Article Text

Abstract
Background Gonorrhoea is increasing among men who have sex with men (MSM). We aimed to determine whether Listerine, a commercial mouthwash product, has an inhibitory effect against Neisseria gonorrhoeae in a randomised controlled trial (RCT) and an in vitro study, and therefore may be a potentially useful agent for gonorrhoea control.
Methods In vitro: a suspension of ∼108 colony forming units per mL (CFU/mL) of N. gonorrhoeae was added to a serial of dilutions (up to 1:32) of alcohol-containing Listerine mouthwashes (Cool Mint and Total Care) for 1 min. A 10 µL aliquot was spread over the surface of a gonococcal agar plate and the number of N. gonorrhoeae colonies present at each dilution was calculated. The phosphate buffered saline (PBS) was used as a control. RCT: we recruited MSM with pharyngeal gonorrhoea who returned for treatment at the Melbourne Sexual Health Centre between May 2015 and February 2016. Untreated men were randomised to rinse and gargle either Listerine Cool Mint or saline for 1 min. Pharyngeal swabs were taken before and after rinsing and gargling for culture of N. gonorrhoeae. The analysis included only men who were culture positive for N. gonorrhoeae before using the allocated solution on the day of recruitment.
Results In vitro: Listerine mouthwashes at dilutions of up to 1:4 for 1 min resulted in significant reduction of total N. gonorrhoeae counts but PBS has no inhibitory effect against N. gonorrhoeae. RCT: a total of 196 MSM were recruited, 58 (30%) were culture positive before using the solution. After gargling the allocated solution, men in the Listerine group were significantly less likely to be culture positive on the pharyngeal surface (52%) compared with men in the saline group (84%) (p=0.013).
Conclusions This data suggest Listerine, significantly reduces the amount of N. gonorrhoeae on the pharyngeal surface. With daily use it may increase gonococcal clearance and have important implications for prevention strategies.
Trial registration number ACTRN12615000716561.
- NEISSERIA GONORRHOEA
- GONORRHOEA
- INTERVENTION STUDIES
- GAY MEN
- CLINICAL TRIALS
Statistics from Altmetric.com
Introduction
Gonorrhoea cases among men who have sex with men (MSM) are increasing in many countries. In Australia, annual gonorrhoea diagnoses among men have doubled from 6892 to 11 508 over the last 5 years, and about 70% of cases are in MSM.1 These increases are occurring in the context of control programmes that have focused on screening and condom use. The implementation and scale up of biomedical interventions for HIV such as pre-exposure prophylaxis and ‘Treatment as Prevention’ has been associated with an increase in the number of sex partners and a decrease in condom use suggesting cases of gonorrhoea will continue to rise.2–4 Rising rates of gonorrhoea will also increase the risk of emergence of resistant gonorrhoea.5 ,6 A gonorrhoea control measure that does not rely on condom use is urgently needed.
Listerine is a commercial brand of mouthwash which is commonly used and available from supermarkets or chemists worldwide. The manufacturer claimed in 1879 that Listerine could be used to cure gonorrhoea in the preantibiotic era7; however, there have been no published scientific studies to assess this. The aim of these two studies was to examine first whether Listerine could be used to inhibit the growth of Neisseria gonorrhoeae in an in vitro study and then second to assess this in a randomised controlled trial (RCT). If Listerine has an inhibitory effect against N. gonorrhoeae in the pharynx, it could be a cheap, easy to use and potentially effective intervention for gonorrhoea prevention and control in MSM.
Methods
This paper describes two studies; an in vitro pilot experiment to determine the inhibitory effect of Listerine products against N. gonorrhoeae in the laboratory environment and a randomised control trial.
In vitro experiment: pilot study
We chose to evaluate two alcohol-containing Listerine products (Cool Mint and Total Care; 21.6% alcohol) because we hypothesised they would be most likely to have an inhibitory effect against N. gonorrhoeae. A standard suspension of ∼108 colony forming units per mL (CFU/mL) of a wild-type clinical pharyngeal isolate of N. gonorrhoeae was added to a series of dilutions of 1:2 to 1:32 of both mouthwashes. Phosphate buffered saline (PBS) was used as a control. After 1 min exposure, a 10 µL aliquot was removed and spread over the surface of a gonococcal (GC) agar plate (Media Preparation Unit, University of Melbourne) which was incubated at 35°C with 5% CO2 for 48 hours. The number of N. gonorrhoeae colonies present on GC agar at each dilution for each mouthwash and saline control was recorded and the corresponding CFU/mL calculated using standard methods (limit of detection 102 CFU/mL).8 Each experiment was replicated three times, and the results presented represent the mean of these three replicates.
