Article Text

Abstract
Background Two randomised controlled trials have recently provided evidence for the efficacy of Pre-Exposure Prophylaxis (PrEP), whereby uninfected individuals use antiretrovirals—either orally or topically—for the prevention of sexual acquisition of HIV. However, the potential population-level impact of a PrEP intervention remains uncertain.
Methods A population-based deterministic mathematical model was developed to investigate the impact of a PrEP intervention in Cotonou, Benin (1.7% adult prevalence in 2006) and Kisumu, Kenya (13.9% adult prevalence in 2008). It was assumed that PrEP has high intrinsic efficacy (90% reduction in acquisition per PrEP protected sex act) but its effectiveness is reduced by imperfect adherence (75% of sex acts are protected for good adherers (40% of PrEP users) and 30% of sex acts are protected for poor adherers (60% of PrEP users)). The impact of prioritising a fixed amount of PrEP with respect to behavioural risk was investigated, whereby 10% of the population received PrEP in each scenario.
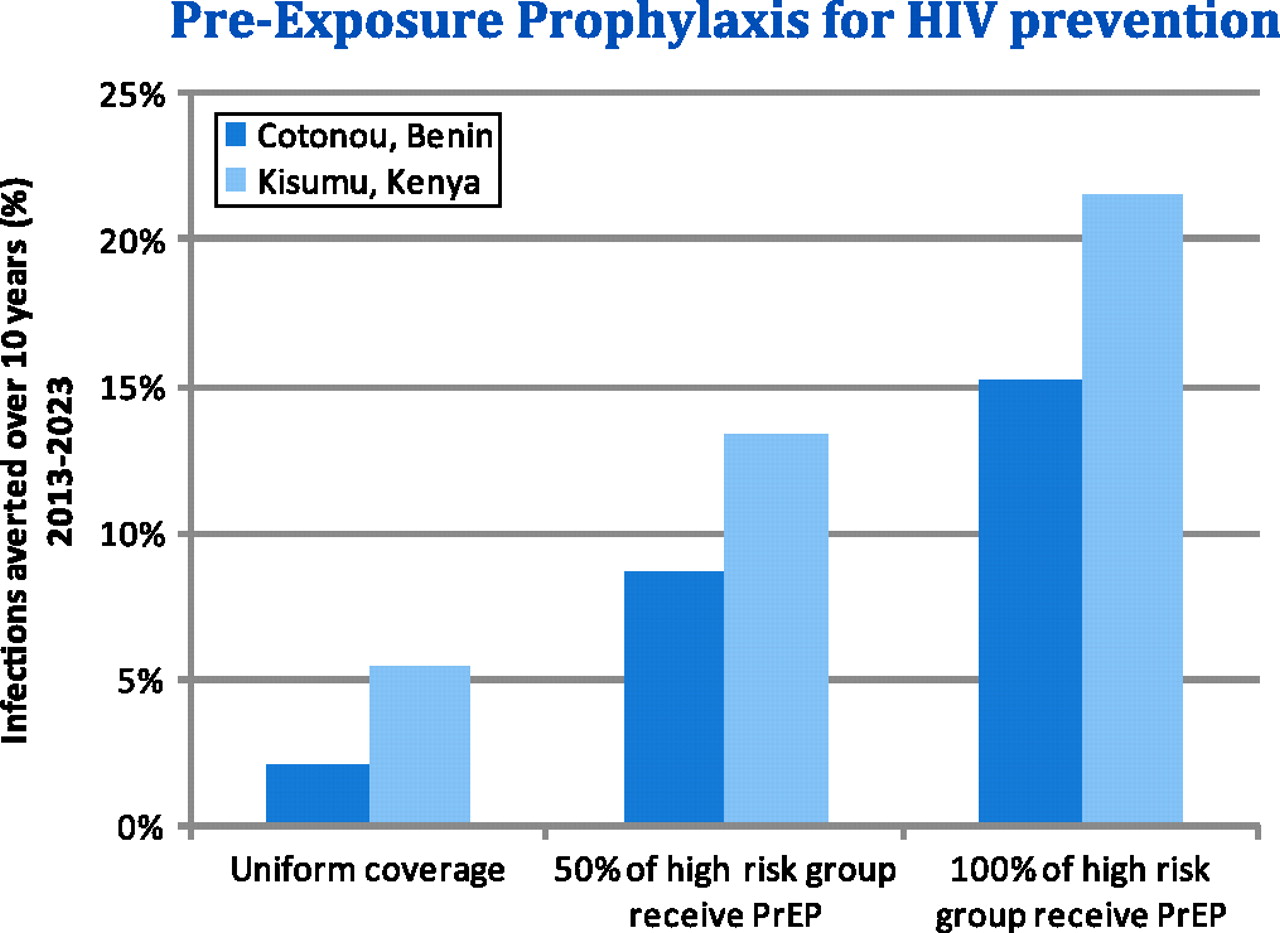
Results In the absence of prioritisation of PrEP, an estimated 2.12% and 5.44% of infections would be averted over 10 years in Cotonou and Kisumu, respectively. However, the population-level epidemiological impact of a PrEP intervention can be substantially increased by prioritising to key populations most at risk of infection (Abstract O1-S06.03 figure 1). Percentage of infections averted over 10 years with respect to different levels of prioritisation by behavioural risk, in Cotonou, Benin and Kisumu, Kenya. The efficiency of increased prioritisation by behavioural risk is greater in Cotonou, as the HIV epidemic is more focussed within identifiable at-risk groups. However, the overall epidemiological impact of the PrEP intervention is greater in Kisumu, which has higher HIV incidence than Cotonou. Assuming an estimated cost range for PrEP of $160–$240 per-person per-year, the estimated cost per infection averted in Kisumu, Kenya, ranges from $13,578 to $20,368, if 50% of high risk individuals receive PrEP and the remaining PrEP is distributed among low and medium risk individuals. These costs should be considered in light of future averted costs of ART provision.
{kind=link}
Percentage of infections averted over 10 years with respect to different levels of prioritisation by behavioural risk, in Cotonou, Benin and Kisumu, Kenya.
Conclusions An effective PrEP intervention could reduce the incidence of HIV transmission in generalised HIV epidemics. Considerable gains in impact, and therefore cost-effectiveness, can be achieved if PrEP is prioritised for those at highest risk of acquisition. Epidemiological context plays an important role in influencing the potential population-level impact of a PrEP intervention.