Article Text

Abstract
Objectives Chlamydia trachomatis is the most commonly diagnosed bacterial STI. Lack of prevalence and risk factor data for rectal chlamydia in women has testing and treatment implications, as azithromycin (a first-line urogenital chlamydia treatment) may be less effective for rectal chlamydia. We conducted a systematic review of studies on women in high-income countries to estimate rectal chlamydia prevalence, concurrency with urogenital chlamydia and associations with reported anal intercourse (AI).
Design Systematic review and four meta-analyses conducted using random-effects modelling.
Data sources Medline, Embase, Cumulative Index to Nursing and Allied Health Literature, PsycINFO and the Cochrane Database were searched for articles published between January 1997 and October 2017.
Eligibility criteria Studies reporting rectal chlamydia positivity in heterosexual women aged ≥15 years old in high-income countries were included. Studies must have used nucleic acid amplification tests and reported both the total number of women tested for rectal chlamydia and the number of rectal chlamydia infections detected. Conference abstracts, case reports and studies with self-reported diagnoses were excluded. Data extracted included setting, rectal and urogenital chlamydia testing results, AI history, and demographics.
Results Fourteen eligible studies were identified, all among diverse populations attending sexual health services. Among routine clinic-attending women, summary rectal chlamydia positivity was 6.0% (95% CI 3.2% to 8.9%); summary concurrent rectal chlamydia infection was 68.1% in those who tested positive for urogenital chlamydia (95% CI 56.6% to 79.6%); and of those who tested negative for urogenital chlamydia, 2.2% (95% CI 0% to 5.2%) were positive for rectal chlamydia. Reported AI was not associated with rectal chlamydia (summary risk ratio 0.90; 95% CI 0.75 to 1.10).
Conclusions High levels of rectal chlamydia infection have been shown in women with urogenital chlamydia infection. The absence of association between reported AI and rectal chlamydia suggests AI is not an adequate indicator for rectal testing. Further work is needed to determine policy and practice for routine rectal testing in women.
- chlamydia trachomatis
- meta-analysis
- systematic reviews
- screening
- women
Statistics from Altmetric.com
Introduction
Chlamydia trachomatis (CT) is the most commonly diagnosed bacterial STI in high-income and middle-income countries, primarily infecting urogenital and rectal mucosa.1 2 Failure to identify and treat urogenital CT can result in serious sequelae such as pelvic inflammatory disease, tubal scarring, ectopic pregnancy and infertility.1 3 Rectal CT infection is largely asymptomatic, and is associated with increased risk of HIV transmission and acquisition.4 5 High concurrency of rectal and urogenital CT in men and women has been observed in some studies, suggesting significant numbers of rectal CT cases may be missed by genital testing alone.6–9
The clinical significance of rectal CT infection in women is unclear, as the risks of long-term sequelae following a rectal infection in women are unknown.9 A positive nucleic acid amplification test (NAAT) result may not represent viable organisms emerging from rectal mucosal intracellular CT infection (a true infection), and instead be indicative of contamination of either DNA or CT organisms from the urogenital tract to the rectum. However van Liere et al 10 have shown comparable bacterial loads in rectal and in urogenital swabs, supporting the premise that detection of CT in the rectum can indicate a biological infection rather than contamination in women with and without a history of anal intercourse (AI). Henceforth, we assume that a positive test means an established CT infection. Undiagnosed, untreated and undertreated rectal CT infections constitute a potential reservoir of CT, and given the possibility of autoinoculation of CT from the rectum to the urogenital tract11 12 may impede effective treatment and transmission prevention.
A recent meta-analysis and other work suggest that azithromycin, a first-line treatment for uncomplicated urogenital CT, may only be around 80% effective when treating rectal CT.2 13 14 Consequently, the WHO and the BASHH recommend doxycycline as the preferred treatment for rectal CT, with the former specifically recommending doxycycline if AI is reported.2 15 In England, 11% of women aged 16–74 years reported AI in the previous year. There is inconsistent evidence for history of AI as a rectal CT indicator.9 16–20 However, WHO guidelines currently recommend that a history of AI guide the decision to test for rectal CT.15
Many countries have policies for opportunistic urogenital CT testing and treatment, such as the National Chlamydia Screening Programme in England, which tests approximately 1.7 million people aged 15–24 and identifies around 140 000 infections annually.1 21 22 Having unidentified reservoirs of rectal CT in women tested only for urogenital CT risks reduced effectiveness and cost-effectiveness of these CT control programmes.
