Article Text

Abstract
Background Active recall can improve reattendance rates and could increase retesting rates and detection of HIV and sexually transmitted infections (STIs), but the best strategy remains uncertain.
Methods We conducted a systematic review and meta-analysis of active recall for HIV and/or STI testing. We searched six electronic databases using terms for HIV, STIs, tests and active recall (defined as a reminder to retest for HIV/STIs) for randomised, non-randomised and observational English-language studies published between 1983 and 2013. Outcomes included reattendance/retesting rate and STI diagnosis at follow-up.
Results Of 5634 papers identified, 17 met the inclusion criteria. Of the 14 comparative studies, all but one demonstrated higher reattendance/retesting rates in the intervention group, but the range was wide (17.5–89%). Meta-analysis of nine RCTs found reattendance/retesting rates were significantly higher in the intervention versus control groups (pooled OR 2.42 (95% CI 1.84 to 3.19)). In a subgroup analysis, home sampling increased retesting compared with clinic testing (pooled OR 2.20 (95% CI 1.65 to 2.94)). In observational studies SMS reminders increased retesting compared with standard clinic care (pooled OR 2.19 (95% CI 1.46 to 3.29)), but study estimates were highly heterogeneous (I2=94%, p<0.001).
Conclusions Active recall interventions are associated with higher reattendance/retesting rates for HIV/STI. Although home sampling and SMS reminders were associated with higher reattendance/retesting rates in most studies, evidence is limited by the heterogeneity of interventions and control groups and the quality of studies. Further work is needed to explore which active recall modality is clinically cost-effective and acceptable for HIV/STI screening.
- HIV
- SEXUAL HEALTH
- HEALTH SERV RESEARCH
- TESTING
Statistics from Altmetric.com
Background
National guidelines in England recommend testing men who have sex with men (MSM) at high risk of sexually transmitted infections (STIs) every 3 months for HIV and STIs.1 Modelling studies suggest that 3-monthly testing is cost saving and could reduce the number of new HIV infections.2 ,3 Despite this, cross-sectional survey data suggests that less than a quarter of MSM in England and Scotland have four or more HIV tests per year.4
Reminders in healthcare improve attendance and reattendance rates.5 ,6 Reminders for STI or HIV testing include text messages, emails, telephone calls or letters. Sending out a kit for home sample collection or testing is another option. National guidance recommends use of reminders for encouraging retesting of MSM, but only a quarter of sexual health clinics have a recall system in place.7 Healthcare providers need to know which is the most effective approach to increase reattendance/retesting rates before widespread implementation.
Several studies have examined the effectiveness of active recall for healthcare appointments in general.8 A review of interventions to increase rates of rescreening for chlamydia found evidence for mailing rescreening kits, to increase retesting rates and for telephone reminders, but evidence for text messages has been conflicting.9 ,10
The reason for the conflicting evidence may be related to barriers to reminders that may reduce their acceptability and effectiveness in increasing reattendance or retesting and need to be explored. Concerns regarding privacy, confidentiality and data protection have led to some services providing opt-in schemes.11
Text message reminders have the potential to be a useful active recall intervention if efficacy can be demonstrated. It is an inexpensive, unobtrusive and simple way of reminding patients about healthcare appointments,12 but it is a relatively new technology within the healthcare field. In high-income countries, 70–90% of people have a mobile phone subscription, similar among all socioeconomic groups.11
Mailing rescreening kits, or home sampling in which a patient takes his/her own sample, also has the potential to access individuals for whom accessing a service is a barrier. Home sampling can increase uptake,13 but not necessarily frequency of testing13 ,14 and surveys of attitudes to self-sampling have highlighted barriers to self-sampling including timeliness of results, accuracy and lack of immediate professional support.15 ,16
We conducted a systematic literature review to compare the impact of active recall interventions in increasing screening and rescreening rates as well as the detection of HIV and STIs in patients who are HIV-negative or of unknown status.
Methods
Eligibility criteria
Active recall was defined as a reminder to return for or to have a repeat test or screen. This could take the form of a text message, email, telephone call, letter, or sending out a kit for home sample collection or testing. A verbal reminder at the initial visit did not count as active recall.
