Article Text

Abstract
Introduction The Chinese government has invested US$140 million annually on prevention of mother-to-child transmission (PMTCT) of HIV. This study evaluates the programme by examining the improvements in programme coverage HIV testing and provision of antiviral drugs along the PMTCT cascade.
Methods Data for PMTCT cascade indicators were collected through a comprehensive systematic review of published peer-reviewed English and Chinese literature during 2003–2011. Meta-analysis was conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Results This study included 113 publications. HIV prevalence among pregnant women in China who accessed antenatal care (ANC) remained below 0.1% during the past decade. HIV testing coverage in pregnant women attending ANC and in HIV-exposed infants at 18 months significantly increased from 62.4% (95% CI 4.7% to 98.2%) and 22.1% (16.3% to 32.3%) in 2003 to 90.3% (88.4% to 91.8%) and 82.8% (66.9% to 99.5%) in 2011 respectively, whereas antiretroviral (ARV) prophylaxis uptake increased from 35.2% (12.2% to 47.3%) and 26.9% (24.3% to 28.9%) to 86.2% (53.2% to 97.2%) and 90.3% (85.5% to 93.7%). HIV vertical transmission rate substantially decreased from 31.8% (25.7% to 38.6%) prior to the programme to 2.3% (1.4% to 3.8%) in 2011. During 2003–2011, among 25 312 (23 995–26 644) infants born to HIV-positive mothers who received ARV prophylaxis, 975 (564–1395) were diagnosed with HIV, corresponding to an average transmission rate of 3.9% (3.2% to 4.6%). However, while including transmissions among HIV-positive pregnant women who were lost along the cascade, the average transmission rate during 2003–2011 was 17.4% (15.8% to 19.0%).
Conclusions PMTCT programmes have reduced HIV mother-to-child transmission in China. Further improvements in the continuum of care remain essential in realising the full potential of the programme.
- HIV
- WOMEN
- ANTIRETROVIRAL THERAPY
- AIDS
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Effective prevention of mother-to-child transmission (PMTCT) of HIV can reduce the vertical transmission risk from 15%–45% to below 5% in breastfeeding populations and below 2% in non-breastfeeding populations.1–3 The 2013 WHO guidelines recommend that all HIV-positive pregnant and breastfeeding women start antiretroviral therapy (ART) as early as during 14 weeks of pregnancy and continue lifelong treatment if resources are available particularly in generalised epidemics. In some countries, for women who are not eligible for ART according to national guidelines, stopping ART after cessation of mother-to-child transmission (MTCT) risk could be considered.4 These guidelines support the implementation of the Global Plan and Asia Pacific Frameworks towards the elimination of new HIV infections that may occur among children.3 ,5 ,6
According to the official statistics, at the end of 2011, 780 000 people were living with HIV in China of which female patients accounted for 28.6%.7 About 10–13 million Chinese women gave birth annually during 2003–2011,8 and HIV infection among pregnant women is below 0.1%.9 Although infections attributed to MTCT accounted for less than 2% of the reported HIV cases in China in 2011,7 ,10 recent studies indicated that the proportion of women infected with HIV has doubled over the past decade and heterosexual exposure remains the main route of transmission.11 ,12 This suggests a continued risk of MTCT of HIV.13 In 2003, China initiated its first PMTCT programme in eight cities which provided free HIV testing and antiretroviral (ARV) prophylaxis as part of standard antenatal care. Prior to 2011, azidothymidine (AZT) and nevirapine (NVP) were the recommended ARVs for HIV-positive pregnant women and newborns.14 ,15 Lamivudine was added later as a third drug.16 HIV testing was provided routinely and confirmed positive diagnoses were reported to the China Information System for Disease Control and Prevention through the antenatal care network. ARV prophylaxis was administered to HIV-positive pregnant women during pregnancy, delivery and postpartum as well as to their babies after delivery. All HIV-infected mothers received free infant formula. In 2010, the national PMTCT programme expanded to integrated PMTCT, which included universal syphilis and hepatitis B testing and treatment. The hypothesis was that integrated testing for several infections would increase the HIV testing uptake. This approach was feasible and successful.17 ,18 Government investment for integrated PMTCT has dramatically increased from US$0.9 million in 2003 to US$136.8 million in 2010.
WHO recommends monitoring the PMTCT cascade using a metric that defines key indicators along the continuum of care.19 The cascade visualises the continuum of HIV care from the estimated number of pregnant women, pregnant women attending antenatal care (ANC) tested for HIV and confirmed HIV-positive pregnant women receiving ARV prophylaxis. The PMTCT cascade also follows exposed infants. However, such an approach is difficult as it requires a defined set of data for each indicator along the cascade. Few publications on PMTCT cascade over time have been published from low HIV burden settings.20 ,21 In China, there is a large number of individual studies which reported isolated indicators related to PMTCT programmes and several previous studies have attempted to integrate some of these indicators.22–25 An integrated spectrum that comprehensively reflects the continuum of PMTCT services at the national and local level has not been published in China. Based on a comprehensive review and meta-analysis, this study aims to (1) describe the chronological trends of HIV disease burden among pregnant women, HIV vertical transmission rates and coverage of PMTCT and (2) map out a PMTCT cascade that reflects the continuum of service provision for both pregnant women and infants born to HIV-positive mothers since 2003 in China. This systematic review informs relevant health policies and best practices for future HIV prevention in China and other settings with concentrated HIV epidemics.
