Article Text

Abstract
BACKGROUND The effect of hepatitis delta virus (HDV) infection on the clinical course of cirrhosis type B is poorly defined.
AIMS To investigate the impact of HDV status on morbidity and mortality in cirrhosis type B.
PATIENTS/METHODS Retrospective cohort study of 200 Western European patients with compensated cirrhosis type B followed for a median period of 6.6 years.
RESULTS At diagnosis, 20% of patients had antibodies to HDV (anti-HDV); median age was lower in anti-HDV positive cirrhotics (34 v 48 years respectively). Kaplan-Meier five year probability of hepatocellular carcinoma (HCC) was 6, 10, and 9% in anti-HDV positive/HBeAg negative, anti-HDV negative/HBeAg negative, and anti-HDV negative/HBeAg positive cirrhotics respectively; the corresponding figures for decompensation were 22, 16, and 19% and for survival they were 92, 89, and 83% respectively. Cox regression analysis identified age, albumin concentration, γ-globulin concentration, and HDV status as significant independent prognostic variables. After adjustment for clinical and serological differences at baseline, the risk (95% confidence interval) for HCC, decompensation, and mortality was increased by a factor of 3.2 (1.0 to 10), 2.2 (0.8 to 5.7), and 2.0 (0.7 to 5.7) respectively in anti-HDV positive relative to HDV negative cirrhotic patients. The adjusted estimated five year risk for HCC was 13, 4, and 2% for anti-HDV positive/HBeAg negative, anti-HDV negative/HBeAg negative, and anti-HDV negative/HBeAg positive cirrhotics respectively; the corresponding figures for decompensation were 18, 8, and 14% and for survival 90, 95, and 93% respectively.
CONCLUSIONS HDV infection increases the risk for HCC threefold and for mortality twofold in patients with cirrhosis type B.
- delta hepatitis
- prognosis
- hepatocellular carcinoma
- decompensation
- survival
Statistics from Altmetric.com
The hepatitis delta virus (HDV) is a defective pathogen which requires for infection the helper functions of hepatitis B virus (HBV).1 It is responsible for acute or chronic hepatitis. Acute delta hepatitis may occur either by simultaneous co-infection with HDV and HBV or by HDV superinfection in a person already chronically infected with HBV. Chronicity of HDV infection most commonly develops after acute delta superinfection.2
Numerous clinical studies have reported that patients with chronic HDV infection often show severe chronic hepatitis or cirrhosis on initial liver biopsy.3-5 Cross sectional studies have indicated that patients with hepatitis B surface antigen (HBsAg) positive chronic hepatitis and HDV infection have more severe liver disease than those with HBV infection alone.6 Moreover longitudinal studies have reported that HDV infection in patients with chronic hepatitis B is associated with a more rapid progression to cirrhosis than in HBsAg carriers with chronic hepatitis and no evidence of HDV infection.7 Overall, these data indicate that HDV infection tends to influence unfavourably the clinical outcome of chronic hepatitis B. However at present, there are insufficient data to clarify whether HDV alters the clinical course of HBV related compensated cirrhosis and increases the risk of hepatocellular carcinoma (HCC). The aim of this study was to investigate the impact of HDV infection on the prognosis of compensated cirrhosis type B in a cohort of 200 Western European patients followed untreated for a median period of 6.6 years. Morbidity, namely incidence of complications of cirrhosis and incidence of HCC, and mortality were compared in anti-HDV positive and negative patients.
Materials and methods
PATIENTS
The study is based on analysis of data derived from a longitudinal study of compensated cirrhosis due to HBV, which involved nine tertiary referral university hospitals in Europe participating in the Concerted Action on Viral Hepatitis named Eurohep. The details of the overall design of this study have been described previously.8Briefly, all patients meeting the following criteria were evaluated in the present investigation: (a) HBsAg positivity; (b) histological diagnosis of cirrhosis according to international criteria9; (c) no history or clinical evidence of complications of cirrhosis—that is, ascites, variceal bleeding, encephalopathy, or jaundice; (d) no evidence of HCC at diagnosis; (e) information on serum hepatitis B e antigen (HBeAg) and antibody to HDV (anti-HDV) at presentation; (f) follow up at the enrolling centre for a minimum period of six months; (g) no antiviral or steroid treatment during follow up. These entry criteria resulted in a cohort of Child-Pugh class A patients. Patients with autoimmune or metabolic liver disease were excluded by history, serological variables, and histology.
