Article Text

Abstract
Objectives: To investigate whether the prevalence of HIV infection among young people, and sexual behaviours associated with increased HIV risk, are differentially distributed between students and those not attending school or college.
Design: A random population sample of unmarried young people (916 males, 1003 females) aged 14–25 years from rural South Africa in 2001.
Methods: Data on school attendance and HIV risk characteristics came from structured face-to-face interviews. HIV serostatus was assessed by oral fluid ELISA. Logistic regression models specified HIV serostatus and high-risk behaviours as outcome variables. The primary exposure was school attendance. Models were adjusted for potential confounders.
Results: HIV knowledge, communication about sex and HIV testing were similarly distributed among students and non-students. The lifetime number of partners was lower for students of both sexes (adjusted odds ratio (aOR) for more than three partners for men 0.67; 95% CI 0.44 to 1.00; aOR for more than two partners for women 0.69; 95% CI 0.46 to 1.04). Among young women, fewer students reported having partners more than three years older than themselves (aOR 0.58; 95% CI 0.37 to 0.92), having sex more than five times with a partner (aOR 0.57; 95% CI 0.37 to 0.87) and unprotected intercourse during the past year (aOR 0.60; 95% CI 0.40 to 0.91). Male students were less likely to be HIV positive than non-students (aOR 0.21; 95% CI 0.06 to 0.71).
Conclusions: Attending school was associated with lower-risk sexual behaviours and, among young men, lower HIV prevalence. Secondary school attendance may influence the structure of sexual networks and reduce HIV risk. Maximising school attendance may reduce HIV transmission among young people.
Statistics from Altmetric.com
By 2005, 25 million people were living with HIV in sub-Saharan Africa, some two-thirds of the world’s total. After years of increase, HIV prevalence has recently been stable or declining in many countries, although it is still increasing in South Africa.1 HIV prevalence declines have been attributed to lower HIV incidence and changing sexual behaviour in some settings.
Average education levels are low in sub-Saharan Africa and HIV/AIDS has been characterised as a disease of poverty and lack of education. Studies conducted up to the mid-1990s, however, showed greater levels of HIV infection among the more educated,2–6 in both urban and rural areas and among men and women.7 This was probably because more educated individuals engaged in larger, more risky sexual networks as a result of their greater mobility and higher socioeconomic status.8 9
The association between education and HIV may, however, change over time. Increasingly, empirical data support this hypothesis. Studies from some countries report reductions in HIV prevalence among the most educated, alongside stable or rising prevalence among those with less education.5 10–14 This pattern has been attributed to the faster adoption of protective behaviours by the more educated. Other studies have reported greater levels of condom use among the more educated.15–17
Studying the association between education and HIV risk is complex. Among older groups, educational attainment is associated with greater mobility and income that may in turn affect HIV risk. Among the young, individual socioeconomic changes have not had time to accrue, thus the effect of education may be directly related to school attendance, perhaps by influencing sexual network characteristics or access to health services. School attendance might, however, also be associated with household wealth and analyses should take account of this.
We investigated the association between school attendance, HIV infection and other outcome variables representing high HIV risk among unmarried 14–25-year-old individuals in rural South Africa. We hypothesised that school attendance would be associated with lower HIV prevalence and lower-risk sexual behaviour and explored evidence for the mechanisms through which associations might be mediated.
METHODS
Setting
The study was conducted in 2001 in eight villages purposively selected for inclusion in a cluster-randomised trial of a social intervention in the rural Limpopo province of South Africa.18 19 Poverty remains widespread in the study area,20 unemployment rates exceed 40%,21 and there are high levels of labour migration.22 HIV prevalence among antenatal clinic attenders in the region was 13.2% in 2000.
There was at least one primary and one secondary school in all but one of the study villages. School fees averaged USA$20 per year. Secondary school attendance beyond the age of 18 years was common. School-based programmes aimed at improving the sexual health of young people were, however, poorly developed at the time of the study.