Methods
Construction of China's PMTCT cascade
The PMTCT cascade in this study was established according to antenatal and postnatal PMTCT-related metrics reported in previous studies,26–28 but adjusted to the Chinese setting. The metrics included the percentage of pregnant women attending ANC who had an HIV test, tested positive and received ARV prophylaxis as well as the proportion of infants who received ARV prophylaxis and antibody testing at 18 months. The population size of pregnant women was calculated based on the number of live births during 2003–2011 reported by the National Bureau of Statistics of China and excluded pregnant women who underwent abortion or miscarriage.8 In China, over 90% of pregnant women attended at least one ANC visit under the free national ANC programme, but a small proportion (<10%) did not attend ANC. The percentage of pregnant women covered by ANC was obtained from the 2012 Health Statistical Abstract.29 Free HIV testing was provided as an integrated part of ANC services. HIV-positive pregnant women could make voluntary choices to either continue pregnancy or terminate pregnancy. This percentage ranged from 52% to 75% during 2003–2011 in China.23 Those who opted to continue pregnancy were recommended ARV prophylaxis for PMTCT (see online supplementary box S1), which was AZT plus a single dose of NVP prior to 2011 and a triple ARV regimen thereafter.14–16 At each step women could opt out. The women and infant who were linked to health facilities and received PMTCT-related services were assumed to be ‘in care’ in our study. In every 100 pregnancies, there were estimated 100.9 live births, which have accounted for stillbirths, perinatal mortality and multiple births at one time in China.30–33 Currently, early infant diagnosis (EID) of HIV infection among infants is not part of the standard PMTCT practices in China.16 Infants will have an HIV antibody test at 18 months.16 ,34 ,35 HIV-positive pregnant women who failed to enrol in ANC, HIV testing and ARV prophylaxis had a 31.8% (25.7%–38.6%) risk to transmit HIV to their infants.36–39 This transmission rate was used for calculating the number of cases of MTCT among HIV-positive mothers who missed ARV prophylaxis. We conducted a meta-analysis from published data to estimate key indicators at each step of the PMTCT cascade for each year during 2003–2011. An overall 9-year cascade was then constructed by summing each indicator of the individual cascades (figure 4).
Search strategy and selection criteria
Peer reviewed articles were searched from the following English and Chinese databases: PubMed and ISI Web of Knowledge, Chinese Scientific Journals Full text Database, China National Knowledge Infrastructure and Wanfang Database from 1990 to 2012. The main search keywords included HIV, mother-to-child transmission, prevention, pregnant women, infant and China. We also conducted a manual search on the reference lists of published articles and a similar keyword search on Google Scholar and Baidu (figure 1). We included all types of quantitative studies, but review articles, modelling-based studies, case reports, news, conference abstracts and commentary were excluded in this review. Non-peer-reviewed publications, including official reports, were also excluded as their study quality cannot be systematically assessed. Studies were included if they: (1) were published in Chinese or English; (2) reported any of the following indicators with sample size: for pregnant women, HIV prevalence, HIV infection mode, HIV testing percentage, uptake of ARV prophylaxis and for infants born to HIV-positive mothers, HIV testing percentage, ARV uptake and vertical transmission rate; (3) reported study period, location and recruitment venues; (4) had sample size more than 30; (5) reported that HIV infection was confirmed by western blot in one of the laboratories designated by Chinese Center for Disease Control and Prevention. A checklist with seven items was used to assess the quality of the studies.