We used the PICO (population, intervention, comparison, outcome) framework17 to guide our eligibility criteria. Studies of patients who were HIV-negative or of unknown status were eligible for inclusion. Studies from all countries were included and testing facilities included hospitals, sexual health clinics, general practice, community venues and home sampling/testing.
The intervention was active recall (as defined above) and the comparator was no active recall, a reminder at the initial visit only or no comparator (in the case of non-comparative and cohort studies). The primary outcome of interest was the proportion of those recalled who reattended or retested at least once. The secondary outcomes were additional infections among those retested (number of infections/number reattended or retested) and infections detected among those recalled (number of infections/number recalled). This gives an idea of clinical and public health benefits, since clinical benefit may be high if the number of additional infections at retest is high, but public health benefit will depend on the number of additional infections identified through active recall, in relation to the cost of the programme.
All randomised and non-randomised interventional and non-interventional study designs were included. Qualitative studies were excluded from this review.
Exclusion criteria included studies without a recall intervention, pretest and post-test counselling without a recall intervention, recall for current episodes of care including tests of cure, postexposure and pre-exposure prophylaxis studies, review articles, conference abstracts and news reviews.
Search strategy
We searched six databases: Medline, Pubmed, Embase, Cinahl Plus, Psychinfo and the Cochrane Database of Systematic Reviews limiting the search from 1983 up to the date of the final search on 6 December 2013, human studies and English language studies. Search keywords included HIV, terms for STIs, specific STIs including chlamydia and gonorrhoea, test, screen, terms for active recall, and the specific modes of active recall including text message and telephone. The full search strategy is provided in the online supplementary annex.
One reviewer (MD) searched the databases and performed a full title screen to remove obviously irrelevant articles. Shortlisted titles underwent full abstract review and full papers were shortlisted using the eligibility criteria above. Full paper review was conducted by one reviewer (MD) to generate a final list of papers included in the review. One reviewer (MD) manually searched the reference list of included papers to identify any articles missed by the search strategy. Two reviewers (MD and SW) extracted data from the selected papers.
Quality assessment
The National Institute of Health and Care Excellence Public Health Methods Manual was used to assess the methodological quality of each study.18 This is a modification of the graphical appraisal tool for epidemiological studies checklist for interventional and observational studies. This tool was chosen as it is intended for use in the development of public health guidance and allows for assessment of all study types. Where the reviewers (MD and SW) felt any items on the tool were ambiguous, these reviewers agreed and applied study-specific criteria.
Statistical analysis
Outcome data for reattendance/retesting was pooled using a random effects model due to heterogeneity between studies and study samples using the Stata statistical package.19 ,20 Pooled ORs are presented separately for randomised controlled trials (RCTs) and observational studies, since biases inherent to observational studies may affect the RCT results. Pooled OR for each active recall intervention is presented separately and as an overall pooled estimate. Each of the studies followed up participants over different time periods; crude and pooled ORs are presented, but the heterogeneity of studies is also considered. We controlled for heterogeneity of study population as far as possible by presenting results for studies with two distinct comparison groups, such as a concurrent and historical control group or control groups from two independent populations separately.
Publication bias was assessed with a funnel plot and using the Harbord test of small study sizes.21
Factors associated with reattendance/retesting are presented descriptively, with population subgroup analyses where possible (eg, by gender, sexual orientation).
Results
Search results
The electronic search identified 5634 unique citations. Title and abstract screening identified 45 citations as potentially eligible for the review and full text was retrieved for these studies. Twenty-eight studies were excluded for reasons outlined in the online supplementary annex. Seventeen studies met the eligibility criteria (online supplementary annex figure 1).
Study design and intervention (see tables 1 and 2): Six were RCTs (four home sampling, one phone call reminder and one SMS reminder). Two of the home sampling studies used a phone call reminder and one used an email reminder in addition to sending the kit. Eleven studies were observational with an intervention, including non-randomised before and after controlled studies (n=5), non-comparative studies (n=4) and cohort studies (n=2). Non-comparative studies included cross-sectional studies and service evaluations. Four used an SMS reminder, one used a postcard/letter, one used a phone call and five used a home sampling kit. One of the home sampling kit studies used a telephone reminder in addition to sending the kit.