The starting time for morbidity and survival analysis was the time of diagnosis of HBsAg positive compensated cirrhosis. The follow up was calculated from the date of entry until death, liver transplantation, or the last observation. All patients were evaluated at least once a year or at more frequent intervals as indicated by their clinical conditions. Death was classified as being caused by liver failure if (a) progressive impairment of liver function occurred or (b) it occurred within 40 days of variceal bleeding, regardless of the severity, or as being caused by HCC. The diagnosis of HCC was based on either liver biopsy or α fetoprotein levels of more than 400 μg/l plus compatible liver ultrasonography. Decompensation was defined as at least one episode of ascites, jaundice, hepatic encephalopathy, or gastrointestinal bleeding of variceal origin.
SEROLOGICAL TESTING
Virological data were obtained by review of the patients' charts or were retrospectively obtained using stored serum samples. HDV infection was diagnosed on the basis of anti-HDV in the serum and hepatitis delta antigen in the liver. HBsAg, HBeAg, antibody to HBeAg (anti-HBe), anti-HDV, and antibody to HIV (anti-HIV) were tested for by commercially available radioimmunoassays or enzyme linked immunosorbent assays (ELISAs). Serum HBV DNA was measured by a spot hybridisation or by a solution hybridisation assay. Serum antibody to hepatitis C virus was tested for by a second generation ELISA. Hepatitis delta antigen in the liver was tested for by direct immunofluorescence using fluorescein isothiocyanate conjugated anti-HDV serum on frozen unfixed liver sections or by immunoperoxidase staining using commercially available polyclonal anti-HDV on paraffin wax embedded material.
STATISTICAL ANALYSIS
Statistical analyses were performed by the χ2test and the analysis of variance test to compare differences between proportions and medians respectively. The cumulative probability of HCC appearance, decompensation occurrence, and survival were calculated by the Kaplan-Meier method.10 Because a minority of cirrhotics were anti-HDV/HBeAg positive, this analysis is based on data condensed into three groups of cirrhotics: anti-HDV positive/HBeAg negative, anti-HDV negative/HBeAg negative, and anti-HDV negative/HBeAg positive. Patients who died from conditions not related to liver disease, those undergoing liver transplantation, and patients who were lost to follow up were censored at the time of death, at the time of transplantation, or at the time of drop out in this analysis.10 Curves were compared using the log rank test.11 Prognostic factors for HCC, decompensation, and survival were identified using Cox regression analysis,12 13 both univariate and multivariate, with backward elimination of insignificant variables. Potential prognostic factors assessed for morbidity and mortality included the following clinical, biochemical, and virological variables measured at enrolment: sex, age, log10 (bilirubin concentration), levels of albumin, γ-globulins, and platelets, HBeAg and anti-HDV status. Sex (male = 1, female = 0), anti-HDV (positive = 1, negative = 0), and HBeAg (positive =1, negative =0) were introduced as dichotomous variables. To analyse the influence of HDV status on clinical end points, the Cox model included at all stages, whether significant or not, the indicator term of HDV status (anti-HDV positive = 1, negative = 0), and in the model obtained the p value for the HDV term shows directly the significance of the HDV status adjusted for the influence of all the other prognostic variables included. Because the analysis requires that all patients are represented by a complete set of variables and, in order not to reduce the number of patients, missing data were replaced by neutral estimates.14 The adjusted relative risks (HDV positive/HDV negative) (with 95% confidence limits) for HCC, decompensation, and survival were estimated from the regression coefficient (and SE) for the HDV status in models including variables, the influence of which was to be adjusted for.14 The adjusted curves for the probability of HCC or decompensation occurrence and for survival were estimated from the regression models as previously described.14 The statistical software used was BMDP. In all analyses, a p value less than 0.05 was considered statistically significant.
