Article Text

Statistics from Altmetric.com
Introduction
Yearly, an estimated 448 million treatable sexually transmitted infections (STIs)1 occur worldwide. Over 80% of all new HIV infections are acquired through sexual transmission.2 The enormous burden of morbidity and mortality due to STIs impact directly on quality of life, sexual and reproductive health (SRH) and child health, and indirectly as cofactors for HIV transmission. Sexually transmitted diseases such as syphilis, chancroid ulcers and genital herpes simplex virus ulcers greatly increase the risk of acquiring or transmitting HIV and in some cases account for 40% or more of HIV transmissions.3 In addition, STIs are the third most common cause of healthy life years lost by women of reproductive age, exceeded only by maternal causes and HIV.4
The Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund) is one of the largest donors for HIV/AIDS programmes worldwide, and, as of March 2010, the Global Fund has committed US$10.8 billion (Approved Grant Amount) in 140 countries out of US$17.4 billion (Total Lifetime Budget). A recent analysis showed that the Global Fund supports SRH interventions through HIV proposals.5 The financial support provided by the Global Fund is pivotal to countries worldwide, especially those with limited resources to prevent and control the HIV epidemic.
The aim of this analysis was to identify the presence of critical elements that address STI prevention and care in funded Global Fund HIV proposals. The analysis should contribute to a better understanding of how the priorities at country level have evolved since round 1.
Methods
HIV proposals to the Global Fund submitted by countries are complex and multidisciplinary. They comprise issues such as HIV prevention and treatment, education and training on HIV, and contextual social and cultural variables. Therefore our analysis of these proposals took into account these variables and the context in which the interventions mentioned were designed to take place.
Individual Global Fund HIV proposals were screened for the elements of STI prevention and care that are consistent with the public health comprehensive package of STIs.6 The three main areas are: early diagnosis and treatment of STIs; key populations at high risk of infection; and condom promotion and distribution. The early diagnosis and treatment of STIs is vital to the interruption of transmission of STIs as well as to the promotion of quality of life of those infected. Interventions for key populations at high risk of infection are important because, although STI care and prevention is desirable for the general population, targeting more vulnerable groups guarantees a more cost-efficient delivery of services to the populations most in need. Lastly, condom promotion and distribution is critical for the promotion of safer sexual behaviours, as condoms can protect against both infection and unplanned pregnancy.
The analysis was carried out with special focus on section 4 of the proposals, which focuses on planned programmes and interventions, objectives, priorities, service delivery areas and needs mentioned by each country. All proposals were accessed on the website of the Global Fund.7
Results
In total, 345 original HIV proposals submitted to the Global Fund and approved for funding from rounds 1–9 (R1–9) were analysed for elements of STI prevention and care. When more than one proposal existed for the same country in one round, the analyses of the different proposals were integrated into one, resulting in a total of 285 proposals.
Early STI diagnosis and treatment feature as priorities in all funded HIV proposals, with up to 81% (percentages are approximate and rounded to the nearest whole number) of countries for R7 and 94% for R8. In addition, countries such as Jamaica, Kosovo, Kyrgyzstan, Mongolia and West Bank and Gaza mention the specific need for syphilis testing. The proposals by Kosovo, Uganda (R7), Serbia and Chad (R8) also refer to testing for herpes simplex virus 2, while other countries such as Burundi and Indonesia refer to the need for broader screening for Neisseria gonorrhoeae, Trichomonas vaginalis, Chlamydia trachomatis and the human papillomavirus infections.
Syndromic management of STIs, which means treating some common STIs and other non-sexually transmitted reproductive tract infections on the basis of consistent symptoms and signs manifested by specific organisms commonly responsible for each syndrome, especially in settings where laboratory facilities are not available, was included in 37–58% of proposals from R1–7 and increased to over 61% in R8 (figure 1). This percentage decreases to some extent in R9, back to the levels of syndromic management suggested in R7 (42%).