Study characteristics for randomised control trials
Study characteristics for observational studies
Comparator: All comparator arms for the home sampling randomised control studies used either a phone call, email or postcard reminder in addition to the offer of a test at a clinic.
Populations: Three studies were conducted among MSM only, two included MSM among other male and female populations, five included women only and the remainder included men and women.
Geography: Two studies were conducted in the Netherlands,24 ,33 four in the UK,29 ,31 ,34 ,36 five in Australia9 ,10 ,27 ,28 ,35 and the remainder in the USA.22 ,23 ,25 ,26 ,30 ,32
Risk of bias
Online supplementary annex tables 1 and 2 show the methodological quality of included interventional studies. Of the six RCTs, one was assessed as having all of the criteria of internal validity fulfilled (++: high quality study)25 and the remainder fulfilled some of the criteria (+: moderate quality study). The moderate quality RCTs were not adequately blinded, were underpowered or did not account for all sources of potential bias, for example, baseline characteristics, sexual risk. Only one RCT was assessed as having adequate (+) external validity.10
Of the controlled before and after studies, all were felt to have only adequate (+: moderate quality study) internal validity due to not being randomised (and hence unable to minimise allocation or selection bias); some did not adjust for potential confounders at analysis. All were assessed as having low external validity (−).
Of the included observational studies, one was felt to have high (++: high quality study) internal validity and the remainder adequate (+: moderate quality study) internal validity. Reasons included potential selection bias due to ghost addresses and systematic differences in baseline characteristics between included and excluded groups. All were assessed as having low external validity (−), mainly because the source population was not clearly identified and hence findings could not be generalised.
Reattendance rates
Overall
Overall, use of active recall increased reattendance/retesting and all but one study of active recall with high or moderate internal validity (high/moderate quality study) demonstrated high reattendance/retesting rates in the intervention group; however range of reattendance was wide between 17%32 and 89%.28 Among all active recall interventions, the OR for reattendance in the intervention group compared with the control group ranged from 0.93 (95% CI 0.65 to 1.33) to 14.0 (95% CI 1.63 to 120.1).