Randomised controlled trial
Trial design and participants
The GONE (GONorrhoea Eradication) study was a parallel, open-labelled RCT conducted at Melbourne Sexual Health Centre (MSHC) between 22 May 2015 and 2 February 2016. This trial is registered with the Australian and New Zealand Clinical Trials network (ANZCTR), number ACTRN12615000716561 and is reported in accordance with the CONSORT (CONsolidated Standards of Reporting Trials) 2010 guidelines.9 Ethical approval was obtained from the Alfred Hospital Ethics Committee (number 544/14).
MSHC is the major publicly funded sexual health service in Victoria, Australia, providing about 40 000 clinical consultations annually, and about 37% of the consultations are MSM.10 MSHC provides free clinical consultations including HIV/STI screening and treatment in accordance with the Australian STI screening guidelines. As part of routine STI screening, MSM who attended MSHC were screened for pharyngeal gonorrhoea by the Gen-Probe Aptimo Combo 2 nucleic acid amplification test (NAAT), and those who tested positive for pharyngeal gonorrhoea by NAAT were contacted and asked to return for antibiotic treatment. The standard antibiotic treatment for gonorrhoea was ceftriaxone 500 mg as a single intramuscular injection and azithromycin 1 g as a single dose.
MSM returning MSHC for treatment were offered the opportunity to participate in the study if they were eligible. Eligibility criteria included: (1) men who reported any sexual contact with another man in the last 12 months; (2) aged 16 years or above and (3) tested positive for pharyngeal gonorrhoea by NAAT on the day of screening and returned for standard antibiotic treatment within 14 days. Men with symptomatic urethral gonorrhoea or those reporting contact with gonorrhoea were treated on the day of screening and were not eligible for this trial.
Randomisation and masking
The randomisation sequence was generated with Stata (V.13.1, Stata, College Station, Texas, USA) by an independent biostatistician. In the first month of the trial, participants were randomised in a 1:4 ratio with a randomised block size of 10 to receive saline (0.9% sodium chloride) or Listerine Cool Mint to encourage recruitment. However, after starting the trial we noted a low rate of culture positivity for pharyngeal gonorrhoea among men randomised into the study which meant that with a 1:4 randomisation ratio, the trial would require a larger number of participants than initially estimated. This together with feedback from participants that entry into the trial was not influenced by the probability of receiving Listerine made us reconsidered our randomisation ratio. We therefore changed to a 1:1 ratio with a randomised block size of 10 to receive saline or Listerine Cool Mint for the remaining 8 months of the trial.