Data collection
Two hundred households were randomly selected within each village, and unmarried individuals aged 14–25 years recorded as household members were eligible for inclusion in the current analysis. Married individuals were excluded because marriage was rare, particularly among young men, and because married individuals rarely continue to attend school. Both individuals currently sleeping in and away from the home were eligible. Dwellings were visited at least three times when necessary to interview eligible respondents. Of 2486 individuals aged 14–25 years that had never been married, 1919 were successfully interviewed (77.2%; 916 men, 1003 women). Individuals were not included in the final sample because of inability to interview after repeated household visits (n = 311), refusal (n = 73), missing data (n = 61) and other reasons (n = 122).
After a witnessed verbal consent procedure, data were collected through face-to-face structured interviews conducted in the local language (Sepedi). Interviews were conducted in a safe location chosen by the respondent and stressed confidentiality and the importance of honest reporting.23 Questionnaires investigated education, employment, HIV awareness and sexual behaviour, including details of up to three sexual partners during the previous year. A participatory wealth-ranking exercise identified households considered “very poor”.24
After a second witnessed verbal consent procedure, oral fluid samples were collected using the OraSure collection device (UCB Group, Belgium) and analysed using the Vironostika HIV Uni-Form II assay (bioMerieux, France). Data from one interviewer raised quality concerns and were excluded (n = 125, 7.6%). In addition, some samples (n = 598, 36.4%) were stored for longer than recommended by the manufacturer before analysis. Sensitivity analysis suggested little impact of this on the estimate of effect although confidence intervals were wider as a result of the smaller sample size; these samples were included. HIV test results were thus available for 1518 individuals (709 men and 809 women, 61.1% of those eligible). The major additional reasons for no HIV test result being available were refusal to provide an oral fluid sample (n = 235) or other reasons (n = 41).
Statistical analysis
Statistical analysis was conducted using Stata version 9 (Stata Corp., College Station, Texas, USA). Analyses were stratified by sex because the causal pathway between educational attainment and HIV risk may differ. A series of logistic regression analyses were undertaken to investigate the association between student status and a set of outcome variables (sexual behaviours associated with high HIV risk and HIV serostatus). Outcome variables denoting high HIV risk were developed in line with preceding literature that has identified characteristics associated with the risk of HIV infection including psychosocial attributes, power dynamics within relationships and levels and characteristics of sexual activity.25 Outcome variables were coded binary, with characteristics theoretically associated with an increased risk of HIV infection coded ‘1’. When data were naturally continuous, cut-offs were applied (see details below). Outcome variables included: an indicator of lack of knowledge about HIV based on two questions (Do you think that a healthy-looking person can be infected with HIV, the virus that causes AIDS?; Can a pregnant woman infected with HIV transmit the virus to her unborn child?); lack of communication in the household about sex/sexuality; never having had an HIV test; ever having had sex; a high total lifetime number of sexual partners (more than three for men, more than two for women, reflecting the greater number of men reporting multiple partners); and having had more than one sexual partner during the past year. Among those previously sexually active, high-risk characteristics were first sexual encounter not being wanted and remaining sexually active during the past year. Childbirth was an outcome variable considered a proxy for unprotected sex among women. High-risk characteristics of sexual partnerships were those in which: sex had occurred more frequently (more than five times in past year); the sexual partner was older for women (male partner more than three years older) or of similar age for men (less than three years younger); only the male partner was perceived to be providing resources in the relationship; and condoms had not been used during the past year or at last sex. The final outcome variable was prevalent HIV infection.