Results
BASELINE CHARACTERISTICS ACCORDING TO ANTI-HDV/HBeAG STATUS
We evaluated 200 white patients with HBsAg positive compensated cirrhosis who fulfilled the inclusion criteria. This series represents all untreated white patients enrolled in a previous study8evaluating survival of compensated cirrhosis type B, except 17 of oriental or black origin, 36 with antibody to hepatitis C virus and/or anti-HIV positivity, and 113 who had received antiviral (n = 87) or steroid (n = 26) treatment.
At enrolment, 39 (20%) patients were anti-HDV positive, including two HBeAg positive cases, and 161 patients were anti-HDV negative, including 45 HBeAg positive cirrhotics.
Table 1 gives a comparison of the main clinical and serological patient features according to HDV and HBeAg status at presentation. Median age was lower in the anti-HDV positive patients, while no significant difference was noted in the gender. Assessment of the probable source of infection showed a higher proportion of household contacts and drug addicts among patients with HDV related cirrhosis. Anti-HDV positive patients had higher γ-globulin concentrations and slightly lower platelet levels. When just tested, a smaller proportion of anti-HDV positive/HBeAg negative cirrhotics had evidence of HBV DNA detectable in the serum than did anti-HDV negative/HBeAg negative patients (7%v 30% respectively).
Baseline features of 200 patients with cirrhosis type B (Child A) according to hepatitis delta virus (HDV) and hepatitis B e antigen (HBeAg) status