We conducted a systematic review and meta-analyses of studies measuring rectal CT positivity in women in order to estimate rectal CT prevalence, concurrency with urogenital CT and the association between rectal CT and reported history of AI.
Methods
Search strategy and selection criteria
We searched electronic bibliographic databases—Medline, Embase, Cumulative Index to Nursing and Allied Health Literature, PsycINFO and the Cochrane Database—from 1 January 1997 to 2 September 2015 using free-text terms and medical subject headings combining all terms for CT, prevalence, positivity, epidemiology, diagnosis, and rectal, anal or anogenital (online supplementary material 1). Additionally, we hand-searched references of included papers for other relevant papers. Conference abstracts were not included. Using the same method, we undertook an additional Medline search between 1 January 2015 and 17 October 2017 to ensure that all relevant recently published articles were included in the review.
Supplementary file 1
We included cross-sectional studies of general and clinic-attending populations, which could be nested in cohort studies or randomised controlled trials, involving heterosexual women aged ≥15 years who were tested for rectal CT. Studies must have used NAATs and reported both the total number of women tested for rectal CT and the number of rectal diagnoses. Case reports and studies with self-reported diagnoses were excluded. Studies were limited to those conducted in high-income countries (defined by the Organisation for Economic Co-operation and Development), as these countries were most likely to have similar healthcare provision and CT epidemiology.
Abstracts and full texts were independently reviewed by two reviewers for eligibility. Disagreements were resolved with a third reviewer. Where necessary, study authors were contacted for more information.
Data were extracted independently by two reviewers, compared and discrepancies resolved with a third reviewer. Data extracted included information on study design, inclusion criteria, outcome of interest and funding information (online supplementary material 2). Urogenital and rectal infections were defined as a positive NAAT from a site-specific swab which was not part of a pooled sample. We assume that a positive rectal swab for CT in a woman represents an active and established rectal CT infection. Data were extracted from papers that reported any history of AI by rectal CT test result (AI not specifically defined).
Risk of bias was assessed by two independent reviewers using a published tool adapted from Hoy et al 23 to determine whether included studies would present a biased estimate of population prevalence. The tool assesses risk of bias using structured questions to appraise internal and external validity of each study. The reviewers collated their evaluations of each paper and agreed on an overall risk for each paper.
Data analysis
The positivity of rectal infection among participants in each study was calculated, defined as percentage of women with a rectal CT infection among all women in the study tested for rectal CT.
Four meta-analyses were conducted, using random-effects models to calculate the following:
summary estimates of rectal CT positivity across all studies stratified by tested population or clinical subgroup: (1) routine clinic attenders (not defined as high-risk as below), n=3; (2) women of high risk (sexual contacts of gonorrhoea-positive individuals, had symptoms, victims of sexual assault, had sexual contact with someone diagnosed with CT, or were being followed up for CT and adult film industry performers), n=4; (3) women who were tested only because they reported a history of AI, n=5; (4) women who were tested for rectal CT because they were positive for urogenital CT, n=1; and (5) women who were all HIV-positive, n=1
summary estimates of proportion of women with rectal CT among women who were positive for urogenital CT in all appropriate studies and among studies reporting routine clinic attenders; these women represent a population who may have an undiagnosed rectal CT infection but have treatment directed towards their urogenital CT infection which may not be the recommended first-line treatment for rectal CT (doxycycline), hereafter we refer to this as ‘less effectively treated’
summary estimates of proportion of women with rectal CT among those negative for urogenital CT in all appropriate studies and among studies reporting routine clinic attenders, as a measure of potential undiagnosed rectal infection among those tested
summary risk ratio (RR) for being rectal CT-positive in women who had reported a history of AI in order to determine the utility of reporting AI as an indicator for rectal testing.
Where heterogeneity was high (more than 75%), summary estimates are not reported (with exception of routine clinic-attending women), and only a range and median average of the results are reported.
Additional data were extracted on specimen type and site tested (online supplementary material 3), but were not analysed to determine association with positivity.