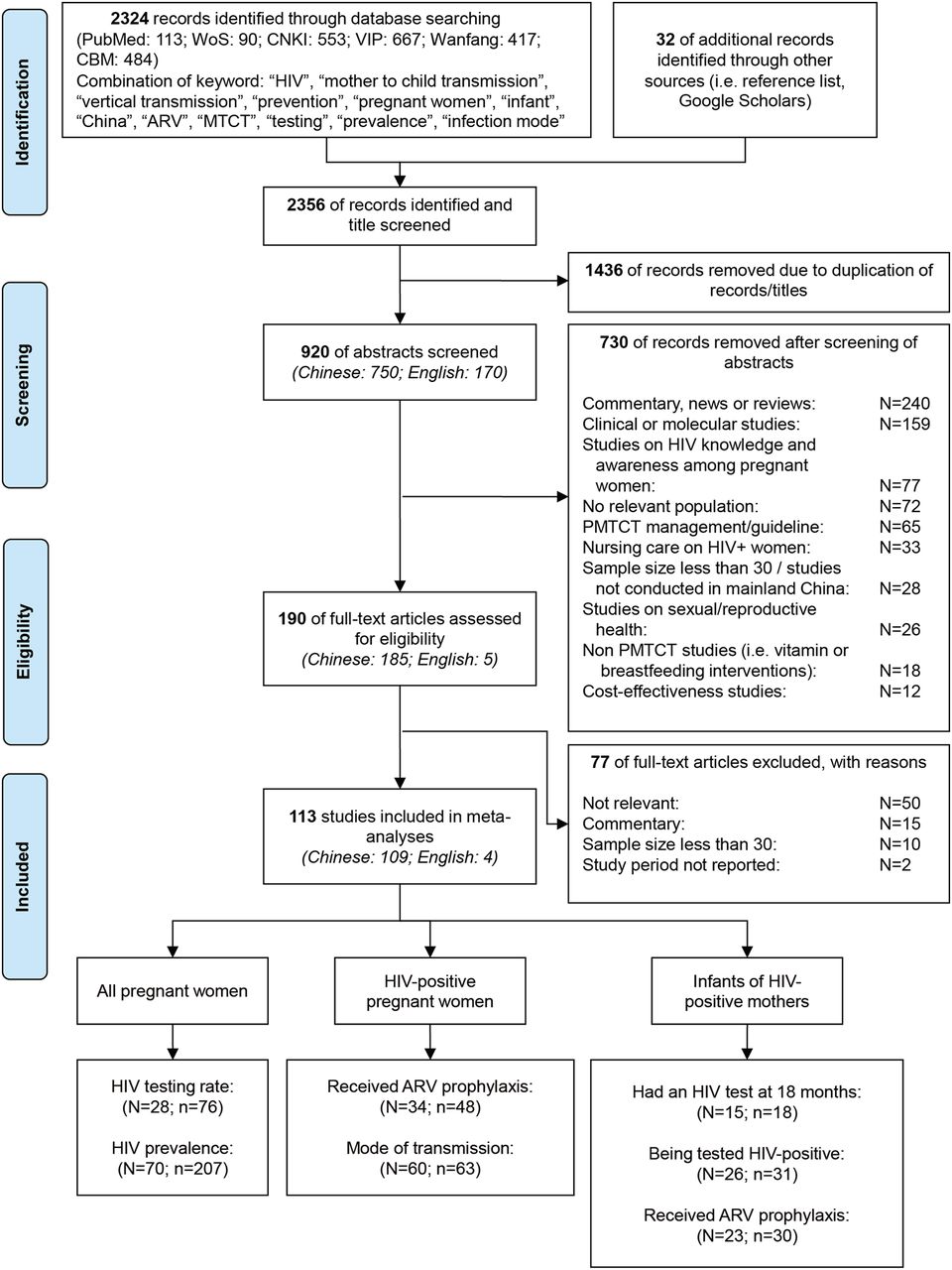
Flow chart showing the meta-analysis studies selection. ARV, antiretroviral; MTCT, mother-to-child transmission; N, the number of articles included in systematic review; n, the number of prevalence estimates included in meta-analysis; PMTCT, prevention of mother-to-child transmission.
Data extraction
Two investigators (HZ and MT, LL and XT, YZ and XL) independently identified the eligible studies for this review. Any disagreement was resolved by the senior investigators (LZ and EPFC). Data were extracted and entered into an electronic form in Microsoft Access Database (V.2007, Microsoft Corp., Redmond, Washington, USA) by HZ and were independently checked by a second investigator (EPFC). The following information was extracted from each eligible study: (1) publication details including author(s) and year of publication; (2) design of study, including type of study, study location and period, sampling method, recruitment venues, sample size and characteristics of the participants; (3) details of targeted indicators.
Statistical analyses
Meta-analyses were conducted by the Comprehensive Meta-Analysis software (V2.0, Biostat, Englewood, New Jersey). The pooled estimates and 95% CIs for each indicator were calculated by pooling the data from each study. The significance of heterogeneity across studies was measured by the Cochran Q-test and the extent of heterogeneity in the studies was measured by the I2 statistic.40 Random-effect model was selected when high and significant heterogeneity was observed across studies; otherwise, the fixed-effect model was used. Meta-regression was used to identify the significance of temporal trend and factors contributing to the high heterogeneities across the studies (see online supplementary table S2). If high heterogeneity was observed, subgroup analysis stratified by study year was performed. Potential publication bias was measured by the Begg and Mazumdar rank correlation. This study was conducted by according to PRISMA checklist (Supplementary checklist S1).
Results
Study characteristics
Among the initial 2356 records, we included 114 studies (4 in English and 110 in Chinese) for the meta-analysis (figure 1). The eligible articles covered 16 of the 31 Chinese provinces. The quality scores of the included studies are listed in online supplementary table S1, and 77.2% (88/114) of the studies scored four of eight or more. High heterogeneity was found in all investigated indicators (all p values <0.001, I2 ranged from 80.8 to 99.9), and subgroup analysis stratified by study year for each indicator was performed. No publication bias was observed (p values ranged from 0.061 to 0.273, priori cut-off=0.05) across the studies in all indicators.
Low HIV prevalence among pregnant women in China
The pooled estimate of HIV prevalence among pregnant women attending ANC in China was 0.10% during 1991–2011 (figure 2). Subgroup analysis stratified by year indicated that prevalence peaked at 0.80% in 1999 then gradually decreased and stabilised at 0.07% in the next decade. However, the variation was not significant during this period (meta-regression, p=0.104, figure 2). Heterosexual transmission (51.9%, 50.6%–53.1%) was the dominant route of transmission, followed by plasma donation (25.5%, 20.5%–22.6%) and blood transfusion (5.9%, 5.4%–6.5%; see online supplementary figure S1).