Logistic regression was used to estimate the magnitude of association between attendance at school or college (“students”) and the high HIV risk outcome variables. “Non-students” were grouped together as the comparison group for the analysis, including individuals who were unemployed, self-employed or employed. This approach was taken because the study sought to compare the experience of students with their peers not attending school. Furthermore, full-time employment was rare so statistical power to detect differences specifically among this group was low. Robust standard errors were computed to take account of intrahousehold clustering.26 Adjustment was made for explanatory variables considered a priori to be potential confounders. These variables included age (included in model 1), and village of residence, number of co-resident young people, residence in village of birth and parental status, as well as household wealth and temporary migrancy (all included in model 2). Adjustment was not made for factors on the causal pathway.27 Childbirth may lead young women to leave school, and thus act as a confounder. It might, however, also be conceptualised as on the causal pathway between school attendance and HIV risk because it is indicative of high-risk sexual behaviour. Consequently, among women effect estimates were additionally calculated after adjustment for previously having had a child (model 3). Likelihood ratio tests comparing models without the use of robust standard errors were used to explore effect modification by age group (14–19 and 20–25 years).
The trial design was approved by ethical review committees at the University of the Witwatersrand (South Africa) and the London School of Hygiene and Tropical Medicine (UK).
RESULTS
More eligible women than men were successfully interviewed (80.8% versus 73.6%; p<0.01). Among both sexes, those interviewed were significantly more likely to be aged 14–19 years (62.4% of those interviewed versus 40.9% of those not interviewed), less likely to be sleeping away from home (9.0% versus 46.0%), more likely to be attending school (65.2% versus 51.7%), less likely to have completed secondary school (11.1% versus 21.3%), and, among those not attending school, were less likely to be in regular employment (11.1% versus 21.3%) than