All meta-analyses were undertaken using STATA V.13, using the metaprop (analyses 1–3) and metan (analysis 4) commands. We tested for variation in estimated proportions (analyses 1–3) or RR (analysis 4) attributable to heterogeneity using the I2 statistic and estimated between-study variance using the Τ2 statistic. A fixed continuity correction of 0.5 was added in cases where a study had a zero result, to ensure all studies could be included, where appropriate, in analyses.24 25
Results
From 681 unique references identified from the database search, 14 studies were included in the meta-analyses (figure 1): 12 cross-sectional studies and 2 observational cohort studies (table 1). Of these 14 studies, 5 only tested women for rectal CT if they had reported a history of AI8 26–29; 1 conducted only among HIV-positive women30; 1 conducted only among urogenital CT-positive participants9; 1 conducted among adult film industry performers31; 3 studies tested clinic attendees considered to be high risk (defined as women who were sexual contacts of gonorrhoea-positive individuals, had symptoms, were victims of sexual assault, had sexual contact with someone diagnosed with CT or were being followed up)7 32 33; and 3 studies included all eligible routine clinic attendees.16 17 34 All studies identified were of women attending sexual health settings, and no studies conducted among a general population sample were identified.

Flow chart depicting the selection of studies for inclusion in the review process. NAAT, nucleic acid amplification test.
Study characteristics and rectal chlamydia positivity of all included studies (n=14)
