Article Text

Statistics from Altmetric.com
In 2006, the US Centers for Disease Control and Prevention recommended expanding HIV testing in healthcare settings1 in order to identify the estimated 25% of HIV-infected persons who are unaware of their status and who may be responsible for up to 50% of HIV transmission.2 These recommendations partly attribute the failure of risk-based testing to issues related to access to care and the inability to target testing if individuals do not admit to potentially stigmatising risk behaviours or are unaware of their risk. However, in this issue of Sexually Transmitted Infections, Brown and colleagues3 (see page 4) present data that suggest that the failure of targeted testing may be partly due to missed opportunities for HIV testing in readily identified high-risk populations.
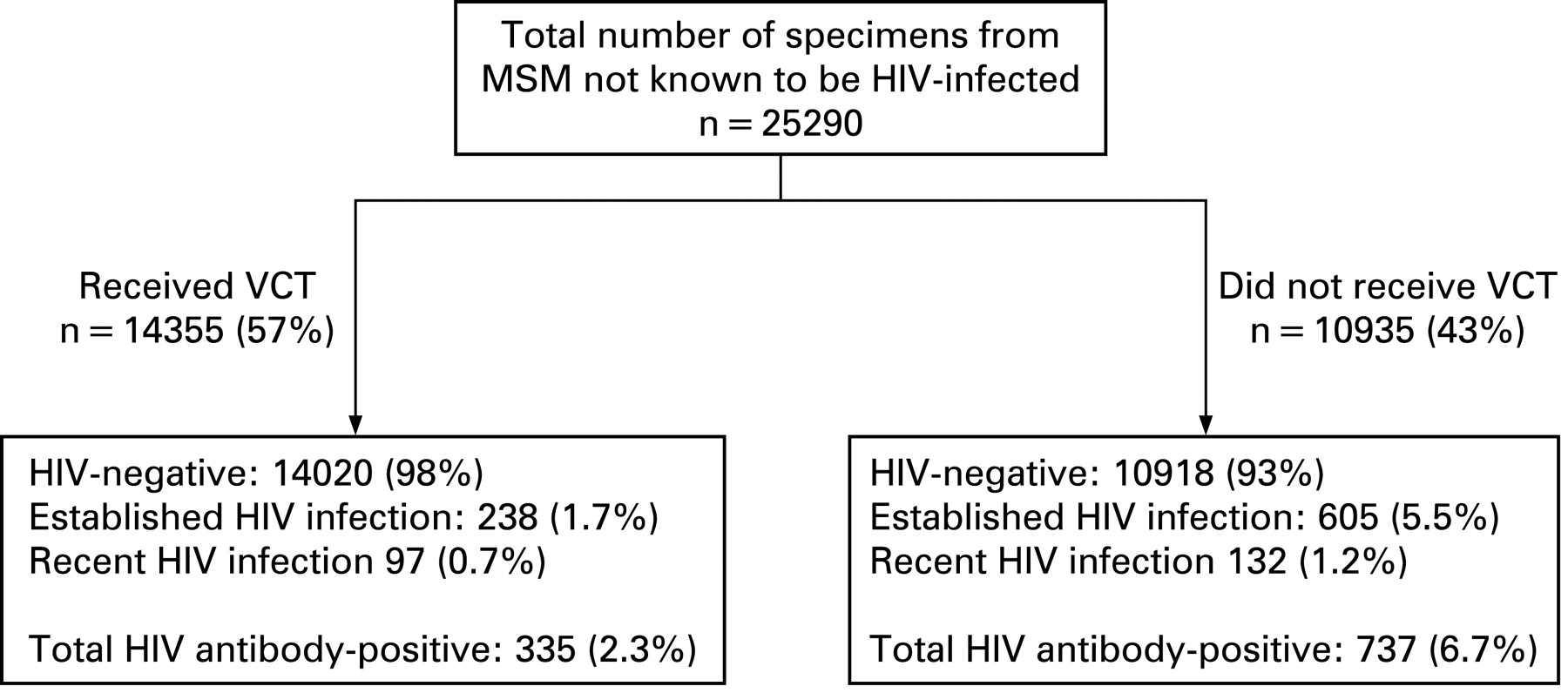
Studying men who have sex with men (MSM) attending 15 genitourinary medicine (GUM) clinics in the UK between 1999 and 2002, the authors detected anti-HIV antibodies in 737 (6.7%) of 10 935 specimens obtained during visits when blood was obtained for syphilis testing but HIV testing did not occur (fig 1). These results are consistent with other published studies, including an anonymous serosurvey conducted at 28 US sexually transmitted disease (STD) clinics in 1997. In nearly all clinics HIV prevalence was 1.4 to 18 times higher among specimens from individuals who were not tested for HIV compared with specimens from individuals who were tested.4 These studies could overestimate the numbers of undiagnosed persons if multiple specimens were obtained from unique individuals during repeat visits or if infected individuals did not acknowledge their HIV status and refused testing. However, it is probably less important to estimate these numbers with precision than to acknowledge that testing is probably inadequate even in venues serving high-risk individuals and to understand why testing was not offered or accepted.

