Article Text

Abstract
Objective To determine how the risk of HIV transmission from homosexual men receiving antiretroviral treatment is related to patterns of patient monitoring and condom use.
Methods A stochastic mathematical simulation model was developed of cohorts of men in the Netherlands who have sex with men (MSM), defining the parameters of the model using observational cohort data. The model incorporates viral load trends during first-line treatment, patient monitoring and different scenarios for the way in which condom use may depend on recent viral load measurements. The model does not include the effect of sexually transmitted infections on HIV transmission.
Results For MSM receiving treatment, the risk of transmitting HIV to their long-term partner is 22% (uncertainty interval: 9–37%) if condoms are never used. With incomplete use (in 30% of sex acts) the risk is reduced slightly, to 17% (7–29%). However, the risk is as low as 3% (0.2–8%) when men receiving treatment use condoms only 6 months beyond their last undetectable viral load measurement. The risk is further reduced when 3 months is the time period beyond which condoms are used.
Conclusions When condom use by HIV-infected men receiving combination treatment with antiretroviral agents is based on their last viral load measurement, the transmission risk is much lower than with incomplete condom use. The key message for patients is that although always using condoms during treatment is the best way to protect partners from the risk of HIV transmission, when such use cannot be achieved, the second best strategy is to use condoms whenever the last undetectable viral load was measured more than 3 months ago.
- Condoms
- HIV
- mathematical model
- transmission
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Introduction
Since the mid-1990s, people infected with HIV in industrialised countries have been able to access combination antiretroviral treatment (cART),1 2 which has substantially decreased HIV-associated mortality in these populations.3 More recently, this trend has been repeated in many developing countries, along with signs of decreasing HIV mortality.4 In both settings, there is a trend for earlier initiation of treatment5 and increasing debate about whether starting treatment earlier (or even immediately on HIV diagnosis) is advisable in order to improve clinical outcomes and reduce HIV transmission.6 7 As the population receiving treatment grows its potential contribution to HIV epidemic increases. Therefore, we expect that the infectiousness and the sexual behaviour of those receiving treatment will become key determinants of the trajectory of the global epidemic in the coming years.
The rate of HIV transmission from infected people is closely tied to their plasma viral load, which cART can reduce to very low levels.8 On this evidence, in 2008 the Swiss National AIDS Commission (EKAF) suggested that there was effectively no risk of sexual transmission from patients receiving cART, provided that they (i) follow the guidelines for antiretroviral treatment strictly, (ii) have no detectable viral load when measured in the past 6 months and (iii) have no other sexually transmitted infection (STI).9 10 The implication that such patients need not use condoms with their sexual partners was warmly welcomed by patient groups and activists.11
In response, many argued that this was not a helpful public health message. Although the chance of transmission from men receiving treatment is likely to be low, it is unlikely to be zero, since at least one transmission event from a man receiving successful cART has occurred,12 and over many sex acts among many men, a small rate of transmission could translate into a large number of new infections.13 14 A simple model was used to argue this point,13 but it did not estimate the absolute risk of transmission from men receiving treatment; nor did it account for condom use being conditional on a recent viral load measurement, as the EKAF statement recommended.9
In this paper, using uniquely detailed data on the trends in viral loads among men receiving treatment17 and a new stochastic mathematical model, we estimate the risk of HIV transmission from men in the Netherlands who have sex with men (MSM) and determine how this is influenced by various patterns of condom use (including those based on the Swiss recommendations) and schedules of viral load monitoring.
Methods
Following earlier work,18 19 we developed a stochastic individual-based simulation model of viral load trends, HIV transmission risk and patient monitoring among cohorts of MSM in the Netherlands. The vast range of possibilities for the evolution of viral load over time was conceptualised as three distinct trajectories (figure 1). Data from the ATHENA observational cohort of HIV-infected individuals in the Netherlands17 were used to evaluate the parameters (table 1, with further detail provided in the online technical appendix).