Using the adapted risk-of-bias tool,23 all studies were considered to have an overall high risk of bias in measuring population prevalence given that they each sampled from specific groups, which is unlikely to represent the general population of sexually active women in their respective countries. Some answers varied by reviewer, but the overall risk was found to be the same (online supplementary material 4).
No study provided an estimated population prevalence of rectal CT. Among all 14 studies, rectal CT positivity ranged from 1.7% to 77.3% with a median of 8.9% (table 1). Due to the high heterogeneity between studies (I2 =97.2%, Τ2 =0.01), a summary estimate was not calculated for all studies.
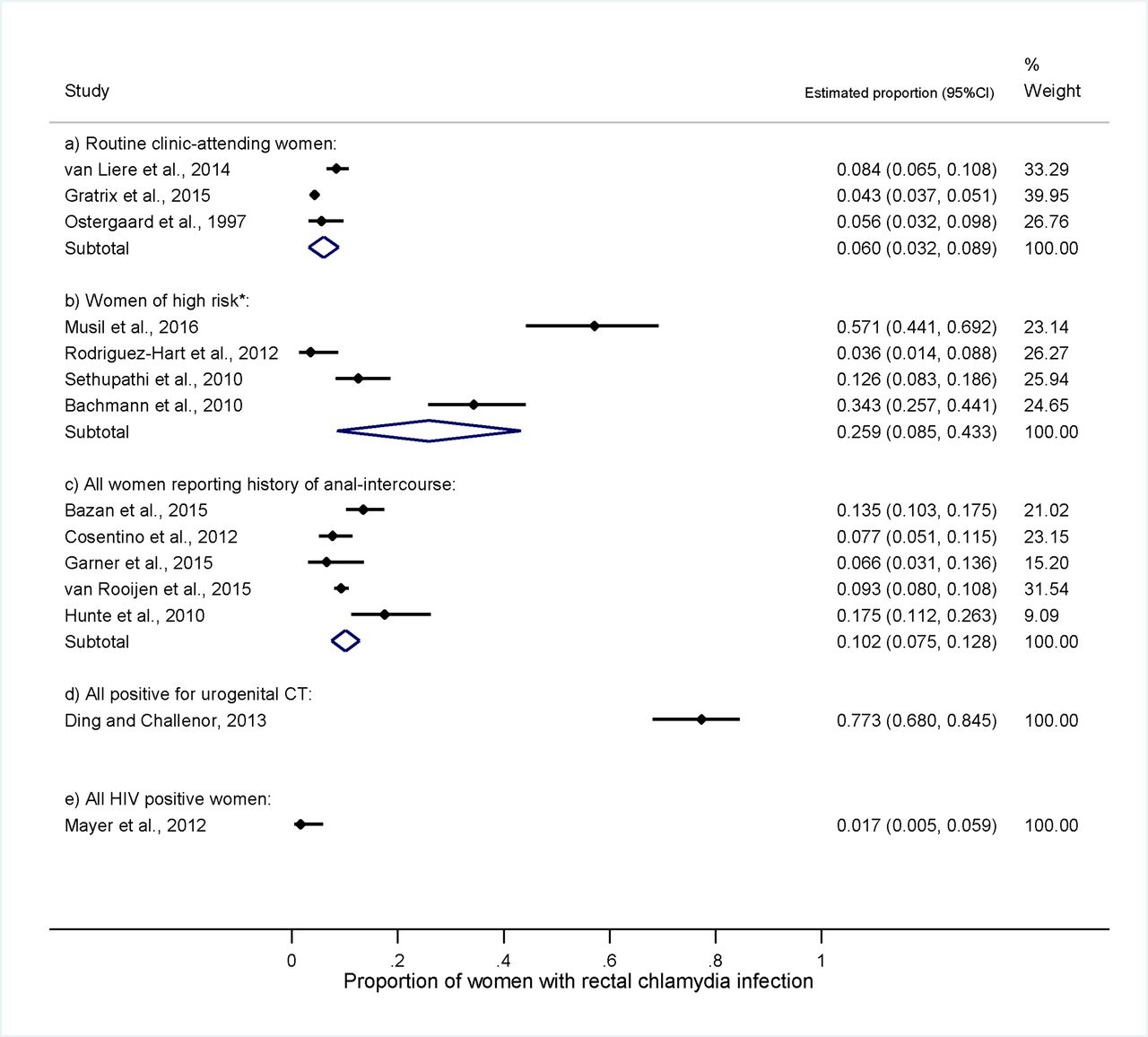
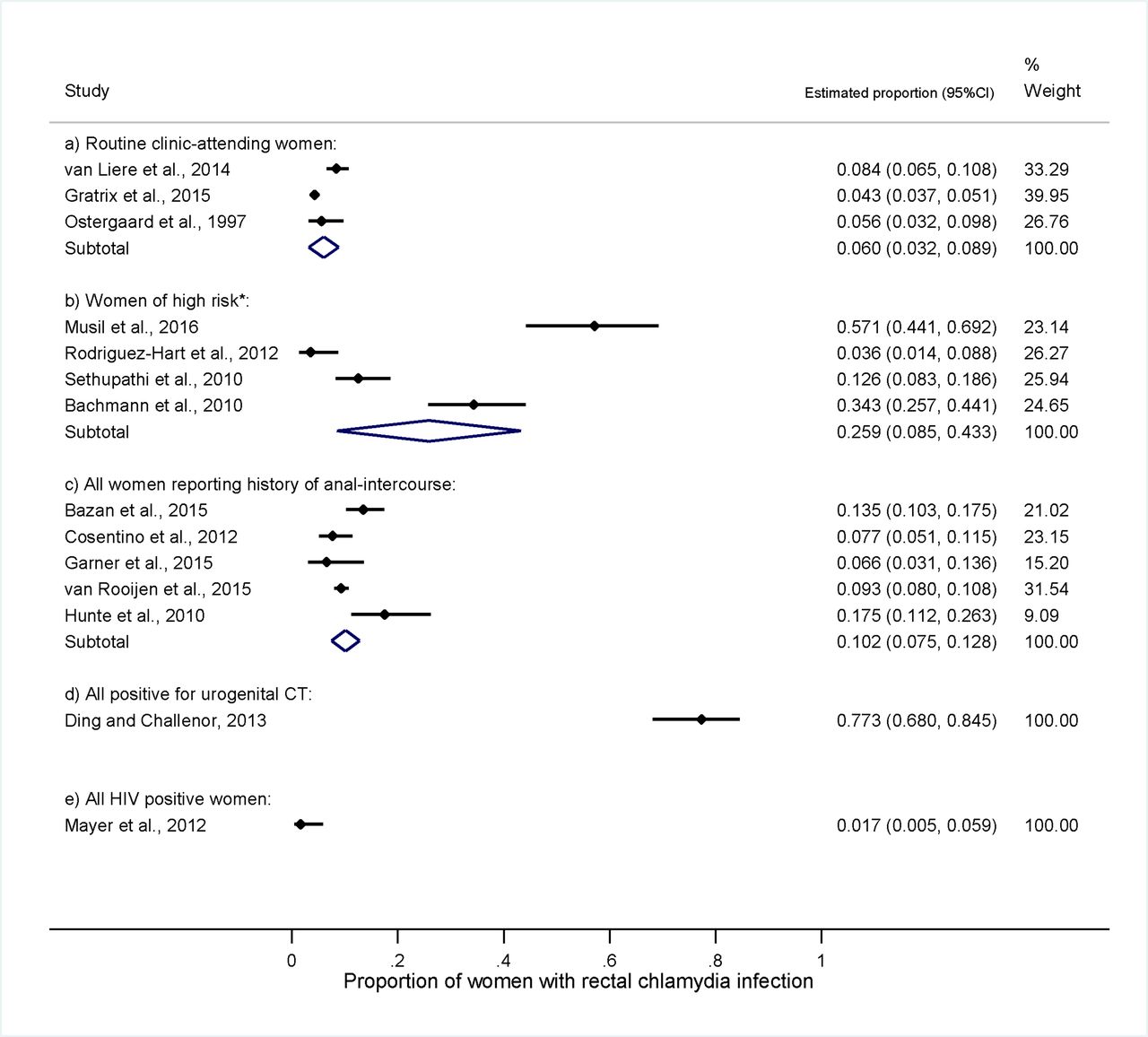
For the studies reporting routine clinic-attending women, although high heterogeneity was seen across the three studies, the subgroup summary estimate for rectal CT positivity was 6.0% (95% CI 3.2% to 8.9%, I2 =84.6%, Τ2 =0.01). For the studies where all women reported a history of AI, the summary estimate for rectal CT positivity was 25.9% (95% CI 8.5% to 43.3%, I2 =65.2%, Τ2 =0.00) (figure 2).
{kind=link}
{kind=link}
Individual study and study subgroup summary estimates of rectal chlamydia positivity in women stratified by clinical subgroup/population type (n=14). The diamonds represent the summary proportions and CIs by subgroup. *Women of high risk category includes sexual contacts of gonorrhoea-positive individuals, had symptoms, were victims of sexual assault, had sexual contact with someone diagnosed with CT or were being followed up, as well as adult film industry performers (potentially high risk due the number of sexual events, however safe-sex and sexual health testing practice is unknown). CT, Chlamydia trachomatis.