Procedure
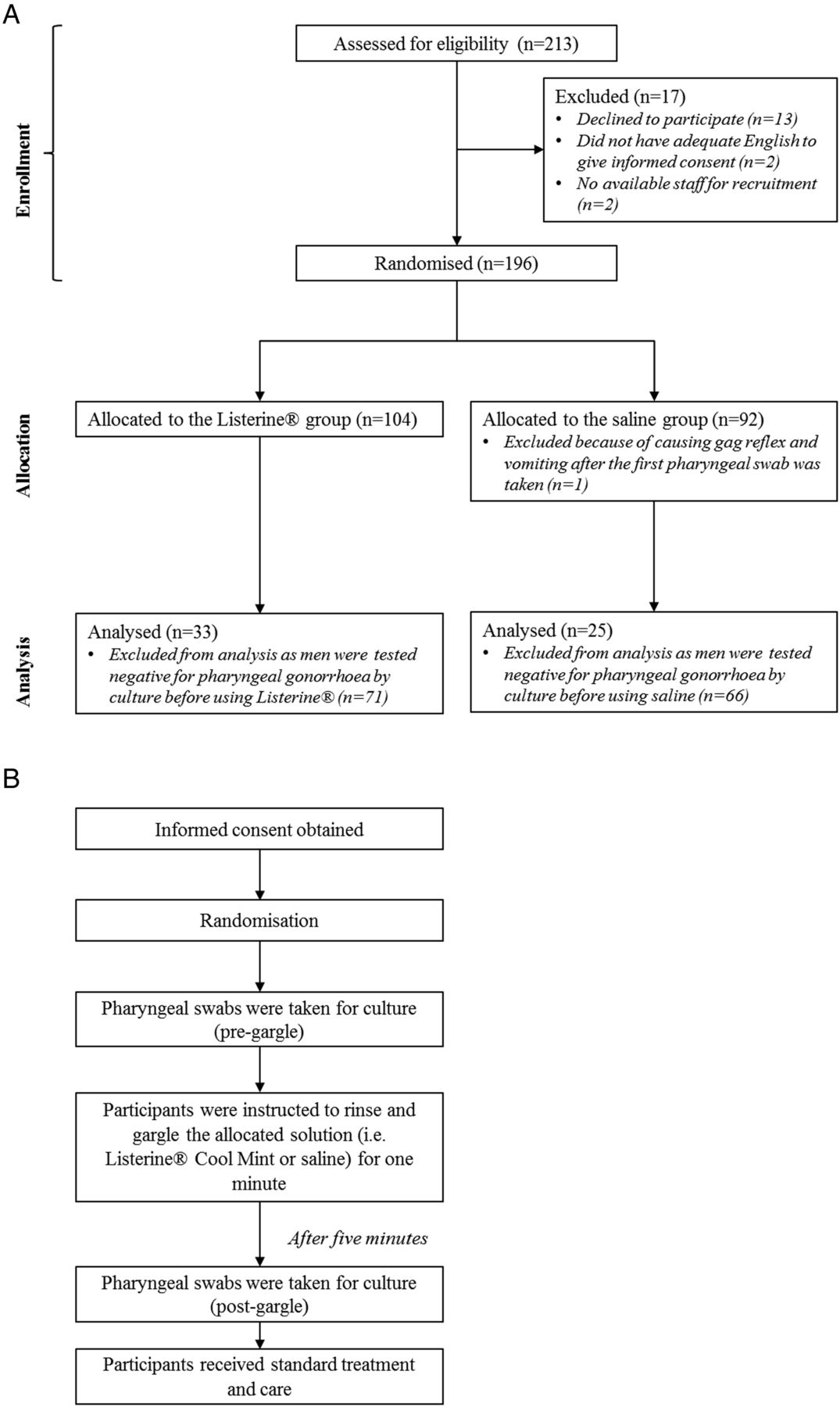
Figure 1A illustrates the study procedure of the RCT. After informed consent was obtained by experienced sexual health clinicians, a sequentially sealed and numbered envelope containing the study group allocation was opened. For both groups, two pharyngeal swabs from the participants were taken, one from the tonsillar fossae and one from the posterior oropharynx. Participants were instructed to use 20 mL of the allocated solution (ie, either Listerine Cool Mint or saline) by rinsing the oral cavity and gargling back to the oropharynx for 1 min. Five minutes after rinsing and gargling the solution, pharyngeal swabs were repeated from the tonsillar fossae and the posterior oropharynx in both groups. All pharyngeal swabs were plated onto GC agar at the point of collection for culture of N. gonorrhoeae. All participants were required to complete a questionnaire about the use of mouthwash, alcohol drinking habits and sexual history in the last 3 months. They received standard antibiotic treatment for gonorrhoea after completing the gargle, questionnaires and specimens collection and no follow-up was required.
{kind=link}
Flow diagram depicting the (A) procedure and (B) flow of the randomised controlled trial (the GONE study) among 196 enrolled men on the day of recruitment. GONE, gonorrhoea eradication.
Sample size
We assume alcohol-containing mouthwash would have a moderate effect and reduce the proportion of men who have a positive pharyngeal culture by 50% (from 80% to 40%). We did not use 100% in the control group because of the limited sensitivity of pharyngeal swabs. With these estimates we would need about 30 individuals in each arm or about 60 culture positive individuals in total at 80% power with a two-side significance level of α=0.05.