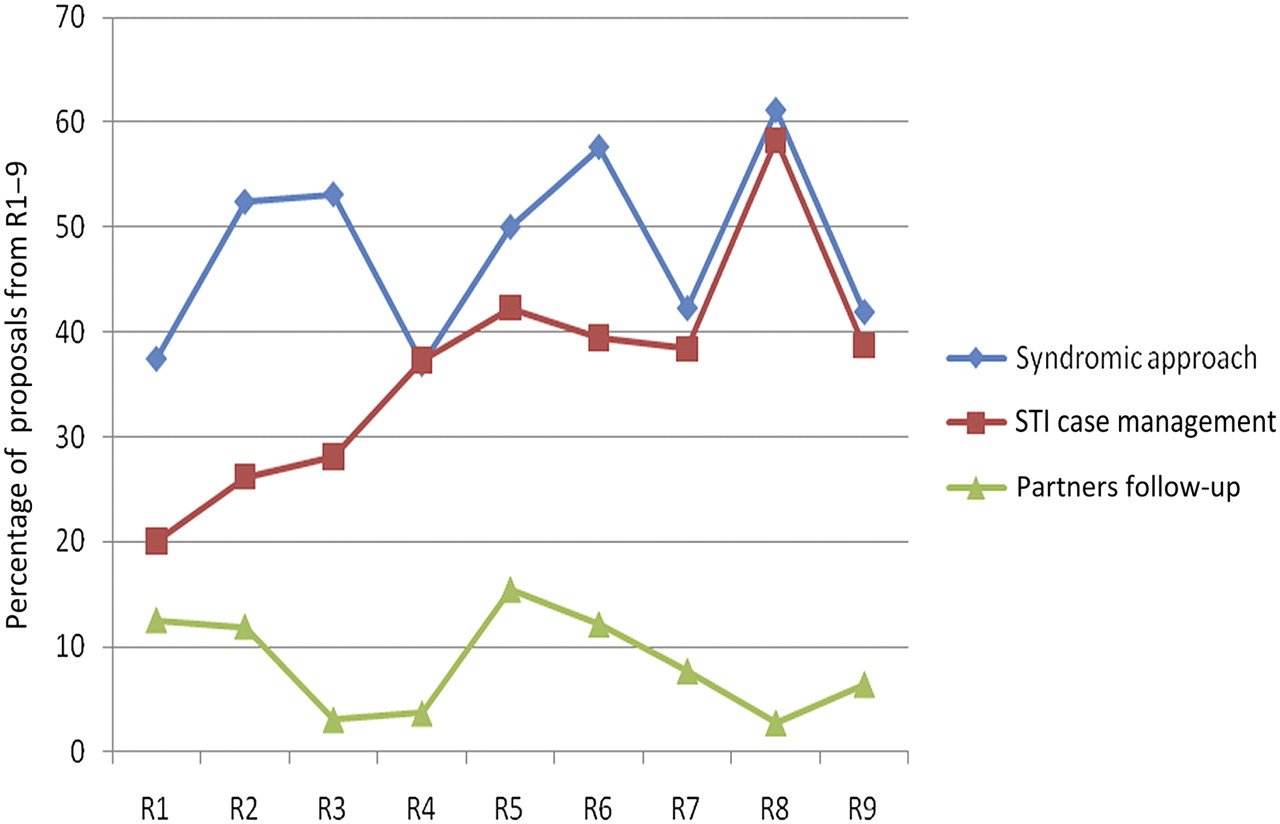
Inclusion of the syndromic approach, sexually transmitted infection (STI) case management, and partner follow-up in proposals from rounds 1–9 (R1–R9).
Management of sexual partners, including the notification, referral and treatment of the partners (who may or may not have symptoms) of patients with STIs is present only in 15% or less of all proposals. For instance, only two countries—Kyrgyzstan and Niger in R7—and one—Gabon in R8—show intention to invest in the follow-up of sexual partners.