those who were not included in the final sample (p<0.01 in all cases). The sociodemographic profile of individuals succesfully interviewed is shown in table 1. Comparing individuals who had an HIV serostatus result available with those who only completed the interview, those individuals were less likely to be sleeping away from home among both sexes (7.9% versus 13.0%), and, among men only, were more likely to be aged 14–19 years (66.3% versus 51.7%) or students (72.5% versus 55.1%), and were less likely to have completed secondary school (8.6% versus 14.0%) or previously had sex (61.2% versus 69.6%; p<0.05 in all cases).
School attendance
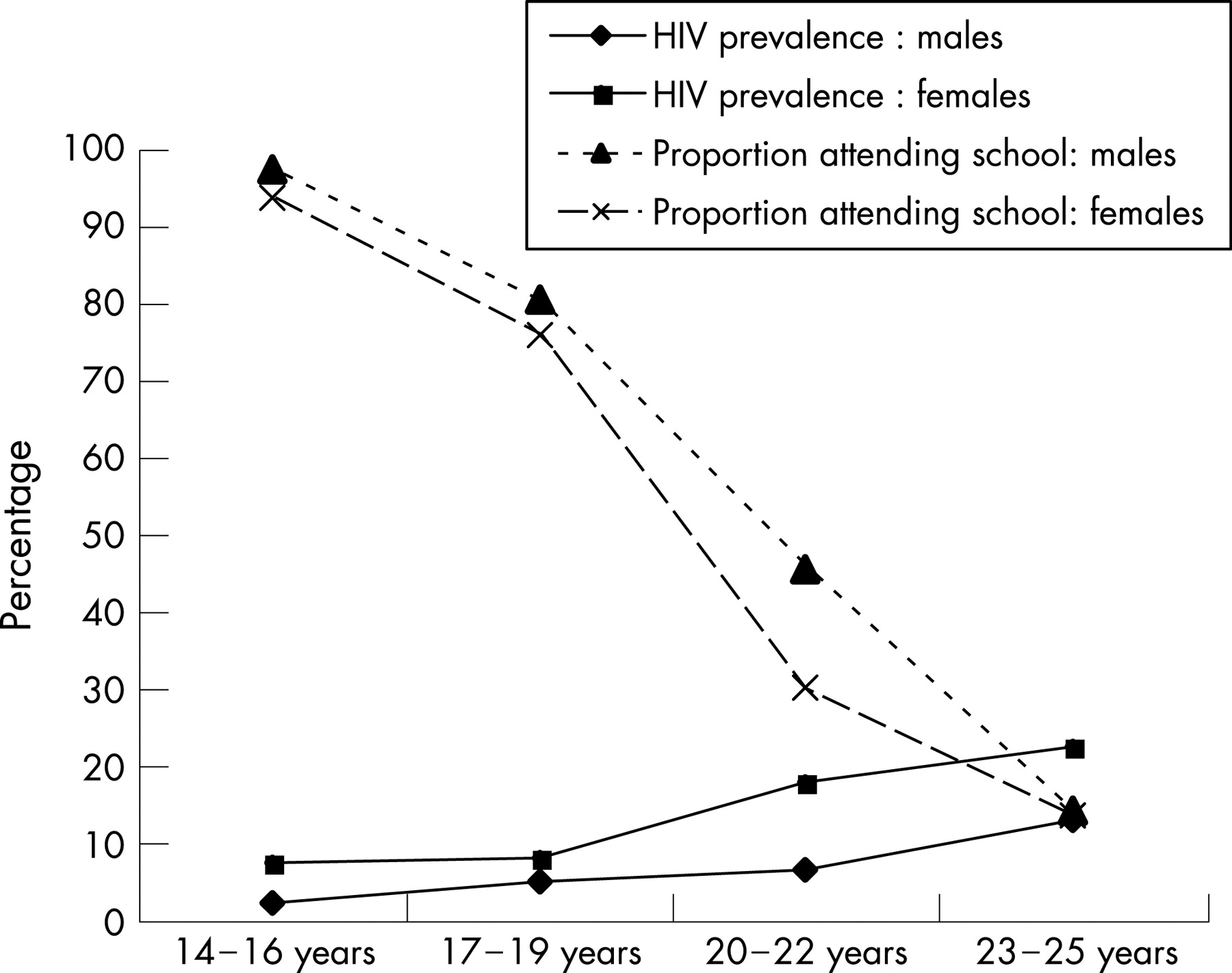
Among the men, 628 out of 916 (68.6%) of those interviewed were students. There was an approximately linear decrease across the full age range in the proportion of individuals who were students (fig 1). Overall, fewer women than men were students (623/1003, 62.1%), particularly among those aged 20–22 years (fig 1). Female, but not male, school attendance varied significantly by village (p = 0.001). Among men, individuals from “very poor” households were less likely to be students, although this was not significant (65.1% versus 70.0%, p = 0.14). Among the women, however, this relationship was significant (54.1% versus 65.5%, p<0.01).

{kind=link}
The remaining 288 men and 380 women were not students. These individuals were most often unemployed and looking for a job (n = 178, 61.8% among men; n = 306, 80.5% among women). Some had irregular work over the past year (35 men, 23 women), were self-employed (13 men, 15 women) or were unwilling or unable to work (13 men, 11 women). Some 49 men (17.0%) and 25 women (6.6%) had regular contract or salaried employment during the past year. The proportion of those not attending school who were employed increased significantly with age among women (test for trend p = 0.02) and non-significantly among men (p = 0.20).
Just three men and five women reported that they had not attended school at all. Most individuals had attended secondary school. The proportion who had completed secondary school, however, including those who had also attended university or vocational training college, was low (90 men, 9.8%; 94 women, 9.4%), but was highest among the oldest age group.