The pooled OR for reattendance/retesting in the six RCTs was 2.42 (95% CI 1.84 to 3.19) and had low heterogeneity (I2=38%, p=0.12) among 2400 participants (table 3, figure 1).
Summary table of reattendance/retest outcomes for randomised control trials

Forest plot of odds ratio of reattendance in randomised controlled trials of active recall for STI/HIV screening.
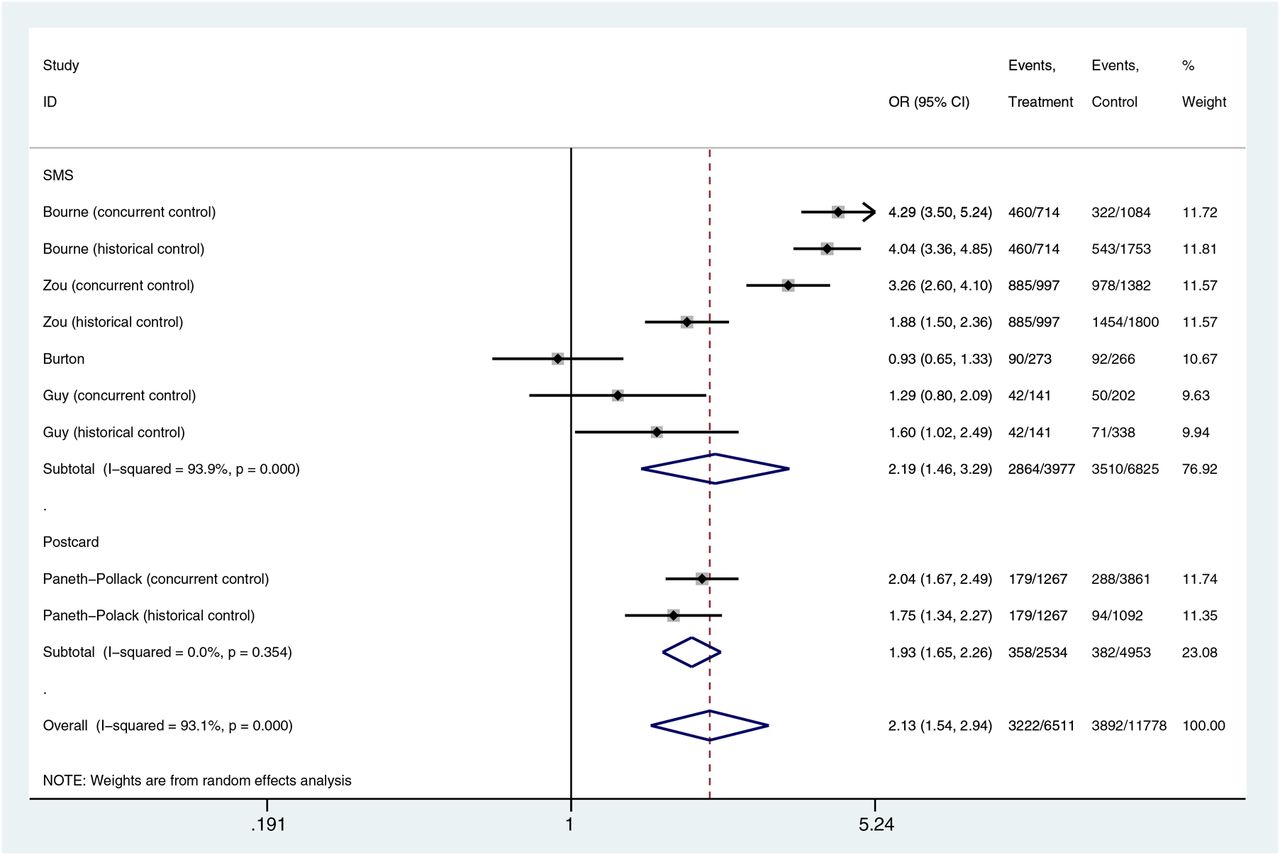
The pooled OR for reattendance/retesting in the observational studies was 2.13 (95% CI 1.54 to 2.93) but had high heterogeneity (I2=93%, p<0.001) among 18 289 participants (table 4, Ofigure 2).
Summary table of reattendance/retest outcomes for observational studies
{kind=link}
{kind=link}
Forest plot of odds ratio of reattendance in observational studies of active recall for STI/HIV screening.
SMS
Five studies used SMS as the active recall intervention.9 ,10 ,27–29 Among SMS reminder intervention groups, the OR of reattendance/retesting compared with clinic control groups ranged between 0.93 (95% CI 0.65 to 1.33)29 and 5.87 (95% CI 1.16 to 29.83).10 The pooled OR among the observational studies was 2.19 (95% CI 1.47 to 3.23) but had high heterogeneity (I2=93%, p<0.001). A pooled OR for reattendance among the SMS group was derived from two RCT substudies of different interventions (SMS only and SMS+financial incentive) reported in one paper and was 5.66 (95% CI 1.78 to 17.99) among 126 participants and had low heterogeneity (I2=0.0%, p=0.95).10 However, although this study was of high methodological quality, populations were recruited from the same clinic population and sample sizes were very small.10
Phone call reminders
One study used phone calls as an active recall intervention.26 Two groups received a phone call reminder in addition to verbal advice and counselling. Both groups saw higher reattendance compared with controls who received verbal advice only. The OR for the phone call reminder+verbal advice+counselling group was 2.50 (95% CI 1.3 to 4.8) and the OR for the phone call reminder+verbal advice group was 14.0 (95% CI 1.63 to 120.09) (table 2, figure 2). However this study had poor internal and external validity, was not powered to show an effect, the control arm included an intervention that was not standard care, and there was little information about the representativeness of the study population in relation to the source.