CLINICAL OUTCOME ACCORDING TO ANTI-HDV/HBeAG STATUS
The 200 patients were followed for a median period of 80 (range 6–198) months. The duration of follow up was comparable for the anti-HDV positive and negative patients (p = 0.2), and so were the drop out rates (p = 0.2) (table 2).
Clinical outcome of 200 patients with cirrhosis type B (Child A) according to hepatitis delta virus (HDV) and hepatitis B e antigen (HBeAg) status
Development of HCC
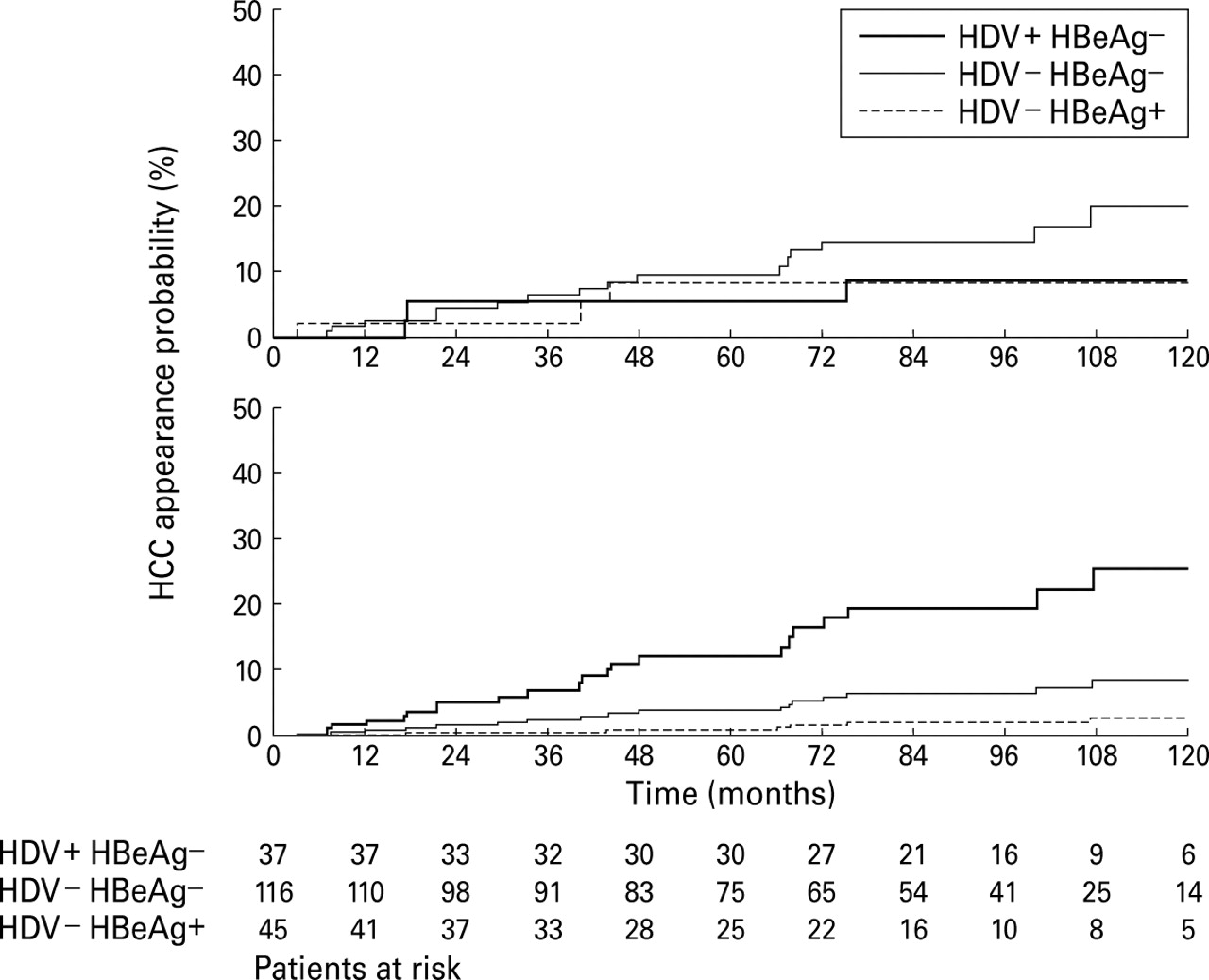
As shown in table 2, during follow up, HCC developed in five (13%) anti-HDV positive/HBeAg negative, 19 (16%) anti-HDV negative/HBeAg negative, and three (7%) anti-HDV negative/HBeAg positive patients with cirrhosis type B; the median age of patients at the time of diagnosis of HCC was 54 (range 51–63), 62 (range 40–76), and 64 (52–78) years for the three groups of cirrhotics respectively. The median interval between the time of entry into the study and the diagnosis of HCC was 75 (range 17–128) months for anti-HDV positive/HBeAg negative patients, 48 (range 7–181) months for anti-HDV negative/HBeAg negative patients, and 40 (range 7–44) months for anti-HDV negative/HBeAg positive cirrhotics. The unadjusted five year cumulative incidence of HCC was 6, 10, and 9% for anti-HDV positive/HBeAg negative, anti-HDV negative/HBeAg negative, and anti-HDV negative/HBeAg positive cirrhotics respectively (fig 1, top).
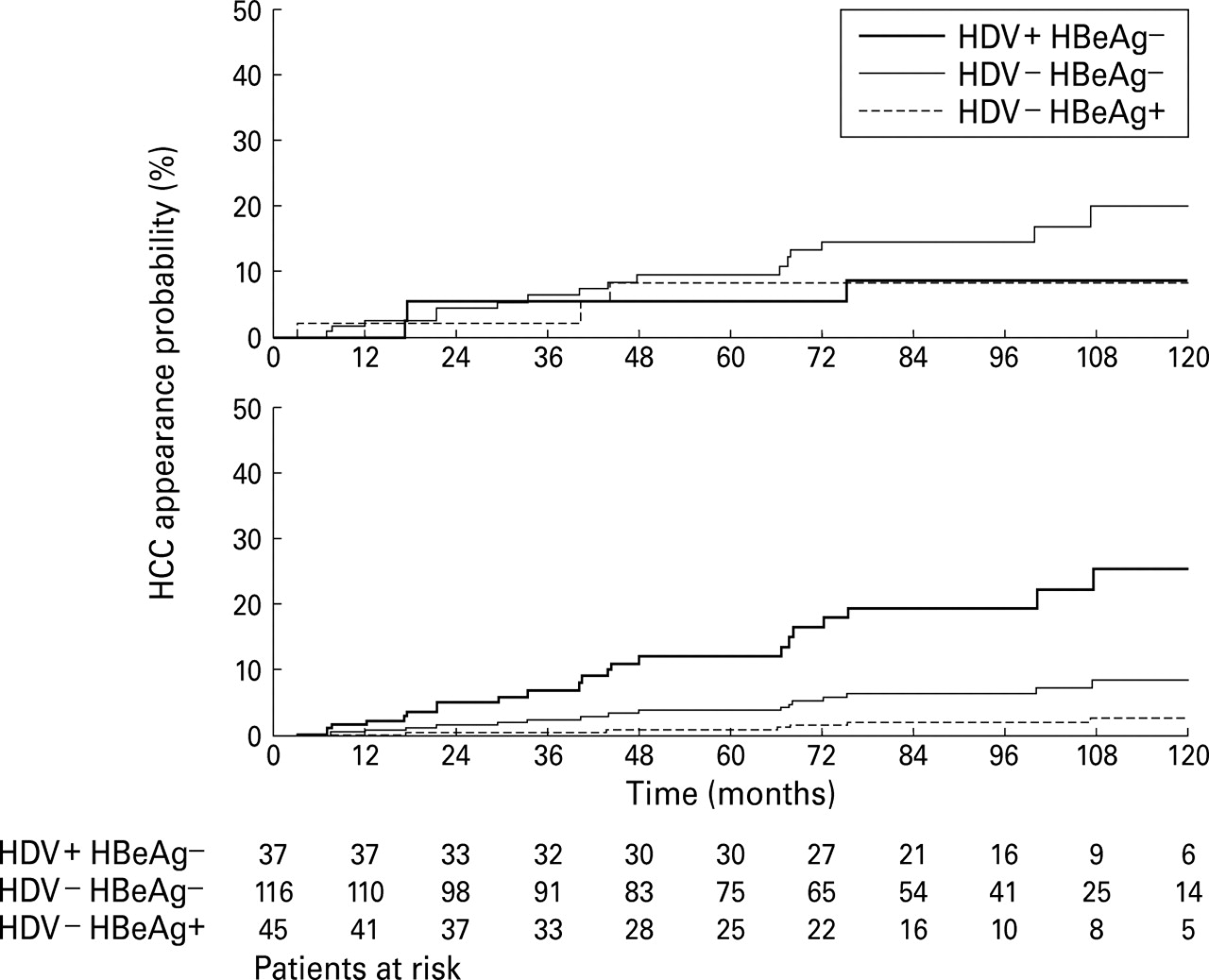