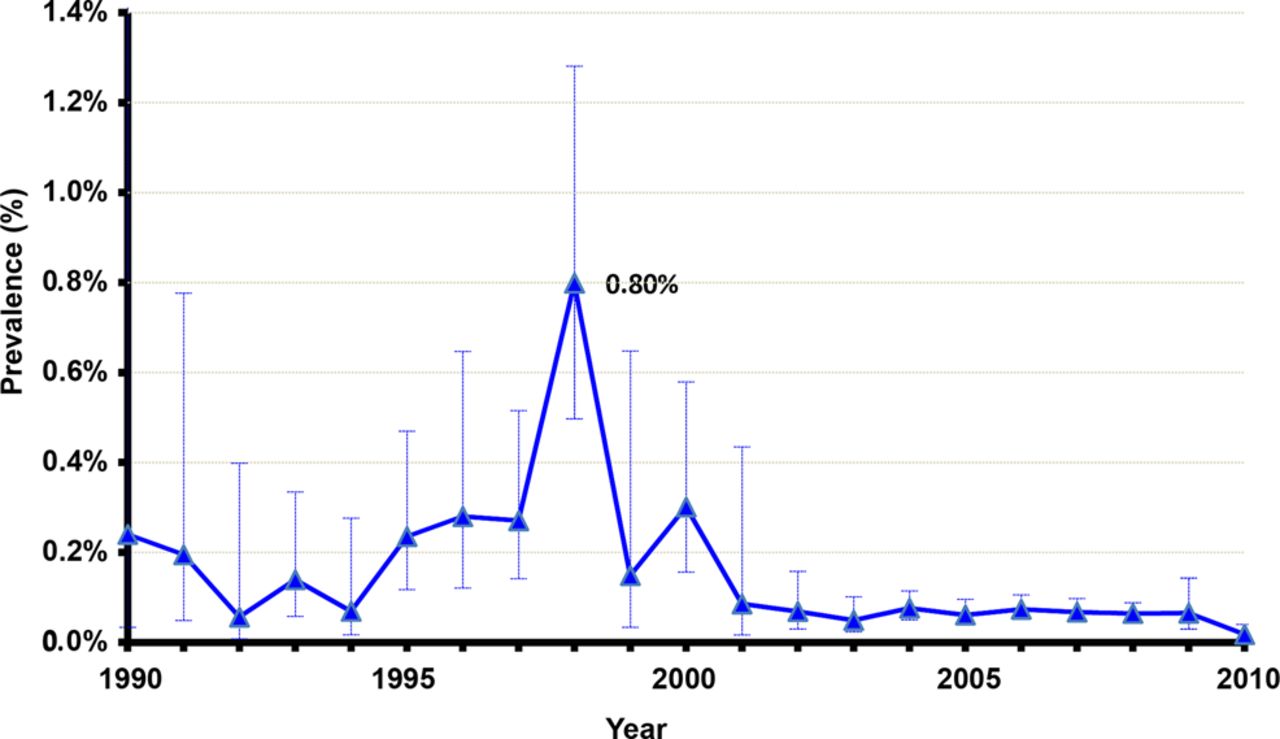
Temporal trend of HIV prevalence among pregnant women during 1991–2011 in China.
Coverage of ANC, HIV testing and PMTCT antiretrovirals
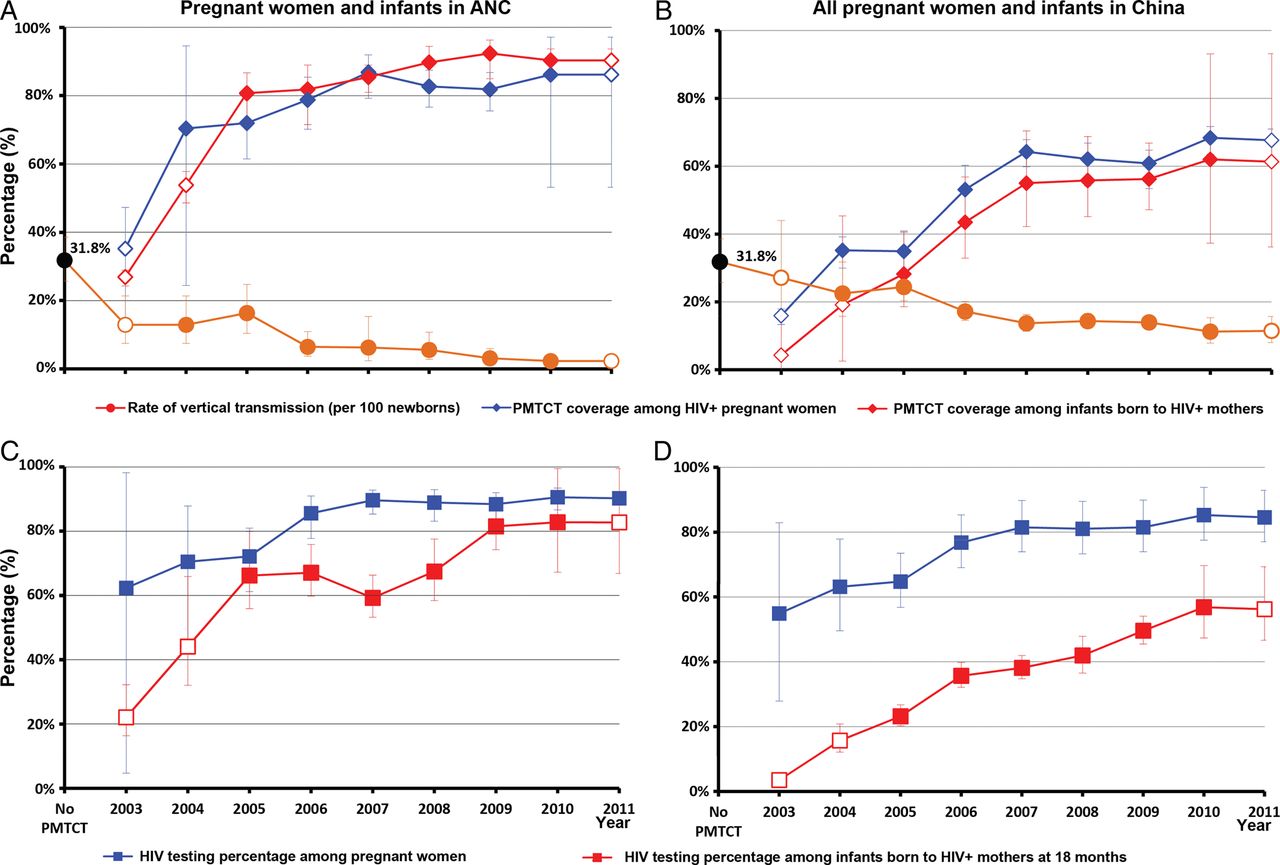
The 2012 Chinese Health Statistical Abstract reported that coverage of ANC (at least one ANC visit during pregnancy) among pregnant women increased from 88.9% in 2003 to 93.7% in 201129 (see online supplementary figure S2). Among those who attended ANC, the percentage of HIV testing uptake significantly increased from 62.4% (4.7%–98.2%) in 2003 to 90.3% (88.4%–91.8%) in 2011 (meta-regression, p=0.002, figure 3C). However, if pregnant women who did not attend ANC were included, the corresponding testing percentages were only 54.9% (27.9%–82.9%) in 2003 and 84.6% (77%–92.9%) in 2011 (meta-regression, p<0.001, figure 3D). Also, the