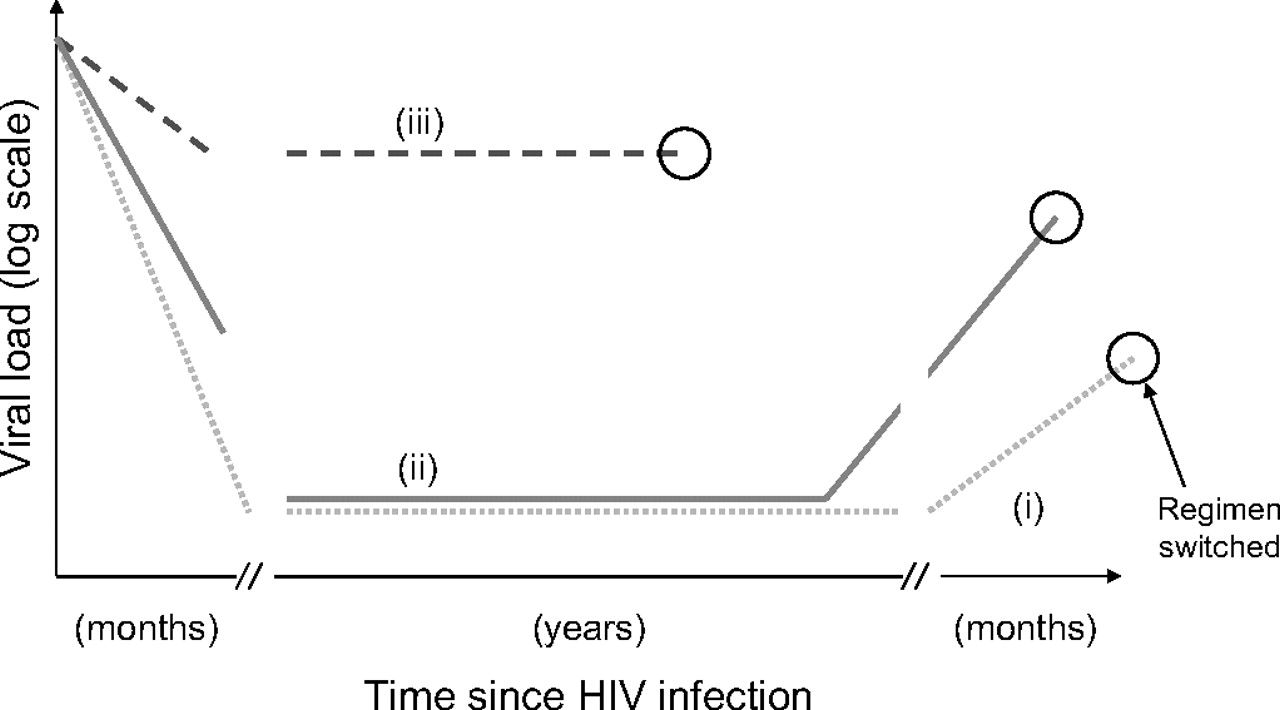
Schematic representation of the three assumed trajectories of (log) viral load after treatment initiation: (i) suppression achieved and adherence good (dotted line); (ii) suppression achieved but adherence poor (solid line); and (iii) suppression not achieved (dashed line). The circles indicate when the regimen was changed. Parameter values are presented in table 1 and details are provided in the online supplementary appendix.
Natural history parameters for HIV infection receiving first-line treatment (Source: ATHENA cohort data17) Refer to the technical appendix for details
The risk of transmission is characterised as the probability that a man receiving treatment will infect his uninfected sexual partner over the course of first-line treatment. We examined only the special case where a partnership is maintained over the entire duration of first-line treatment and did not include the effect of STIs on the chance of HIV transmission. In most analyses, the functional relationship between plasma viral load and the chance of transmission in each unprotected sex act was based on a Hill function fitted to observational data on HIV transmission in Zambia by Fraser et al.20 This function is supported by recent review of transmission rates15 16 and is denoted the ‘Fraser et al’ assumption. The function was rescaled to match the observed approximate transmission risk for each sex act for MSM (∼0.01 for men with log-viral loads of ∼4.5 log-copies)13 (supplementary figure S2). An alternative assumption for the relationship (linear trend in log-risk and log-viral load21: see figure S2) was used as well in sensitivity analyses: this is denoted the ‘Wilson et al’ assumption. We assumed that there were 100 sex acts a year in the partnership and that the efficacy of condoms in reducing transmission is 95%. In uncertainty analyses, the model assumption for which there was least directly relevant data was varied independently in a Monte Carlo analysis: specifically, the frequency of sex acts per years (uniform between 50 and 150), the efficacy of condoms when used (uniform between 85% and 100%) and chance of transmission per sex act without treatment (uniform from 0.0075 to 0.0125). A combined 95% uncertainty interval (the range between the 2.5th and 97.5th centiles of the resultant distribution) was calculated.