Statistical methods
Of 196 men recruited in the study, only 58 men who were culture positive for N. gonorrhoeae before using the solution (Listerine Cool Mint or saline) were included in the data analysis (specified a priori in the ANZCTR) (figure 1B). This was because the effect of Listerine or saline could not be assessed on men who were culture negative for N. gonorrhoeae on the day of recruitment. Two-tailed Fisher's exact test was used to compare the detection of N. gonorrhoeae between the Listerine and saline groups (1) on the pharyngeal surface (posterior oropharynx and/or tonsillar fossae); (2) at the tonsillar fossae and (3) at the posterior oropharynx. Other potential confounding factors such as age, frequency of mouthwash use, use of spirits and HIV serostatus were also compared between two groups. All analyses were performed using Stata (V.13.1, Stata, College Station, Texas, USA).
Results
In vitro study
Using a 1-minute exposure, and three biological replicates, both Listerine Total Care and Cool Mint were found to significantly inhibit the growth of the tested strain of N. gonorrhoeae at dilutions of 1:2 and 1:4, even with the high inoculum of 108 CFU (table 1). The PBS control displayed no inhibitory effect against N. gonorrhoeae.
Mean CFU/mL Neisseria gonorrhoeae (108 CFU/mL) to various concentrations of Listerine Total Care, Cool Mint and saline after 1 min of exposure
Randomised controlled trial
Characteristics of participants
A total of 213 men were eligible and 196 men were enrolled in the study, 104 were randomised to use Listerine and 92 were randomised to use saline (figure 1B). There was no significant difference in age, number of partners, use of spirits or mouthwash, HIV serostatus or the proportion of pharyngeal gonorrhoea culture positive on the day between the two groups at enrolment (see online supplementary table S1).
supplementary table S1
Demographic characteristics, sexual behaviours and gonorrhoea positivity among 196 enrolled men.
Of 196 men, 58 men were culture positive at either the posterior oropharynx and/or tonsillar fossae before using the solution (28 men were positive at both posterior oropharynx and tonsillar fossae, 15 were positive at posterior oropharynx only and another 15 were positive at tonsillar fossae only) (table 2). The median age of the 58 men was 27 (IQR 24–31). The median number of male sexual partners in last 3 months was 6 (IQR 3–8). Five (9%) men were HIV positive (four in the Listerine group and one in the saline group). There was no significant difference in age, number of partners, use of spirits or mouthwash, HIV serostatus and days of return for treatment between two groups (table 3).
Number of positive gonorrhoea swabs by culture among 58 men before using the solution, stratified by site of sampling
Demographic characteristics, sexual behaviours and gonorrhoea positivity among 58 men
Effect on the pharyngeal surface (posterior oropharynx and/or tonsillar fossae)
Of the 58 men included in the final analysis, 33 men were in the Listerine group and 25 men were in the saline group. Men in the saline group had a significantly higher gonorrhoea culture positivity on the pharyngeal surface (84%; 95% CI 64% to 95%), compared with men in the Listerine group (52%; 95% CI 34% to 69%) after rinsing and gargling for 1 min (p=0.013, Fisher's exact test) (table 3). Men in the Listerine group had a lower odds of being culture positive for gonorrhoea on the pharyngeal surface (OR=0.20, 95% CI 0.07 to 0.72) compared with those in the saline group 5 min after 1-minute rinse and gargle.
Effect at the tonsillar fossae
Forty-three men were culture positive at the tonsillar fossae before using the solution (table 3). Men in the saline group had a higher gonorrhoea culture positivity at the tonsillar fossae (90%; 95% CI 68% to 99%) compared with men in the Listerine group (57%; 95% CI 34% to 77%) (p=0.016, Fisher's exact test). Men in the Listerine group had a lower odds of testing positive for gonorrhoea at the tonsillar fossae (OR=0.14, 95% CI 0.03 to 0.77) compared with those in the saline group 5 min after 1-minute rinse and gargle of the solution.