Procurement of drugs for the treatment of STIs, as well as educational materials and technical support for healthcare professionals, increased between R1 (around 25–38%) and R8 (61–67%), with a significant decrease in R9, which is undoubtedly not due to disinvestment but a response to the sharp increase between R7 and R8.
Target key populations at high risk of infection (figure 2) vary considerably from country to country, depending on cultural and religious views, social conditions and even political stability. The population most often targeted is sex workers (male and female) followed by young people (both in- and out-of-school), orphans and young children. 'Other' in figure 2 includes populations that were mentioned in a few proposals that were context- and country-specific—for example, disabled people (Burundi, R8), refugees, nomads and displaced populations (Chad, R8), victims of internal and external conflicts (Central African Republic, R7) and gang members (El Salvador, R7).

Vulnerable populations targeted by the Global Fund HIV funded proposals from rounds 1–9 (R1–R9). Unif Men, Uniformed men, including military personnel; Mig workers, Migrant workers; IDU, Injecting drug users; MSM, men who have sex with men; PLWHA, People living with HIV and AIDS.
Men who have sex with men (MSM) are mainly targeted in Asian, Eastern European and South American countries, but largely overlooked in proposals submitted from African countries. Although the total number of proposals that included interventions for MSM is, in general, low, the analysis shows that there is an increasing trend, particularly in R6 and R8 (figure 2).
Over 80% of proposals from R1–9 include the promotion and distribution of male condoms. However, only a small number of countries specifically included procurement of female condoms (the highest 41% in R9) or lubricants (52% in R9) as shown in figure 3.

{kind=link}
{kind=link}
{kind=link}
Condom (male and female) and lubricant promotion and distribution in proposals from rounds 1–9 (R1–R9).
Discussion
STI can lead to chronic diseases, pregnancy complications, infertility, cervical cancer and death, as well as facilitating the transmission of HIV infection. In developing countries, this group of infections and their complications are among the top five reasons that adults seek healthcare. Given the magnitude of the health problems caused by STIs, the benefits of STI prevention and control interventions go beyond HIV prevention.
This analysis of key elements of STI prevention and care from R1 to R9 of funded HIV proposals submitted to the Global Fund shows the first thorough baseline data of opportunities and gaps that exist in including aspects of diagnosis and treatment of STIs. About 77% of all HIV-related proposals include early diagnosis and treatment of STIs, and 48% include syndromic management as key priority interventions. Interventions for the management of sex partners feature little in the proposals (<15% in most cases). This may be a reflection of the practical difficulty of putting such interventions in place or the lack of evidence of cost-effectiveness of such interventions. Further operations research is needed to strengthen evidence and explore effective strategies for reaching and treating sex partners. Although some countries have included targeted interventions, in particular for young people and key populations at high risk of acquiring and transmitting STIs, including sex workers and MSM, the actual interventions are not clearly articulated. For example, there is no specific mention of screening for asymptomatic infection in such populations or the implementation of interventions such as periodic presumptive treatment for sex workers with high rates of STIs and poor access to healthcare, which have been shown to affect the prevalence of STI in such populations.8 Interventions targeting MSM vary considerably by geographical region, being quite low in Africa, which may be a reflection of the many discriminatory legal and cultural practices that limit the provision of much needed health support for these populations. Some countries are also missing opportunities for improved surveillance data on the rates of STIs in such key populations. Lastly, the distribution of male condoms has remained stable throughout the rounds analysed, and the increasing inclusion of female condoms and lubricants has positive implications for women and MSM, enabling them to have the necessary reproductive health commodities.
This in-depth analysis of inclusion of STI components builds on the methodology and results of the previous systematic analysis of SRH elements in HIV proposals supported by the Global Fund, which clearly demonstrated that national level stakeholders see the opportunity for funding SRH services. Most STIs and HIV infection share mechanisms of transmission, risk behaviours and prevention measures that are not easy to separate, making it difficult to ascertain whether there is a critical balance of funding that maximises the impact on one or the other, or both. In addition, the proposals do not specifically include in every instance the financial information for each proposed activity. This makes it difficult to ascertain or track the actual funding that goes to activities that are specifically STI-related. Although it may also be informative to analyse unfunded HIV proposals, these are not available on the Global Fund website.