In the model, reflecting clinical guidelines,22 patients with undetectable viral loads are monitored every 4 months. When viral load is detectable, the patient returns for another appointment after 8 weeks and the treatment regimen is then changed if retesting confirms the finding.
Various scenarios for condom use in partnerships were considered: (i) never using condoms; (ii) using condoms in 30% of sex acts24; (iii) not using condoms if viral load was undetectable at the last measurement in the past 6 months; and, (iv) always using condoms. Scenario (iii) corresponds to the way that the EKAF statement has been interpreted and we considered two variants whereby the decision not to use condoms is based on the last measurement in the past 3 months (instead of 6 months) or the last viral load measurement ever taken (ie, irrespective of time).
Results
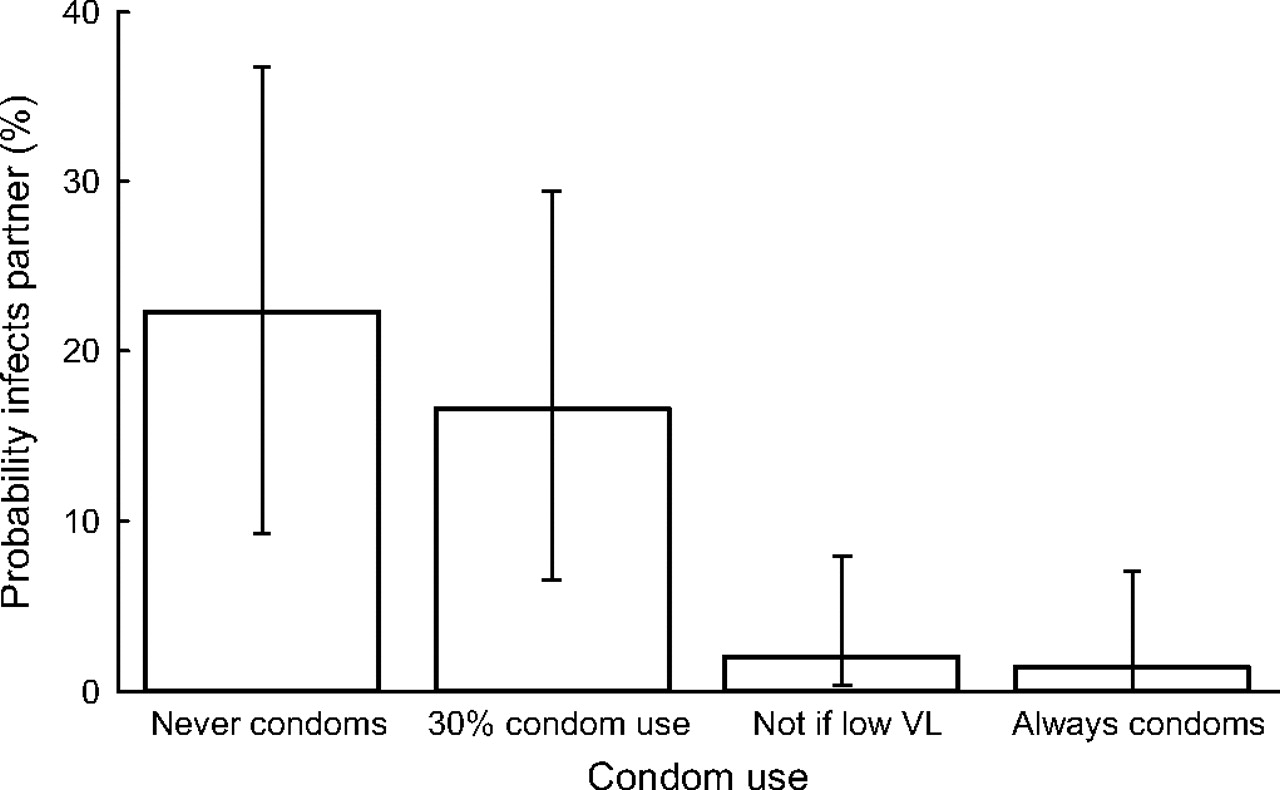
We found that men receiving treatment pose a substantial risk of HIV transmission (22% (9–37% in uncertainty analysis)) to their partners if they do not use condoms (figure 2), and the relationship between viral load and transmission is as described by Fraser et al.20 This risk is generated in three ways: (i) treatment is not sufficient to suppress viral load, so transmission can occur even if the regimen is quickly changed; (ii) the level of virus can rebound quickly and reach high levels before detection and change of regimen; (iii) even with suppressed viral loads, the risk of transmission is not zero, so that over the many sex acts during treatment, the cumulative chance of transmission becomes non-negligible.

Probability of transmission to partner during first-line treatment, if condoms are never used; condoms are used 30% of the time; (iii) condoms are used unless last viral load (VL) measurement in the past 6 months was undetectable; or always using condoms. Error-bars show the 95% uncertainty interval, as described in the text. It is assumed that the partnership is maintained over the entire course of first-line treatment and that viral load is related to transmission rate, as Fraser et al20 have described.