proportion of diagnosed HIV-positive women who received ARV prophylaxis during pregnancy or at delivery increased from 35.2% (12.2%–47.3%) to 86.2% (53.2%–97.2%) during 2003–2011 (meta-regression, p=0.015, figure 3A). In comparison, ARV coverage among all HIV-infected pregnant women was estimated to be as low as 67.7% (42.5%–99.5%) in 2011, despite a substantial increase from 16.0% (8.7%–27.9%) in 2003 (meta-regression, p<0.001, figure 3B).
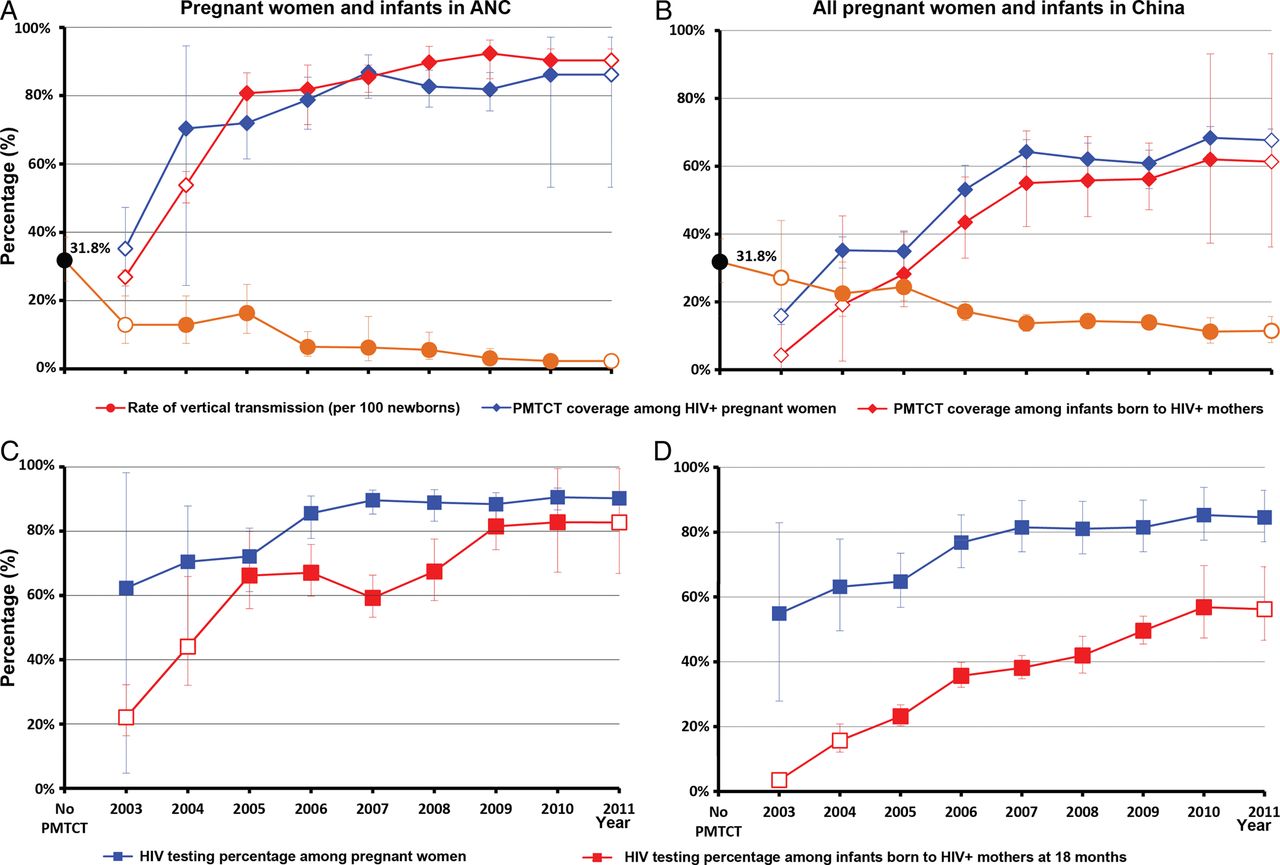
HIV testing and ARV prophylaxis coverage among pregnant women and infants who were born to HIV-positive mothers during 2003–2011 in China. The empty symbols represent interpolated values of the corresponding indicators in years where data are absent. The 95% CIs are included. ANC, antenatal care; ARV, antiretroviral; PMTCT, prevention of mother-to-child transmission.