HIV risk characteristics
Among both sexes, lack of knowledge about HIV was widespread (57.8% men, 55.9% women). Intrahousehold communication on sex and sexuality in the past year was relatively common (40.1% men, 48.1% women). Few individuals had had an HIV test (4.1% men, 6.1% women). More young men reported a high number of partners than young women (median 2, interquartile range 0–4 for men; median 2, interquartile range 0–3 for women), although there was little difference between men and women in the numbers reporting ever having had sex (63.1% men, 70.4% women). A total of 515 men and 627 women reported at least one sexual partner in the past year, and in total men reported 774 sexual relationships (of which details were available for 750) and women reported 702 relationships (details on 700). Condom use at last sex was reported for 37.0% (men) and 29.4% (women) of sexual partnerships. Sexual partnerships reported by young women usually involved men who were older than them (median 4 years older, interquartile range 2–7 years) and who they perceived to be providing them with resources (71.7%), whereas young men reported partnerships with women who were of similar age or younger (median 2 years younger, interquartile range 1–4 years). HIV prevalence was 3.4% among men and 9.8% among women, increasing over the age range (fig 1).
School attendance and HIV-risk characteristics
Men
After adjustment for age and other confounding factors, HIV knowledge, communication and testing were more likely to be reported by students than non-students, although none of these associations was statistically significant (table 2). Having had more than three lifetime sexual partners and having had sex with more than one partner in the past year were both significantly less commonly reported by students. Ever having had sexual intercourse, unwanted sex at debut and secondary abstinence among those previously sexually active were not significantly associated with school attendance.
Partnerships characterised by male-to-female resource exchange were less commonly reported by students (table 2). There was some evidence that partnerships in which sexual intercourse had occurred more than five times in the past year were less commonly reported by students, although this did not reach statistical significance. Students were significantly less likely to be HIV positive than non-students. There was little evidence of age interaction for any outcomes.
What is already known on this subject
HIV has spread most rapidly in countries with low average education. Within sub-Saharan Africa, however, higher educational attainment has previously been associated with a greater risk of infection. This may be changing as the epidemic progresses, but mechanisms remain unclear.
Women
Among women, HIV knowledge and testing were not associated with school/college attendance, although lack of household communication about sex/sexuality was more common among female students with borderline significance before adjustment for childbirth (table 3). Without adjustment for childbirth, students were significantly less likely ever to have had sex. This effect was, however, almost entirely removed after adjustment for ever having had a child. Students were less likely to report more than two partners during their lifetime than non-students, even after adjustment for previous childbirth. Students were also less likely to have had a child. This effect was particularly strong among the younger group but was also significant in the older group (likelihood ratio test p<0.01).
Sexual partnerships reported by students were significantly less likely to be characterised by a high frequency of sexual activity than non-students (table 3). Students were significantly less likely to report partnerships characterised by the man being more than three years older than the woman or to report never having used a condom during the past year. Condom use at last sex was more commonly reported by students. After adjustment for age there was little evidence of an association between school attendance and prevalent HIV infection among women. There was little evidence of age interaction for any characteristics other than previous childbirth.
What this study adds
This study suggests that among young people in rural South Africa, attendance at school may be associated with lower vulnerability to HIV. The data suggest that this may be through an impact on the size and characteristics of the sexual network of students compared with those who leave school early.
DISCUSSION
In this study, male students were less likely to be HIV positive than their peers not attending school. Among young women there was less evidence of an association. For both sexes, attending school was associated with having fewer sexual partners. In addition, female students in relationships had sex less often, had partners closer in age to themselves and used condoms more often than non-students.
Policy implications
In the long term, strategies to reduce school drop-out, increase attendance and ensure universal access to both primary and secondary education will contribute to the effective prevention of HIV infection.
Interventions that might increase secondary school attendance such as microfinance, school feeding programmes or direct cash incentives should be evaluated for their potential to influence HIV risk.
The development of HIV prevention programmes that effectively meet the needs of out-of-school youth remains an urgent priority.
The strengths of the study included the use of best-practice techniques to collect sexual behaviour data and ensure a high response rate. Focusing on young people also has methodological advantages. HIV infection is likely to have occurred recently, allowing the association with current school attendance to be assessed with greater confidence. Biases associated with AIDS-related mortality will be limited. Nevertheless, the study had limitations. The cross-sectional data meant it was not possible to determine the temporality of recorded events. This was particularly an issue among young women, for whom childbearing is an important reason for leaving school early.28 Most associations between school attendance and risk characteristics among young women were, however, seen after adjustment for childbirth, which might also have given “overadjusted” results because this factor may be on the causal pathway. Further limitations were the remaining potential for misreported outcomes and the use of multiple statistical tests, increasing the probability that some significant associations arose by chance.