Using condoms 30% of the time reduces the chance of transmission but only marginally (to 17% (7–29% in uncertainty analysis)), since there remains a substantial numbers of unprotected sex acts overall. In contrast, men who always use condoms unless their viral load was undetectable at the last measurement in the past 6 months are much less likely to transmit HIV to their partner (chance of transmission: 3% (0.2–8% in uncertainty analyses)). This is because the risk generated in the first two ways has been largely removed. Men following this strategy, on average, use condoms 10% of the time they are receiving treatment, while reducing the risk of transmission to 3%. The risk with this strategy is nevertheless greater than always using condoms, in which the chance is 1% (0–7% in uncertainty analysis) (figure 2). The risk is not zero, because condom efficacy is not perfect.
Using the alternative (‘Wilson et al’) assumption about the relationship between plasma viral load and transmissibility, the overall chance of infection if condoms are not used is higher (47% vs 22%), but the same key result is reproduced: men who use condoms unless their viral load was undetectable in the past 6 months are much less likely to transmit HIV to their partner than if condoms are used intermittently (online figure S3).
The frequency with which patients receiving treatment are monitored is a key determinant of the chance of HIV transmission (figure 3A). Patients monitored frequently can be quickly switched to new regimens if first-line treatment fails—that is, before viral load increases and they have exposed their partner to an increased risk of transmission for a long period. The second effect of increased frequency of monitoring is the reduction in overall condom use. This is because with less frequent monitoring, many men with suppressed viral loads would use condoms since they have not had a recent viral load measurement. With monitoring every 18 months, condoms would be used in ∼70% of sex acts, but with monitoring every 3 months, condoms are used in only 9%.

{kind=link}
{kind=link}
{kind=link}
The influence of (A) monitoring frequency and (B) loss to follow-up on the probability of HIV transmission, assuming condoms are used unless last viral load measurement in the past 6 months was undetectable. It is assumed that the partnership is maintained over the entire course of first-line treatment and that viral load is related to transmission rate, as Fraser et al20 have described.
The benefit of patient monitoring is influenced by the proportion of patients lost to follow-up. The probability of infecting a partner increases from 2% when none of the patients are lost to follow-up, to 5% when 20% do not return for care (figure 3B). This is because increases in viral load go undetected for longer, exposing partners to a higher risk of infection.