Among HIV-exposed infants whose mothers were linked to and diagnosed with HIV in ANC, the proportion who received ARV prophylaxis significantly increased from 26.9% (24.3%–28.9%) to 90.3% (85.5%–93.7%) during 2003–2011 (meta-regression, p=0.008, figure 3A). However, while including infants born to HIV-positive mothers outside ANC, the corresponding ARV coverage was 4.3% (2.7%–7.0%) in 2003 and 61.4% (46.2%–80.5%) in 2011 (meta-regression, p<0.001, figure 3B). HIV testing percentages among infants retained in care at 18 months after birth significantly increased from 22.1% (16.3%–32.3%) to 82.8% (66.9%–100.0%) during 2003–2011 (meta-regression, p=0.001, figure 3C), while the corresponding rates were 3.5% (2.5%–5.4%) and 56.2% (46.7%–69.4%) among all infants born to HIV-positive mothers (meta-regression, p<0.001, figure 3D).
HIV vertical transmission
PMTCT programmes had an impact on mother-and-child pairs enrolled. The transmission rate decreased to 12.9% (7.5%–21.4%) in 2003 and then to 2.3% (1.4%–3.8%) in 2011, with an annual reduction of 1.7% (0.9%–2.5%, meta-regression, p=0.001, figure 3A). Nevertheless, while including mother-and-child pairs not enrolled, the corresponding rates were 27.1% (17.4%–44.0%) in 2003 and 11.5% (8.0%–15.7%) in 2011 (meta-regression, p<0.001, figure 3B).
PMTCT cascade in China during 2003–2011
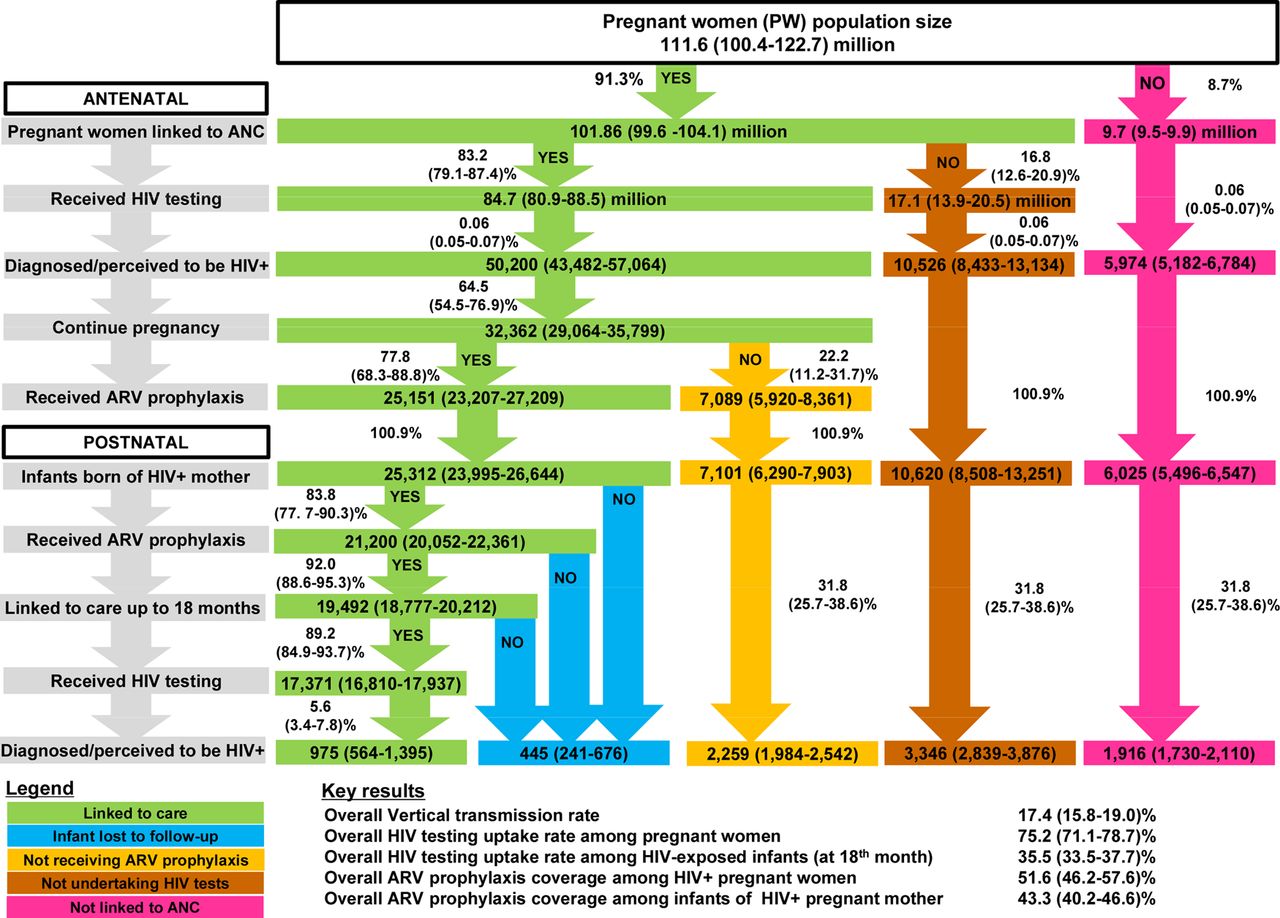
Figure 4 summarises a national PMTCT care and treatment cascade for pregnant women and children in China during 2003–2011. A total of 111.6 million Chinese women gave birth during this period. On average, 91.3% were registered in ANC, and 83.2% (79.1%–87.4%) of those had had an HIV test. Approximately 50 200 (43 482–57 064) individuals of those tested were diagnosed HIV-positive; 64.5% (54.5%–76.9%) HIV-positive women continued pregnancy and 77.8% (68.3%–88.8%) of those received ARV prophylaxis prior to or at delivery. Of the 25 312 infants born to HIV-positive mothers who decided to continue their pregnancy, 83.8% (77.7%–90.3%) received ARV prophylaxis. Among infants who received ARV prophylaxis, 92.0% (88.6%–95.3%) were retained in care (up to 18 months), and 89.2% (84.9%–93.7%) of those retained were tested for HIV. About 975 (564–1395) infants who were followed in care, were found to be HIV infected at 18 months, corresponding to an average vertical transmission rate of 3.9% (3.2%–4.6%). However, an additional 445 (241–676) infections may have occurred among infants born of HIV-positive mothers but lost to follow-up, and 2259 (1984–2542) infections may have occurred among children born to HIV-positive pregnant women who did not receive ARVs and their infants did not take ARV prophylaxis either. Further, 3346 (2839–3876) additional cases and 1916 (1730–2110) additional cases due to pregnant women who were not HIV tested and did not attend ANC, respectively, were reported (figure 4). When including these additional cases, the overall rate of vertical transmission was estimated to be 17.4% (15.8%–19.0%) during 2003–2011. Overall, only three quarters (75.2%, 71.2%–78.7%) of the pregnant women and less than half (41.5%, 39.2%–44.2%) of the HIV-exposed infants were tested for HIV. Only 51.6% (46.2%–57.6%) of the total estimated number of HIV-positive pregnant women and 43.3% (40.2%–46.6%) of their infants received ARVs for PMTCT. PMTCT cascade for each year during 2003–2011 were included in online supplementary figure S2a–S2i.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Continuum of care in the PMTCT cascade during 2003–2011 in China. ARV, antiretroviral; PMTCT, prevention of mother-to-child transmission.
Discussion
This is the first published systematic review analysing the PMTCT cascade in China. Along with the relatively low and stable HIV prevalence among pregnant women in China (<0.1% since 2002), remarkable reduction of HIV vertical transmission has been achieved through expanding PMTCT interventions following the improved national guidelines and remarkably high government investment.34 ,41 The overall trend of HIV prevalence is consistent with official reports.9 ,42 Transmission rates among mother and infants enrolled in PMTCT have decreased from 31.8% (25.7–38.6%) prior to the roll-out of PMTCT to 12.9% (7.5%–21.4%) in 2003 and 2.3% (1.4%–3.8%) in 2011. However, when including pregnant women who did not attend ANC and hence not enrolled in PMTCT, the vertical transmission rate was 27.1% (17.4%–44.0%) in 2003 and 11.5% (8.0%-–15.7%) in 2011, which is slightly higher than 7.4% reported by the 2012 progress report on PMTCT of HIV in China.17 This corresponds to similar findings published from other settings.21