Effect at the posterior oropharynx
Forty-three men were culture positive at the posterior oropharynx before using the solution (table 3). The proportion of gonorrhoea culture positivity at the posterior oropharynx among men in the saline group was 70% (95% CI 46% to 88%); while the gonorrhoea culture positivity among men in the Listerine group was 57% (95% CI 34% to 77%) after rinsing and gargling the allocated solution for 1 min, but the difference of effect was not statistically significant (p=0.277, Fisher's exact test). Men in the Listerine group had a lower odds of (OR=0.56; 95% CI 0.16 to 1.97) having a positive culture result at the posterior oropharynx compared with those in the saline group, though the difference was not statistically significant.
Discussion
The two studies presented here are the first to demonstrate Listerine can inhibit the growth of N. gonorrhoeae in vitro and in a clinical study and raise the potential that it may be useful as a control measure. If daily use of mouthwash was shown to reduce the duration of untreated infection and/or reduce the probability of acquisition of N. gonorrhoeae then this readily available, condomless and low-cost intervention may have very significant public health implications in the control of gonorrhoea in MSM. Interventions such as this are urgently needed in the context of rising rates of gonorrhoea in MSM11 and the likelihood that condom use may fall further as condom-free HIV preventions are more widely adopted.2 ,3
The main limitation of our study is the short follow-up time after mouthwash use. We did this because we considered more evidence was required before undertaking either a prevention study involving daily use (ACTRN12616000247471) over months or a large comparative treatment study. Both required convincing preliminary clinical data showing efficacy in reducing culture positivity for N. gonorrhoeae. The short follow-up period means we cannot exclude the mouthwash having only a short lived effect. However, the laboratory evidence showing a strong inhibitory effect compared with saline would suggest a longer effect. In addition, if the load of N. gonorrhoeae was reduced by the mouthwash after a single dose then one might expect that daily mouthwash over weeks would potentially reduce the viable number of N. gonorrhoeae, and hence reduce further transmission or reduce the mean duration of infection.
This study has several limitations that should be noted. First, this trial was not blinded to the research team or the participants. This could have led to a possible unconscious variation in the way the clinicians obtained pharyngeal specimens although they were not aware of the results of the in vitro laboratory study until after the trial was completed. The observation that there was no difference in the proportion of baseline swabs positive by culture in both groups and that the effect of mouthwash was limited only to the tonsillar fossae and not posterior oropharyngeal samples would argue against a systematic bias from sampling. Second, although 196 men were enrolled in the study, only 58 (30%) men with a culture positive for pharyngeal gonorrhoea on the day of treatment were included in the analysis to assess the effectiveness of mouthwash. We included only culture positive men in the analysis because we could not assess the endpoint if baseline cultures were negative. Low proportion of culture positive may due to self-limited colonisation within days.12 ,13 Third, while the in vitro laboratory study demonstrated consistent inhibition of N. gonorrhoeae at dilutions of 1:2 and 1:4, to date we have only used a single wild-type clinical isolate of N. gonorrhoeae and further testing against additional clinical and reference isolates may be valuable. Nonetheless, the results of the clinical study support the findings of the in vitro study which involved many different isolates, and further suggest that the inhibition demonstrated with a single high inoculum experiment in the laboratory is clinically relevant and important. Finally, we had a relatively small sample size that was able to identify only a moderate effect size of Listerine. We did this because it was the first study of its type and even when the study was powered for a moderate effect size we required over 200 NAAT positive cases. To assess an OR of about 0.5 would require about 200 culture positive cases in each group or nearly 600 positive pharyngeal gonorrhoea cases by NAAT which would be a much more substantial undertaking. If future studies are specifically interested in assessing the effect of mouthwash on the positivity of the posterior oropharynx (OR 0.56) alone they will require a substantially larger study than ours.
We found that the significant effect of the mouthwash was limited to the tonsillar fossae (OR 0.14) and that the effect was less marked at the posterior oropharynx (OR 0.56). Our study was designed to detect an effect size of six or more and so was not powered to detect an OR of 0.56 at the posterior oropharynx. The evidence from our RCT suggests it will be effective but it may be that more mouthwash reaches the tonsillar fossae than the posterior oropharynx during use and highlight the need to gargle and not just rinse. The different effect by site does raise the issue of whether mouthwash use will translate to a reduction in gonorrhoea carriage or prevent infection. To address this question we are currently recruiting for a study to determine if daily use of Listerine over months will reduce the risk of reinfection and are sampling men at both the tonsillar fossae and posterior oropharynx (ACTRN12616000247471).