The results suggest mechanisms by which there may be a protective effect of school attendance on HIV risk. Those in school did not seem to have greater access to HIV prevention materials. Life skills and sexual health education within schools across South Africa was poorly developed at the time of the study.29 There was little evidence that school attendance was associated with better HIV knowledge, the use of testing services or communication.
School attendance may, however, reduce HIV risk through affecting sexual network structure.30 This study reports lower numbers of partners for both young men and young women attending school. Furthermore, young women attending school were less likely to have an older male partner than those out of school, had sex less often and were more likely to use condoms. Wide age differences between partners can be a risk factor for HIV infection among young women, contributing to their higher prevalence of infection than young men,31–34 alongside biological mechanisms.35 Power inequalities between older men and younger women might also affect the frequency of sex and whether condoms are used.36 No data were available on whether sexual partners were attending school. Future research should explore this because it has important implications for targeting health promotion messages to individuals and couples within, and across, school boundaries. School attendance might affect communication within sexual networks, in turn helping to improve confidence, self-efficacy and the adoption of safer sexual behaviours. It may also increase group negotiation of positive attitudes towards protective behaviours,37 38 by putting young people in regular contact with each other in a structured environment. Behavioural self-efficacy was not measured within the current study but may also have been linked to the differences noted. School attendance may encourage the formation of other social groups with high levels of social capital and more positive future expectations that may support the adoption of protective behaviours.39 Furthermore, students may have shared reference to HIV prevention campaigns. Conversely, those who leave school may enter adult sexual networks in which negotiation processes are more fraught and older partners with more experience and power dictate the “rules” of sexual engagement. Future studies employing both qualitative and quantitative methods should examine the influence of school attendance on psychosocial attributes, the size and structure of sexual networks and characteristics of sexual behaviour that can influence HIV risk.
HIV prevalence is falling in sub-Saharan Africa among young people with high, but not low, educational attainment.10–13 Primary school fees have been abolished in efforts to extend access in countries such as Kenya, Tanzania, Malawi and Uganda, resulting in significant increases in school enrolment.40 Fees still exist in many countries, however, including South Africa, alongside barriers to attendance such as the cost of transport, uniforms and books. Secondary school attendance remains constrained in many settings, but this has the greatest potential to influence sexual network structure. Strategies to reduce school drop-out and ensure universal access to primary and secondary education should be a priority. Interventions that might increase secondary school attendance such as microfinance, school feeding programmes or direct cash incentives should be evaluated for their potential to influence HIV risk. Finally, the development of HIV prevention programmes that effectively meet the needs of out-of-school youth remains an urgent priority.
Acknowledgments
The authors would like to thank the Contract Laboratory Services at the Johannesburg Hospital, particularly Dr Wendy Stevens, Grant Napier, Anusha Makuraj and Dr Gwynn Stevens, for assisting in the processing of laboratory specimens, and also Edwin Maroga, Rico Euripidou and Joseph Mhlaba who led the data collection. They would also like to thank Professor John Gear, Professor Simon Gregson, Dr Anne Buvé and Professor Salim Vally for useful comments at various stages of the work. Finally, the authors would like to thank the two anonymous reviewers who provided comments on the paper.
REFERENCES
Footnotes
Funding: The study received financial support from AngloAmerican Chairman’s Fund Educational Trust, AngloPlatinum, Department for International Development (UK), The Ford Foundation, The Henry J. Kaiser Family Foundation, HIVOS, the South African Department of Health and Welfare, and the Swedish International Development Agency.
Competing interests: None declared.
Linked Articles
- In this issue