Despite the marked improvements in China, gaps remain in achieving 90% coverage targets at each step of the PMTCT cascade towards reducing vertical transmission of HIV.43 The over 90% ANC coverage among pregnant women during 2003–2011 is high compared with other countries in Asia and other developing and emerging economies around the world.44–47 The low awareness of ANC and its associated benefits in isolated areas of rural China are incredible missed opportunities to improve both maternal and child health and in the prevention of paediatric HIV.48 ,49 During 2010–2011, the overall PMTCT coverage (67.7%) among all pregnant women falls short of the desired national goal of 90% in China41 and a similar global target of pregnant women receiving ARV by 2015.50 Although HIV testing has been integrated as a standard service in China's ANC system, the fact that over one-fifth of pregnant women in care did opt-out of HIV testing is alarming. Low self-perceived risk and societal stigma against HIV seem to be the major causes for women opting-out despite provision of free HIV tests.22 ,51 ,52 The current HIV testing strategies requiring confirmatory western blot at a central level may further lead to delay in pregnant women receiving their test result.53 Approximately one-quarter of the diagnosed pregnant women living with HIV either have not received any ARV prophylaxis during pregnancy or have started late during pregnancy. Similar to other resource-limited settings, loss to follow-up in antenatal care is also a major hindrance to the effectiveness of PMTCT programme.54–56
The high percentages of pregnancy termination among HIV-positive pregnant women suggest that there is still high social stigma and limited confidence in the efficacy of PMTCT interventions.57 Training of healthcare workers providing services to HIV-infected pregnant women should address factors influencing women’s decisions with regard to pregnancy termination. The late start of ARV prophylaxis during pregnancy may explain the high rates of C-section for PMTCT. It is very likely that the widespread use of infant formula in China may have resulted in the high uptake of formula feeding in the PMTCT programme.58
Provision of ARV prophylaxis to infants remains suboptimal. During 2003–2011, approximately 83.8% infants born to HIV-positive mothers in ANC received ARV prophylaxis, but this percentage falls to just 43.3% if infants born to women who did not attend ANC are included. Both percentages are comparable to those in the mothers, reflecting that care-seeking behaviours of the mothers determine their children's likelihood of receiving ARV. China's current national guidelines on PMTCT recommend HIV testing of infants born to HIV-positive mothers at 18 months after birth.41 As a result, our findings show that only around two-thirds (68.8%) of these infants eventually have an HIV test at their 18th month, whereas one-third died or were lost to follow-up. The concept of EID is recommended in the Chinese Handbook of Free ART since 2012.59 Although early diagnosis using DNA PCR viral tests has been piloted in some parts of China, so far there are limited published studies reporting the implementation and impact of EID. The studies indicate that most health facilities in a number of provinces cannot implement EID due to financial constraints as well as structural and infrastructural limitations.60
Several limitations should be noted. First, most published literature did not specify the timing of HIV testing for pregnant women; additionally, we were unable to differentiate the first time testers and re-testers, both of these would lead to an over-estimate of HIV testing coverage. Second, geographical variations in the implementation of PMTCT are likely to be substantial across the country. As published data were only available in 16 of the 31 Chinese provinces, these biases were not investigated in our meta-analysis. Also, data unavailability prevents us from differentiating between rural and urban areas. Third, most collected studies are cross-sectional with one single data point in a given year; the temporal trend provided in our findings was estimated by the pooled average of these studies in each year and may not reflect the actual trend. In particular, given the small number of PMTCT sites at an early stage of the programme, the national pooled estimates of HIV testing coverage based on limited available data may overestimate the actual percentages. Fourth, the variations in quality of reporting in selected papers may potentially affect our findings. Fifth, the included studies did not provide information on the percentage of