Cumulative probability of hepatocellular carcinoma (HCC) appearance in patients with compensated cirrhosis type B (Child A) in relation to anti-hepatitis delta virus (HDV) and hepatitis B e antigen (HBeAg) status. The five year appearance rate was 6, 10, and 9% for anti-HDV positive/HBeAg negative (thick line), anti-HDV negative/HBeAg negative (thin line), and anti-HDV negative/HBeAg positive (dashed line) patients respectively (p = 0.33, log rank test) (top). The estimated five year probability adjusted for all potential prognostic variables by Cox model was 13, 4, and 2% for anti-HDV positive/HBeAg negative, anti-HDV negative/HBeAg negative, and anti-HDV negative/HBeAg positive patients respectively (bottom).
Factors correlating with HCC
Among the clinical and biochemical features studied by univariate analysis, older age, lower platelet levels, and higher bilirubin concentration were significantly associated with a higher risk of HCC (table 3).
Univariate Cox analysis for hepatocellular carcinoma (HCC) occurrence, decompensation appearance, and survival in 200 patients with cirrhosis type B (Child A)
In multiple Cox regression analysis, an older age (p<0.0001) and anti-HDV positivity (p = 0.05) were independently and significantly associated with a higher risk of HCC (table 4).
Cox regression models including only significant variables (and HDV status) for prediction of hepatocellular carcinoma (HCC) occurrence, decompensation appearance, and survival
As shown in table 5, HDV superinfection significantly increased the risk for HCC by a factor of 3.2 (fully adjusted relative risk).
