintaining databases on HIV/AIDS surveillance.