mothers and infants who continue to receive life-long ART beyond the PMTCT programme. Also, other minor indicators, such as the percentages of women enrolled in ART voluntarily and retained in care, HIV-exposed infants who initiated cotrimoxazole by 6 weeks of age and HIV-infected infants who initiated ART were not included in our analyses. Sixth, our subgroup analysis could not fully explain the high heterogeneities in most indicators. These may be contributed by the variations in geographical locations and design of the studies and the demographic characteristics of the participants. These have not been investigated in the current scope of our study. We acknowledge that using national aggregate data could be a substantial limitation. Finally, as diagnosis of HIV-positive infants can only be confirmed at 18 months after birth, this inevitably represents substantial delay in the calculation of vertical transmission rates.
China is well poised to implement PMTCT cascade monitoring with the sophisticated electronic databases and unique health identifiers in place.61 Routine programme monitoring should be implemented at all levels for improving programme and service delivery. This systematic review shows that such cascade monitoring can be done in settings with low and concentrated HIV epidemics. The cascade promotes the use of population-based denominators to compare coverage across countries rather than using individuals registered into care as denominators. The PMTCT cascade monitoring as shown in this analysis helps in identifying bottlenecks in service delivery. There remains space for improvement for HIV testing coverage among pregnant women who are already linked to ANC, early ARV uptake among diagnosed pregnant women and early diagnosis in newborns. The exercise provides useful insights for future resource planning and allocation for PMTCT in China.
Improving PMTCT via increased integration of maternal and child health service delivery and enhancing performance of health system is perceived as a promising strategy, globally.62 ,63 Currently, a more innovative mechanism for PMTCT is taking shape in China, in which HIV prevention is integrated into maternal and children's healthcare services. PMTCT of multiple infectious diseases, including HIV, syphilis and HBV is integrated into a single mechanism under ANC services. In response to the new WHO 2013 ARV guidelines for treating and preventing HIV infection,4 China will need to substantially expand its PMTCT and ART programmes to provide life-long treatment to women of reproductive age and strengthen systems to maintain its high ANC coverage, increase uptake of HIV testing and improve retention in care. Reaching pregnant women who do not attend ANC, starting PMTCT interventions early during pregnancy and ensuring postpartum follow-up care determine the effectiveness of PMTCT.43 ,62 An integrated approach based on a cascade analysis would be important in improving provision of HIV care and treatment to pregnant women in China.
Key messages
HIV prevalence among pregnant women in China has remained very low (<0.1%) during the past decade.
Coverage of HIV testing among pregnant women attending antenatal care and ARV prophylaxis uptake among HIV-positive mothers and their babies have significantly increased during 2003–2011.
During 2003–2011, an estimated 25 000 infants were born to HIV-positive mothers who were in care in China.
During 2003–2011, HIV vertical transmission rate was 3.9% among mother–infant pairs registered in care, but was 17.4% when including transmissions occurred outside the continuum of prevention of mother-to-child transmission of HIV care.
Acknowledgments
Special thanks go to Dr Zhen Zhang of the Centre for Disease Control and Prevention of Yuzhong District, Chongqing, China, for his provision of valuable information on HIV mother-to-child transmission in China.
References
Supplementary materials
Abstract in Chinese
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Abstract in Chinese - Online abstract
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Handling editor Jackie A Cassell
Contributors Design: HZ, LZ and EPEC. Data collection: HZ, EPFC, MT, LL, XT, XL and YZ. Data analysis: HZ, LZ and EPFC. Paper writing: HZ, LZ, EPFC, Y-RL and AW. Paper revision: YZ and YW.
Funding This study was funded by China Effective Health Care Network (x7254) and 2012 Endeavour Award of Australia (ERF_PDR_3100_2012).
Disclaimer Y-RL is a staff member of the WHO. The views expressed are those of the author and should not be construed to represent the views of the WHO.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.