Effect of hepatitis delta virus (HDV) status on hepatocellular carcinoma (HCC) occurrence, decompensation appearance, and survival
The estimated fully adjusted five year risk of HCC occurrence (using median values of the variables at baseline in the Cox model) was 13, 4, and 2% for anti-HDV positive/HBeAg negative, anti-HDV negative/HBeAg negative, and anti-HDV negative/HBeAg positive cirrhotics respectively (fig 1, bottom).
Development of decompensation
Of the 173 patients who remained tumour free, 12 (37%) anti-HDV positive/HBeAg negative, 20 (21%) anti-HDV negative/HBeAg negative, and 11 (26%) anti-HDV negative/HBeAg positive cirrhotics developed at least one episode of decompensation (table 2). The unadjusted five year probability of decompensation was 22, 16, and 19% in the three subgroups of cirrhotics respectively (fig 2, top).

Cumulative probability of developing decompensation in patients with compensated cirrhosis type B (Child A) in relation to anti-hepatitis delta virus (HDV) and hepatitis B e antigen (HBeAg) status. The analysis included 171 patients who remained tumour free. The five year probability of decompensation was 22, 16, and 19% for anti-HDV positive/HBeAg negative (thick line), anti-HDV negative/HBeAg negative (thin line), and anti-HDV negative/HBeAg positive (dashed line) patients (p = 0.38, log rank test) (top). The estimated five year probability adjusted for all potential prognostic variables by Cox model was 18, 8, and 14% for anti-HDV positive/HBeAg negative, anti-HDV negative/HBeAg negative, and anti-HDV negative/HBeAg positive patients respectively (bottom).
Factors correlating with decompensation
By univariate analysis the following variables were significantly associated with a higher risk of decompensation: older age, lower albumin concentration, higher γ-globulin concentration, and lower platelet levels (table 3).
In multivariate analysis, lower albumin concentration (p = 0.0001) and higher γ-globulin concentration (p<0.0001) independently showed significant association with a higher risk of decompensation (table 4).
HDV superinfection increased the risk for decompensation, although not significantly, by a factor of 2.2 (fully adjusted relative risk) (table5).
The estimated fully adjusted five year probability of decompensation (using median values of the variables at baseline in the Cox model) was 18, 8, and 14% for anti-HDV positive/HBeAg negative, anti-HDV negative/HBeAg negative, and anti-HDV negative/HBeAg positive patients respectively (fig 2, bottom).
Survival
During follow up, liver related death occurred in six (16%) anti-HDV positive/HBeAg negative patients, 23 (20%) anti-HDV negative/HBeAg negative, and nine (20%) anti-HDV negative/HBeAg positive cirrhotics (table 2). Decompensated cirrhosis necessitating liver transplantation occurred in four, two, and two other patients in the three subgroups of cirrhotics respectively. The unadjusted five year probability of survival was 92, 89, and 83 in anti-HDV positive/HBeAg negative, anti-HDV-negative/HBeAg negative, and anti-HDV negative/HBeAg positive cirrhotics respectively (fig 3, top).

{kind=link}
{kind=link}
{kind=link}
Cumulative survival probability in patients with compensated cirrhosis type B (Child A) in relation to anti-hepatitis delta virus (HDV) and hepatitis B e antigen (HBeAg) status. The five year survival probability was 92, 89, and 83% for anti-HDV positive/HBeAg negative (thick line), anti-HDV negative/HBeAg negative (thin line), and anti-HDV negative/HBeAg positive (dashed line) patients (p = 0.61, log rank test) (top). The estimated five year survival probability adjusted for all potential prognostic variables by Cox model was 90, 95, and 93% for anti-HDV positive/HBeAg negative, anti-HDV negative/HBeAg negative, and anti-HDV negative/HBeAg positive patients respectively (bottom).
Factors correlating with survival
By univariate analysis, older age, lower albumin concentration, and higher γ-globulin concentration were significantly associated with a decreased survival (table 3).