There are some other characteristics of Listerine that suggest it could become an effective intervention if it were shown to be acceptable and effective. First, mouthwash in general is commonly available in supermarkets and most people use it, although only a minority (∼20%) use it every day. A recent study has shown that of the 10 men were asked to use Listerine at least once every day, they used it 95% of days over a 2-week period.14 Furthermore, another MSM study in San Francisco has shown that the majority of men (>90%) reporting it was easy to gargle a mouthwash.15 However, information on how mouthwash is used at a population and its' acceptability are required.
Whether a pharyngeal intervention can reduce the overall rates of gonorrhoea when it also infects the anus and urethra, depends on the contribution that pharyngeal gonorrhoea makes to the overall incidence in MSM. While theoretically gonorrhoea at asymptomatic sites has a greater opportunity to be transmitted than short lived urethral infection, this has not yet been determined. Urethral infection in any individual is mostly symptomatic and in most settings infected individuals rapidly seek healthcare.16 There is only one published model of gonorrhoea in MSM and this suggested pharyngeal transmission was important in the persistence at a population level.17
A number of studies have implicated pharyngeal gonorrhoea as an important source of both urethral and anal infection.18 ,19 A cross-sectional study has shown 34% of MSM with urethral gonorrhoea had no insertive anal sex or no unprotected insertive anal sex in the previous 3 months, suggests penile-anal sex may not be the only driver for gonorrhoea.20 Very similar results were reported from a case–control study from Seattle where 34% of urethral gonorrhoea was attributable to oral sex.21 These data are supported by a mathematical model showing gonorrhoea in MSM cannot be eliminated even with 100% of condom use for penile-anal sex.17
Our data provide preliminary evidence to support the further investigation of mouthwash as a non-condom based control measure for gonorrhoea. Listerine mouthwash is a cheap, easy to use and effective agent that inhibits gonorrhoea growth and requires further careful consideration and study.
Key messages
Dilutions of up to 1:4 resulted in significant declines in total Neisseria gonorrhoeae counts.
After rinsing and gargling men in the Listerine group were significantly less likely to be culture positive on the pharyngeal surface.
Listerine significantly reduces the amount of N. gonorrhoeae on the pharyngeal surface and therefore may be a potentially useful for gonorrhoea control.
Acknowledgments
The authors acknowledge Afrizal Afrizal for his assistance with data extraction, Tiffany Phillips and Clare Bellhouse for their assistance with data entry. We would like to thank Kerrie Stevens, Samantha Tawil and Mark Enriquez of the Microbiological Diagnostic Unit (MDU), Public Health Laboratory at the Doherty Institute, University of Melbourne for their laboratory technical expertise.
References
Footnotes
Handling editor Jackie A Cassell
Contributors CKF conceived the idea that Listerine may be used as an alternative intervention to reduce the risk of pharyngeal gonorrhoea. EPFC, CKF, SW and DL contributed to the conception and design of the randomisation controlled trial. EPFC, BPH, GF and CKF contributed to the design of the in vitro laboratory study. EPFC, SW and DL involved in data management of the randomisation controlled trial. BPH involved in the laboratory testing, data analysis and interpretation of the in vitro laboratory study. EPFC involved in data analysis and interpretation of the randomisation controlled trial. CKF, MYC and CSB assisted with the data interpretation of the randomisation controlled trial. DL, AS and SC involved in study recruitment and acquisition of data. BPH provided the overall supervision of the in vitro laboratory study, and CKF provided the overall supervision of the randomisation controlled trial. EPFC wrote the first draft of the manuscript. All authors involved in revising the manuscript critically for important intellectual content and approved the final version.
Funding This work was supported by the Australian National Health and Medical Research Council (NHMRC) programme grant (grant number 568971). EPFC is supported by the Early Career Fellowships from the Australian NHMRC (number 1091226).
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethical approval was obtained from the Alfred Hospital Ethics Committee (number 544/14).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.