Ten studies reported testing for urogenital CT and rectal CT.7–9 16 17 27 31–34 Among these studies where all women were tested for rectal CT and urogenital CT, a concurrent infection was found in 3.6%–81.5% (median, 11.8%) (table 2). Among studies where women were positive for CT regardless of site of infection, concurrent urogenital CT and rectal CT was found in 40.9%–100% (median, 78.5%; calculated using columns from table 2 A/(A+B+C)). In studies in which women were positive for rectal CT, a concurrent urogenital CT infection was found in 62.9%–100% (median, 94.3%; A/(A+C)) (table 2).
Data extracted from studies reporting women tested for urogenital chlamydia and/or studies reporting a history of anal intercourse rectal
High heterogeneity was found between the 10 studies (I2 =80.9%, Τ2 =0.01). The proportion of women having a rectal CT infection among those positive for urogenital CT ranged between 45.0% and 100%. This range represents a worst-case scenario of women at risk of being less effectively treated (ie, women with undiagnosed rectal CT who do not receive the recommended first-line treatment for rectal CT) (online supplementary material 5a). The summary estimate of rectal CT infection among those positive for urogenital CT across studies reporting only routine clinic attenders was 68.1% (95% CI 56.6% to 79.6%, I2 =70.9%, Τ2 =0.03).
A summary estimate among those who tested negative for urogenital CT was not provided due to the high heterogeneity (I2 =91.0%, Τ2 <0.0001). The proportion of women with a rectal CT infection among women who tested negative for urogenital CT ranged from 0.0% to 11.5%. This range represents the potential proportion of women with a CT infection who may have been undiagnosed and untreated (online supplementary material 5b). Although a high heterogeneity was found, the summary estimate for studies reporting only routine clinic attenders was 2.2% (95% CI 0% to 5.2%, I2 =97.3%, Τ2 =0.001).