In multivariate analysis, older age (p<0.0001), lower albumin concentration (p = 0.0027), and higher γ-globulin concentration (p = 0.026) independently showed association with a decreased survival (table 4).
As shown in table 5, HDV superinfection increased mortality, although not significantly, by a factor of 2 (fully adjusted relative risk).
The estimated fully adjusted five year survival (using median values of the variables at baseline in the Cox model) was 90, 95, and 93% for anti-HDV positive/HBeAg negative, anti-HDV negative/HBeAg negative, and anti-HDV negative/HBeAg positive cirrhotics respectively (fig 3, bottom).
Discussion
The main findings of our study concern the clinical expression of HDV infection in Western European patients with compensated cirrhosis (Child A) on their first presentation at tertiary referral centres and the impact of HDV infection on morbidity and mortality in cirrhosis type B.
The 20% prevalence of anti-HDV in 200 HBsAg positive cirrhotics closely parallels the data from previous European studies of chronic HBsAg carriers.15 16 Our results indicate that HDV infection modifies to a certain extent the clinical and serological presentation of HBsAg positive cirrhosis. In fact the presence of anti-HDV in serum identified a subgroup of cirrhotic patients who were younger and had higher serum levels of γ-globulins and slightly lower platelet levels compared with anti-HDV negative cirrhotics. In addition, characteristic features of these anti-HDV positive patients were the high prevalence of anti-HBe in serum and the low rate of active HBV replication, as indicated by the detection of serum HBeAg and/or HBV DNA in a small proportion of about 10% of the patients tested. These results are consistent with the fact that HDV suppresses the synthesis of HBV genome and serum HBV DNA often remains undetectable by traditional methods both at the acute and chronic stage of HDV superinfection.17 18 It is interesting to note that these findings are in agreement with previous observations obtained in prospective studies of patients with HBsAg positive chronic hepatitis that HDV infection affects mainly young anti-HBe positive patients and is associated with a more rapid progression to cirrhosis.7 19 It has been reported that, in about 15% of cases of chronic delta hepatitis, the disease is rapidly progressive, with cirrhosis developing within two years of onset,19 and our data indicate that patients with superimposed delta infection may progress to cirrhosis about 15 years earlier than those with HBV infection (median age at diagnosis of cirrhosis 34 v 48 years in anti-HDV positive and negative patients respectively).
The analysis of potential risk factors for HDV infection in our study population confirms that parenteral drug addicts are at highest risk and play a major role in the spread of the delta agent in the western world. HDV infection was also related to household contact with an HBsAg positive carrier, which is in agreement with previous observations that intrafamily contact may favour the spread of infection, particularly in areas of southern Europe where the delta agent is endemic.15 16
Few data are available on the clinical course of compensated cirrhosis associated with delta infection. Previous longitudinal studies on the outcome of delta cirrhosis have only included a small number of cirrhotic patients and/or have not distinguished between compensated and decompensated cirrhosis.3 20 In addition, at present the question is whether HDV alters the clinical course of HBV related compensated cirrhosis and increases the risk of HCC.