Home sampling kit
Four RCTs22–25 and five observational studies32–36 assessed the impact of sending home sampling kits on retesting rates. The four RCTs sent out a home sampling kit combined with a phone call/email reminder and had a comparison group, which included clinic appointment+phone call/email/postcard reminder. The observational studies did not have comparator arms.
Among the four RCTs, retest rates in the home sampling groups ranged from 1.54 (95% CI 1.11 to 2.15)23 to 2.83 (95% CI 1.78 to 4.50).25 The pooled OR was 2.20 (95% CI 1.65 to 2.94) across 1942 participants and had low heterogeneity (I2=44%, p=0.13).
Clinical outcome
Four RCTs reported chlamydia infection rates10 ,23 ,24 ,37 at retest as the clinical outcome, one reported chlamydia and gonorrhoea infection at retest22 and one looked at STIs in general25 (online supplementary annex table 3). Three observational studies reported acute bacterial STIs (chlamydia, gonorrhoea, syphilis and Lymphogranuloma Venereum (LGV)) and HIV (SMS reminders as the active recall),28 ,29 ,31 five reported chlamydia reinfection (all home sampling studies),32–36 one reported chlamydia and gonorrhoea reinfection (postcard/letter as the active recall)30 and two did not report a clinical outcome9 ,27 (online supplementary annex table 4).
Two RCTs reported clinical outcomes that allowed OR of infections in the intervention group compared with the control group to be calculated.23 ,24 Both compared home sampling kit intervention with email/phone reminder to clinic care. The OR of testing positive at the retest visit in intervention versus control groups ranged between 0.7 (95% CI 0.3 to 1.5) and 0.9 (95% CI 0.3 to 2.6) among those retested, and between 0.9 (95% CI 0.4 to 1.8) and 1.6 (95% CI 0.4 to 6.5) among those recalled.
Factors associated with reattendance/retest
In this review, in studies that included men and women, women were more likely to retest than men.24 ,30 Those men and women who were younger, had more sexual partners or had a lower education level were less likely to retest.24 ,33 Among studies that only included MSM, reattenders were more likely to have higher number of partners but also have higher condom use.28
Assessment of publication bias
A funnel plot of RCTs shows symmetry for the home sampling studies which all appear to be larger studies (online supplementary figure 2 annex). The Harbord test for small study size effect suggests that there is no small study size effect (p=0.520). The SMS interventions and phone call studies are too few to comment upon.
A funnel plot of observational studies suggests some asymmetry with lack of small studies showing a large effect size for SMS interventions (online supplementary figure 3 annex). The Harbord test for small study size suggests no small study size effect (p=0.063). There are too few postcard studies and no home sampling studies to comment on these intervention types.
Discussion
The studies in this review provide evidence for the use of active recall in increasing or achieving high reattendance/retesting rates for testing for HIV/STIs. Although the review suggests that home sampling and SMS are associated with higher rates of reattendance/retesting, evidence is limited by heterogeneity of interventions and control groups and the quality of studies. There were too few studies to assess the impact of other interventions. The results do not provide clear evidence to support any one active recall intervention over another.
It was not possible to determine the impact of active recall on detection of STI reinfection as only two RCTs compared infection rates between the intervention and control groups. Although both studies suggest no difference in infection rates between the control and intervention groups, they have a wide non-significant CI.