Finally, we examined three ways in which condom use could be based on viral load measurements (online figure S5). The decision not to use condoms could be based on an undetectable viral load in the past 3 months, the past 6 months or the last measurement ever. With the decision based on a measurement in the past 3 months, there is reduced transmission compared with a decision based on the past 6 months, provided that patients are monitored at least every 3–12 months. However, with the decision based only on the last measurement regardless of time, the chance of transmission is higher, especially if monitoring intervals are longer.
Discussion
The debate about the EKAF statement on HIV transmission from patients receiving cART13 and earlier modelling work14 did not consider the way in which deciding not to use condoms might be conditional on the last viral load measurement. There was also little focus on estimating the rate of HIV transmission across the population or exploring how it is influenced by patterns of patient monitoring. In this paper we have shown that basing the decision to use condoms on viral load provides substantially better protection to partners than incomplete condom use, provided that the measurement is within the past 3–6 months. Compared with always using condoms, the viral-load-dependent strategy allows slightly more HIV transmission (2–3% vs 1%). However, as condoms are needed much less of the time (10% vs 100%), adherence to this strategy may be better.
Our results also highlight the importance of monitoring patients more often and minimising losses to follow-up. Without such effort, increases in viral load go undetected, exposing partners to higher risks of transmission.23 With measurement at intervals of 3–12 months, the risk of transmission can be reduced further by basing condom use on measurements taken only 3 months before. This guards against the risk of increases in viral load since the last measurement.25 For this reasons, it is important that decisions are not based on viral load measurements taken more than 6 months before.
The model used in this paper incorporates more biological realism than earlier work13 14 by using the functional form of the viral load–transmission relationship that reflects a sophisticated analysis of observational data,20 explicitly tracking viral load monitoring and modelling the course of viral load evolution over time. Nevertheless, a number of simplifying assumptions were made. The risk of transmission per sex act was scaled to match only an approximate observation of the risk, without considering differences in the frequency of being the insertive or receptive partner.26 27 We assumed that, below a certain viral load level, the chance of transmission is low and not actually zero; but evidence is lacking, since observing almost no instances of transmission15 could be consistent with either possibility. The response of patients to treatment varies widely and we have attempted to only broadly represent this in the model. However, we believe the key features of viral load evolution have been captured by finding a set of parameters for the viral load trajectory (its rise, period of stability and subsequent rise) and its relationship to treatment adherence. An important limitation of the model is that the effects of other STIs on HIV transmission is not incorporated. The data available from the cohort do not permit a detailed representation of STI transmission and the influence of STIs would depend on many factors, including the pattern of STI spread across the populations. If STIs were included, the overall estimate of HIV transmission risk would probably be greater, but we would expect the key relationship between risk and patterns of condom use to hold or be strengthened (since more frequent screening affords greater opportunity for treating STIs). Finally, the model does not include the influence of intermittent viraemia on the chance of HIV transmission, since we assumed its influence on transmission to be relatively small.28
The implications of this work are that the key message to patients should remain that always using condoms when receiving treatment is the best way to protect partners from the risk of HIV transmission. However, an additional message is that using condoms is most crucial when patients have not recently (within the past 3 months) had an undetectable viral load measurement. This message refines the intuitive association between successful treatment and reduced transmission24 29 and could substantially improve protection for infected partners. This advice must be supported by frequent viral load monitoring (at least every 6 months, but preferably every 3 months) of all patients receiving treatment.
Key messages
Intermittent use of condoms by men receiving treatment offers relatively little reduction in the chance of transmission to their partner.
In contrast, the chance of HIV transmission can be substantially reduced if condoms are used when the last undetectable viral load measurement was not within the past 3 months.
Frequent viral load measurement can maximise the potential for treatment to reduce HIV transmission.
Acknowledgments
TBH thanks the Wellcome Trust for funding support. We thank two reviewers for their constructive assessment of this work.
References
Supplementary materials
Web Only Data sti.2010.042622
Files in this Data Supplement:
Footnotes
TBH and CS contributed equally to this paper.
Funding Wellcome Trust.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.