The impact of HDV infection on the clinical course of compensated cirrhosis type B (Child A) has been analysed in our cohort of 200 untreated patients followed for a median period of 6.6 years; morbidity and mortality were evaluated in delta positive/HBeAg negative cirrhotics and compared with two groups of delta negative patients, namely 116 HBeAg negative and 45 HBeAg positive. The unadjusted Kaplan-Meier analysis of the cumulative incidence of HCC and decompensation and of survival probability showed no significant difference between the three subgroups of patients (figs 1, 2, and 3top). In addition, by univariate prognostic Cox analysis, HDV status is not a significant predictor of clinical outcome and has a negative B regression coefficient for HCC and survival (table 5)—that is, it tends to be associated with a lower risk for liver tumour and a longer survival—but these data are partly explained by the younger age of the anti-HDV positive patients. As age is a very powerful prognostic variable for HCC and survival (table 4), its inclusion has a pronounced effect in the multivariate analysis, where HDV status has a positive B regression coefficient—that is, higher risk for HCC occurrence and worse survival if anti-HDV is positive—and becomes significant for liver tumour occurrence (table 5). These data indicate that univariate analysis can be misleading and that the HDV effect needs to be adjusted in a multivariate analysis. In addition to age, albumin and γ-globulin levels were found to be independent predictors of clinical outcome in the multivariate analysis. In the current study, albumin is a strong prognostic variable for decompensation and survival. Only a minority (17%) of our patients with Child A cirrhosis had serum levels of albumin lower than 35 g/l, further indicating that albumin is a sensitive marker of hepatic insufficiency in cirrhosis. Hypergammaglobulinaemia in cirrhosis is considered to be a consequence of chronic exposure to exogenous antigen absorbed mainly from the gut as the result of an impaired hepatic reticuloendothelial systemic phagocytic activity related to intrahepatic shunting of blood.21 22 In addition, recent data indicate that high levels of endotoxin antibodies contribute to hypergammaglobulinaemia in cirrhotic patients, probably as a result of chronic endotoxin exposure.23 Therefore serum γ-globulin levels have a prognostic value because they reflect the degree of alteration of the hepatic circulation in the cirrhotic liver.
The prognosis in cirrhosis varies widely according to patient characteristics. As shown in table 5, it appears that for all the three end points evaluated (HCC, decompensation, and survival) the adjusted HDV effect tends to be harmful (positive B regression coefficient) and that the estimated risk for HCC or decompensation occurrence and for shorter survival increases by a factor of 2 or more, although this is only significant for HCC. Accordingly, after adjustment for clinical and serological differences at baseline, the estimated five year probability of HCC, decompensation occurrence was highest and of survival was lowest in anti-HDV positive patients (figs 1, 2, and 3, bottom).
The probability of survival (about 90% at five years) observed in our delta cirrhotics was higher than that (71%) previously reported at five years in a Dutch study.20 This finding may be explained by differences in patient characteristics at entry, as the study from The Netherlands also included patients at an advanced stage of cirrhosis (Child B and C). In our study we have analysed only patients with biopsy proven compensated cirrhosis, but no data are available about how many potential cirrhotics were excluded because they did not have a liver biopsy or because they already had clinical evidence of advanced cirrhosis, and it is possible that there may have been a selection bias to exclude delta positive or delta negative patients with more severe liver disease
In conclusion, the most important characteristic of chronic delta hepatitis appears to be its propensity to progress rapidly to cirrhosis, and our longitudinal study conducted in patients with compensated cirrhosis type B indicates that concomitant HDV infection is associated with a threefold increased risk for HCC and with a twofold increased risk of mortality, confirming the poor prognosis in this subgroup of patients.
Acknowledgments
In addition to the authors, the members of the European Concerted Action on Viral Hepatitis (Eurohep) include the following: Piero Almasio, Cattedra di Clinica Medica R, University of Palermo, Palermo, Italy; Miguel Carneiro de Moura, Servico de Medicina II, Medical School of Lisbon, Lisbon, Portugal; Francoise Degos, Fèdèration d'Hèpatogastroentèrologie et INSERM U24, Hopital Beaujon, Paris, France; Stephanos Hadziyannis, Academic Department of Medicine, Hippokration General Hospital, Athens, Greece; Kim Krogsgaard, Institute of Preventive Medicine, Kommunehospitalet, Copenhagen, Denmark; Carlos Quero, Hepatogastroenterology, Erasmus University Hospital Dijkzigt, Rotterdam, The Netherlands; Josè Sanchez-Tapias, Liver Unit, Hospital Clinic, University of Barcelona, Barcelona, Spain; Antonio Solinas, Istituto di Patologia Speciale Medica, University of Sassari, Sassari, Italy.
References
Footnotes
- Abbreviations used in this paper:
- HDV
- hepatitis delta virus
- HBV
- hepatitis B virus
- HBsAg
- hepatitis B surface antigen
- HBeAg
- hepatitis B e antigen
- ELISA
- enzyme linked immunosorbent assay
- HCC
- hepatocellular carcinoma