{kind=link}
For established testing programmes, these findings suggest two future objectives: (1) to increase the proportion of patients who are tested when they present for care and (2) to increase the frequency with which high-risk populations access care. The use of rapid antibody testing could increase the uptake of testing5 because patients may prefer rapid testing6 and more testers may receive test results7 8 compared with standard testing. Routinisation of testing through “opt-out” strategies could also increase HIV testing. Individuals attending UK clinics with opt-out testing policies had increased odds (odds ratio 1.59; 95% CI 1.09 to 230, p = 0.02) of being offered an HIV test.9 With opt-out strategies, one review estimated that 71–98% of women received an HIV test during pregnancy, compared with 25–83% in opt-in programmes.10 Additional procedural streamlining, by eliminating written consent requirements11 or delinking counselling and testing, could increase the uptake of HIV testing further.
Some individuals with a recent negative HIV test or risky exposure may be offered but defer testing because of concerns about the antibody-negative “window period”. Are modifications needed to the recommendations to defer testing until 3 months after a potential exposure? Newer antibody assays reduce the window period to 1 month,12 and pooled nucleic acid amplification testing programmes13 shorten it further. The avoidance of testing during primary HIV infection, when individuals are highly infectious,14 is likely to be counterproductive to goals of reducing HIV transmission. In fact, the phylogenetic analysis described by Brown et al3 suggests that transmission from recently infected individuals may have occurred, and similar studies estimate that transmission during primary infection accounts for 25–49% of incidence.15–18 There is a need for more frequent HIV testing in high-risk populations, use of the most sensitive tests and consideration of education programmes designed to teach the symptoms of acute HIV infection. Although these strategies cannot eliminate transmission that occurs within days following HIV acquisition,12 they should decrease the time that HIV-infected individuals are unaware of their status and their potential for transmission.
Fortunately, Brown et al3 highlight a problem that is already being addressed. In UK GUM clinics in 2006, HIV testing was offered to 86% of MSM and testing occurred at 71% of visits.9 Similarly, the Centers for Disease Control and Prevention MSM Surveillance Monitoring Project reported that the proportion of MSM tested for HIV among four STD clinics increased from 49% in 2002 to 61% in 2006.19 In our public health STD clinic in Seattle, MSM not known to be HIV infected received confidential testing during 84% of clinic visits in 2007–8 and others received anonymous testing. We are moving in the right direction.
Our second goal for the future is to leave behind the traditional, passive approach of offering HIV testing to individuals who come to us. Modern technologies such as e-mail, text messaging and other online resources provide the potential for public health to play a more active role in increasing the frequency with which high-risk individuals seek testing. Although these technologies are not well studied to date, reminder and recall systems have been successfully employed to increase vaccination rates.20 21 In the interim, we look to mathematical modellers to inform us of the cost-effectiveness of prompting HIV testing and the ideal frequency of testing.
In the past decade, HIV testing and care services have expanded worldwide. In the UK and USA, more individuals attending GUM/STD clinics are receiving HIV testing and are receiving it more frequently. HIV testing remains one of the sharpest tools in the HIV prevention toolbox. Now we should wield that tool more efficiently. To do so, we should: (1) remove the remaining barriers to testing and move towards “opt-out” strategies; (2) advocate for the routine use of the most sensitive HIV tests, including pooled nucleic acid amplification testing in MSM and other groups with a high HIV incidence and (3) actively strive to increase the frequency of testing among those at highest risk of HIV acquisition. Programmatic research is required to develop and disseminate effective interventions and models to these ends. We still have much work to do to identify less accessible populations at risk of HIV infection, but as Brown et al3 make clear, we could do more to diagnose HIV in individuals identified as high risk who already access care.
REFERENCES
Footnotes
Funding: This work was supported in part by grants from the National Institutes of Health (K23 AI65243) and University of Washington Center for AIDS Research New Investigator Award to JS (AI-27757).
Competing interests: None.