STIs are cofactors for HIV transmission and acquisition. The scientific evidence accumulated over the past two decades on the role of genital ulcer diseases and other STIs in facilitating the sexual transmission of HIV infection is beyond dispute. Even recent studies with more sophisticated tests have shown increased shedding of HIV in people (both men and women) coinfected with HIV and other STIs. Since people with STIs have a higher risk of acquiring or transmitting HIV infection through high-risk sexual behaviour and the cofactor effect of an existing STI, it is important to maintain services for STI control within the framework of HIV prevention.9 These services will provide opportunities for early treatment of STIs, counselling and communication for behaviour change; provide access to testing for HIV in populations with STIs and offer opportunities for prevention education and counselling for people with acute or established HIV infection; and serve as an entry point into care programmes for people living with HIV infection. Technical and advocacy guidance to countries wishing to include key components of STI prevention and control can be found in the WHO Global Strategy for the Prevention and Control of Sexually Transmitted Infections: 2006–201510 as well as technical guidance on SRH.11 The technical content of the Global STI Strategy deals with methods to promote healthy sexual behaviour, protective barrier methods, effective and accessible care for STIs, and upgrading of monitoring and evaluation of STI control programmes. Emphasis is placed on a public health approach based on sound scientific evidence and cost-effectiveness. A section on advocacy offers advice to programme managers on approaches to mobilising the high-level political commitment that forms the essential foundation for an accelerated response. The WHO technical guidance is designed to provide support for those who are writing HIV-related proposals to be submitted to the Global Fund. It focuses on specific SRH interventions that build on successes and endeavour to make programmes better through a holistic approach to HIV prevention and control. This approach provides opportunities to reduce unintended pregnancy and STIs, including HIV, as well as maternal and newborn morbidity and mortality. It also helps people to know their HIV status and helps to ensure that the SRH and rights of people living with HIV are respected.
For the key populations with high rates of treatable STIs, prevention and early treatment of STIs are essential to minimise the STI cofactor effect in the transmission of HIV, as well as to provide an entry point for a comprehensive prevention and care package for HIV and other STIs. Screening for asymptomatic infections or provision of treatment for STIs at periodic intervals for populations with poor access to healthcare, such as sex workers, are some of the strategies that countries need to consider more closely and seek funding for their implementation, particularly in settings with high STI and HIV burden.
The newer technologies that are becoming available, such as human papillomavirus vaccines and rapid diagnostic tests for STIs, and the possibility of accessing financial resources such as the Global Fund offer real opportunities for national strategic plans to include and scale up interventions for the prevention and control of STIs, including HIV infection. This analysis demonstrates that STI prevention and control is seen as a key cost-effective intervention by national stakeholders and that the Global Fund has been, and continues to be, supportive of such activities when included within HIV-related proposals. The types of interventions included cover a wide spectrum, reaffirming the importance of not promoting a single intervention for reducing the sexual transmission of HIV, but to establish and maintain a comprehensive package of services, which can be offered by referral or directly during an STI-related encounter.
Key messages
The Global Fund supports interventions related to STI prevention and care within the context of funding proposals for HIV, but numerous opportunities are missed.
Although countries are including targeted interventions, in particular for young people and most-at-risk populations with high rates of curable STIs, such as sex workers, opportunities for implementing proven interventions with maximum impact on infections and strengthened surveillance to inform programme success are missed.
Although there is good evidence to support targeted STI prevention and care interventions for men who have sex with men to prevent the spread of HIV infection, regional differences exist, probably reflecting the prevailing stigma and discriminatory regulations and policies towards these population groups.
The distribution of male condoms has remained consistently high throughout the rounds analysed at about 80%, but more needs to be done to make female condoms more accessible.
Footnotes
Competing interests None.
Provenance and peer review Commissioned; externally peer reviewed.