Eleven studies had information on history of AI.7–9 16 17 26–29 32–34 The definition of ‘history of AI’ was inconsistent across the studies or not specified. Among all women who were tested for rectal CT, 2.0%–30.4% (median, 9.1%; F/J) had a positive test and reported AI (table 2). Among all women who had a positive rectal CT infection, between 13.5% and 100% (median, 51.6%; F/(F+H)) reported AI. However these included five studies that only tested women who reported AI; without these five studies,8 26–29 the range is 13.5%–50.0% (median, 29.1%) (table 2).
The calculated summary RR for a history of AI as a risk factor for rectal CT was 0.90 (95% CI 0.74 to 1.10, I2 =5.6%, Τ2 =0.004) (online supplementary material 6).
Discussion
The systematic review and meta-analyses of 14 studies found a summary estimate of rectal CT positivity of 6.0% among routine clinic-attending women in high-income countries. However, because of high heterogeneity and bias due to the populations sampled, this is a likely overestimate of population prevalence of rectal CT in women. We calculated that 68.1% of routine clinic-attending women infected with urogenital CT also had rectal CT, which is important for treatment implications, as azithromycin is a recommended first-line treatment for urogenital CT but is less effective for rectal CT. Of routine clinic-attending women without urogenital CT, 2.2% had a rectal CT infection, which would go undetected if they only have urogenital testing. Most interestingly, this analysis did not find a relationship between rectal CT and reported AI, and therefore we believe that currently there is insufficient evidence to guide practice on using reported AI as an indicator for rectal testing, as recommend by WHO guidelines.15
A key strength of our study is that we employed a robust methodology to search for and review papers following an a priori protocol with clear inclusion and exclusion criteria. We searched several databases, assessed papers for risk of bias and undertook double extraction. Our findings are subject to limitations, arising from the nature of included studies. First, estimates cannot be applied to the general population as all 14 studies included women attending sexual health services, limiting the generalisability. Second, sexual health clinic populations varied, thus limiting comparability. Third, there was no consistent definition of history of AI so findings should be interpreted with caution. Similarly, ‘high-risk’ women were inconsistently defined.
This is the first systematic review of the prevalence of rectal CT in heterosexual women in high-income countries. A non-systematic review of the literature on extragenital infections showed similar findings for rectal CT positivity and also highlighted that extragenital infections are often found in the absence of reported risk behaviours such as AI.6 However, the authors did not calculate an estimate for concurrent urogenital CT or RR for AI and rectal CT.
The uncertainty regarding rectal CT infections representing true infections versus contamination could not be taken into account in this review given that included studies did not undertake any testing method to rule out contamination.
Although questions remain about the meaning of a rectal CT diagnosis, our study raises some important issues concerning CT testing and treatment policies. We found that a summary estimate of 68.1% of routine clinic-attending women with urogenital CT had concurrent rectal CT. While the relative efficacy of azithromycin versus doxycycline for rectal CT in women has not been definitively established, a high proportion of routine clinic-attending women may be subject to less effective treatment, if given azithromycin directed at their urogenital infection in the absence of rectal testing. Assuming our estimate to be true and combining it with a previous estimate of azithromycin effectiveness for rectal CT of 82.9% (95% CI 76.0% to 89.8%)14 suggests that among routine clinic-attending women diagnosed with urogenital CT, only approximately half (56%; calculated by 68.1% multiplied by 82.9%) would receive adequate treatment if their rectal infection remained undiagnosed and they had received azithromycin. Furthermore in approximately 12% (calculated by 17.1% multiplied by 68.1%), treatment would have failed. In genitourinary medicine clinics in England 2015, there were 794 168 CT tests and 50 708 diagnoses reported among women (all ages).35 Applying our results to this surveillance data shows the potential scale of less effective treatment (diagnoses multiplied by 56%) in women attending sexual health services. If we assume all tests and diagnoses were for urogenital CT only, and that azithromycin is prescribed, in this scenario, approximately 28 400 CT infections may have been less effectively treated and approximately 6000 infections would fail to be treated (diagnoses multiplied by 12%). However, in practice, some clinicians are likely to further assess the need for rectal CT testing (eg, through history of AI) and manage accordingly so fewer infections are likely to be at risk of less effective treatment.