Our findings are in agreement with other systematic reviews of active recall to improve reattendance rates for healthcare appointments, vaccinations, other diseases such as tuberculosis and health promotion,5 ,6 ,8 ,38 which have demonstrated net benefit. Several reasons have been given for missed appointments, including forgetting, and the use of a reminder can help facilitate reattendance.39 ,40
A review by Car et al found that SMS reminders increased the rate of attendance at healthcare appointments compared with no reminders (risk ratio 1.10 (95% CI 1.03 to 1.17). Cost per attendance for SMS reminders was lower than phone reminders.8 SMS has been successfully used in health promotion, and a recent meta-analysis suggested a net benefit of SMS on health outcomes.38
Reattendance among MSM in this review was associated with higher number of partners and higher condom use, which may reflect higher self-perceived risk and greater awareness of sexual health.28 This demonstrates features of regular and repeat testers. Regular testers test on a regular basis, for example, once a month, sometimes as part of a routine health check, and this may not be indicative of sexual risk.41–43 They are less likely to have been diagnosed with an STI, perceive lower sexual risk and report protected insertive anal sex.44 Repeat testers undergo additional HIV tests after receiving an initial negative result. Repeat testing among MSM has been associated with a history of STIs, higher number of sexual partners, having oral or unprotected insertive anal sex, and knowing someone with HIV infection.42 ,44 In this review, non-reattenders in response to recall were more likely to be HIV-positive,31 in keeping with studies that have compared sexual risk among those that test for HIV compared with those that do not.31 ,45 ,46
The theory of planned behaviour47 suggests that social norms, behavioural attitudes and perceived behavioural control influence an individual's behavioural intention to test. In the case of HIV/STI screening, active recall may influence behavioural attitudes and perceived behavioural control to empower an individual to take control of their sexual health and change their testing behaviour, changing their probability of reattendance. Few studies explore the drivers and barriers to active recall for HIV/STI recall, and those that do highlight concerns regarding the confidentiality and sensitivity of active recall reminders and the importance of framing the message correctly. Qualitative studies highlight the importance of using messages to increase risk perception and motivational messages to reduce fear of getting tested.48
If active recall for HIV/STI testing is an effective method to increase reattendance rates, as is suggested by this review, the most cost-effective strategy needs to be determined. One study assessed cost-effectiveness of phone call reminders and found brief verbal advice combined with a phone reminder yielded the highest return rate and the lowest cost per infection treated compared with brief verbal advice alone or a financial incentive.49 Other studies suggest that the use of SMS reminders is a cheap and effective way of increasing reattendance rates for HIV/STI testing, but no cost-effectiveness studies were performed.
Limitations
The inclusion criteria were kept broad to include as many relevant studies as possible. However this resulted in variation in the OR for reattendance attributable to heterogeneity for some intervention types. This may be due to differences in study populations and different follow-up times.
Second, the low methodological quality of the majority of the included studies means that it is difficult to draw conclusions about any of the individual active recall intervention types. Participants in studies of active recall reminders are not blinded to the intervention they receive; this results in these studies receiving a low score for internal validity due to the potential for selection and participation bias. Several studies included multiple interventions or did not have a standard care comparison, making it difficult to unpick individual intervention effects.
None of the studies scored highly for external validity because it was not possible to assess representativeness of the source population to the general population.
Conclusions
This systematic review suggests that active recall interventions are associated with an increase in retesting rates for HIV/STIs. However, the evidence is limited by heterogeneity of interventions and control groups and therefore cannot determine which method of active recall is most effective.
An adequately powered RCT comparing the different methods of active recall is needed to assess the efficacy of the different active recall interventions, their cost-effectiveness and acceptability as well as drivers and barriers to returning for a HIV/STI screen when actively recalled.
Key messages
Use of reminders or active recall can increase or achieve high reattendance rates for HIV/sexually transmitted infection (STI) screening and rescreening.
There is insufficient evidence to guide which mode of active recall is the most effective.
Further studies are needed to determine the cost-effectiveness and acceptability of active recall interventions for HIV/STI screening.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Handling editor Jackie A Cassell
Contributors MD devised and planned the review, conducted the literature search, data extraction, quality assessment and wrote the initial draft of the manuscript. SW was involved in planning the review and contributed equally to data extraction, quality assessment and manuscript preparation. AN, DM, FB and RG were involved in planning the review and contributed equally to manuscript preparation and review. All authors had full access to all the data in the study and can take responsibility for the integrity of the data and accuracy of the data analysis. SW worked with Professor Charles Lacey and Becky Wiggins on a review of repeat infection with chlamydia after treatment which informed some of the review strategy for this paper.
Competing interests MD reports personal fees from Janssen, outside the submitted work. FB reports grants from Gilead, personal fees from Janssen, personal fees from MSD, grants from NIHR, outside the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement MD and SW have access to study data and results. Further access to unpublished data is available upon request.