Furthermore, our finding that an estimate of 2.2% of routine clinic-attending women without a urogenital CT infection had rectal CT suggests a number of rectal CT infections could be missed even among those actively engaged in testing. Among all studies with available data, only 13.5% of rectal CT detected were among women reporting AI. Therefore, limiting testing and treating for rectal CT to women reporting a history of AI or rectal symptoms (as recommended by current guidelines) could miss a significant number of rectal infections, which has potential implications for current CT control programmes.
These findings suggest that less effective treatment and missed diagnoses in women may be occurring on a considerable scale. However the clinical significance of missed and untreated rectal CT in women is still uncertain. Furthermore, the potential impact of less effective treatment may not be as great because in practice, some women receive doxycycline as first-line treatment for urogenital CT; currently this proportion is unknown.
From our findings it is clear that current evidence is insufficient to make a robust recommendation regarding routine rectal CT testing in women across settings and the use of history of AI as a reliable indicator, highlighting the need for further research. While the evidence is limited, rectal testing could be done in women who repeatedly present with a urogenital infection within 3–6 months of treatment. Current BASHH guidance in the UK on the management of CT infection states that those who test positive should be retested after 3 months to identify reinfection.2 Positive tests at this stage could be tested for rectal infection or simply treated for rectal infection. High rates of concurrent rectal and urogenital CT are not enough to warrant the use of doxycycline rather than azithromycin for first-line treatment of women with urogenital CT; however, a randomised controlled trial of azithromycin versus doxycycline in women for the treatment of rectal CT would determine whether individuals with a diagnosed urogenital CT infection but undiagnosed rectal CT who are treated with azithromycin are being treated suboptimally. Data on current prescribing (azithromycin or doxycycline for urogenital CT) and extragenital testing practices in specialist and non-specialist settings would add understanding to the scale of potential less effective treatment. High-income countries with national testing and treatment policies also require a robust estimate of rectal CT among their target populations. Biological studies on bacterial viability as well as non-urogenital sources of rectal CT infection such as orally acquired12 36 would further allow implications of rectal CT to be better understood. Studies to ascertain feasibility, costs and acceptability of different testing strategies are also needed to understand how rectal testing may best be incorporated into clinical pathways. It would be interesting to determine if other clinical practices such as who obtains the sample, specimen type and the invasiveness of the swab affect the positivity rate of rectal chlamydia. Finally, there is a need for studies to determine the significance of rectal CT in women by understanding the natural history and complications associated with rectal CT.
In conclusion, we have found evidence that a substantial proportion of women attending sexual health clinics are infected with rectal CT and that the infections risk being missed or less effectively treated. Further work is needed to determine the feasibility of and criteria for routine rectal testing in women.
Key messages
Currently there are no definitive estimates of the prevalence of rectal chlamydia, of concurrent rectal and urogenital chlamydia infection, or of the relationship between anal intercourse and rectal chlamydia infection.
This systematic review found high rates of concurrent rectal infection in women with urogenital infection and no evidence that a history of anal intercourse is a reliable indicator for rectal chlamydia infection.
Using reported anal intercourse as an indicator for rectal testing is likely to lead to missed diagnoses of rectal infections.
References
Footnotes
Handling editor Nicola Low
Contributors SCW, STS, JMS, EMH-E, KF and JKD had the initial idea and concept of undertaking this systematic review. JMS and SCW developed the idea and wrote the study protocol which laid out the search strategy and study design. NLC undertook the literature search and reviewed the titles. NLC, KT, CB and KF reviewed the abstracts and full-text papers. JMS and JKD evaluated the included papers for risk of bias. NLC, CB and KF extracted and collected the data. NLC designed and undertook the meta-analyses, with contributions from all authors. NLC wrote the first draft of the paper and developed the figures. All authors contributed to the writing of the manuscript and approved the final version.
Funding Project funded by Public Health England, the UKCRC Translational Infection Research (TIR) Initiative supported by the Medical Research Council, eSTI2 Consortium (grant number G0901608), and the National Institute for Health Research (NIHR) i4i Programme (grant number II-LB-0214-20005). The funding bodies had no role in the design of the study, in the writing of the manuscript and in the decision to submit the manuscript for publication. The views expressed are those of the authors and not necessarily those of the NIHR, the NHS or the Department of Health.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data available.