Article Text

Abstract
Background: It is well documented that highly active antiretroviral therapy (HAART) restores systemic immunity to human immunodeficiency virus (HIV) but the effect of this treatment on the mucosal immune system is less clear.
Aims: Because future preventive or therapeutic vaccines against HIV may be administered by the mucosal route, we wished to evaluate the effect of HAART on the activation level and homeostasis of the intestinal B cell system.
Patients and methods: Duodenal biopsy specimens were collected consecutively from infection prone HIV positive adults (n = 31), mostly with advanced AIDS. In situ two colour immunofluorescence staining was performed to quantify mucosal immunoglobulin (Ig) class and subclass producing immunocytes (plasmablasts and plasma cells).
Results: HIV positive patients had, on average, duodenal proportions of IgA (74.6%), IgM (19.5%), and IgG (3.4%) immunocytes similar to median values recorded in 11 HIV seronegative healthy controls but the total immunocyte number per mucosal section length unit (500 μm) was significantly increased in patients (median 175 v 120 cells/unit; p<0.008), mainly comprised of IgA (p<0.02) and IgG1 (median 81.8% of total IgG; p<0.02) isotypes. Patients receiving a successful HAART regimen tended to normalise their IgG1 proportion and showed significantly lower total duodenal IgA immunocyte number than those receiving no or insufficient antiretroviral treatment (p<0.005).
Conclusion: Our study demonstrated that advanced AIDS patients hyperactivate their intestinal B cell system. HAART could significantly reverse this perturbation, suggesting restored ability of the mucosal immune system to control intestinal infections.
- duodenal mucosa
- Ig producing cells
- mucosal immune response
- AIDS
- therapy response
- highly active antiretroviral therapy
- AIDS, acquired immunodeficiency syndrome
- ARC, AIDS related complex
- β2-M, β2 microglobulin
- CDC, Centers for Disease Control and Prevention
- HAART, highly active antiretroviral therapy
- HIV, human immunodeficiency virus
- IELs, intraepithelial lymphocytes
- Ig, immunoglobulin
- IVDA, intravenous drug abusers
- mAbs, monoclonal antibodies
- NA, nucleoside analogues
- SIV, simian immunodeficiency virus
- TCR, T cell receptor
Statistics from Altmetric.com
- duodenal mucosa
- Ig producing cells
- mucosal immune response
- AIDS
- therapy response
- highly active antiretroviral therapy
- AIDS, acquired immunodeficiency syndrome
- ARC, AIDS related complex
- β2-M, β2 microglobulin
- CDC, Centers for Disease Control and Prevention
- HAART, highly active antiretroviral therapy
- HIV, human immunodeficiency virus
- IELs, intraepithelial lymphocytes
- Ig, immunoglobulin
- IVDA, intravenous drug abusers
- mAbs, monoclonal antibodies
- NA, nucleoside analogues
- SIV, simian immunodeficiency virus
- TCR, T cell receptor
Despite numerous reports on intrinsic B cell defects in the systemic immune system of human immunodeficiency virus (HIV) infected subjects (reviewed by Scamurra and colleagues1 and Moir and colleagues2), only a few studies have described alterations in humoral mucosal immunity in such patients. Moreover, existing reports are remarkably conflicting,3,4 and studies have rarely been based on valid quantitative determinations of intestinal immunoglobulin (Ig) producing cell numbers. Information on perturbations in intestinal IgA or IgG subclass proportions and a possible “compensatory” increase in IgM producing cells, as seen in selective IgA deficiency,5 is virtually lacking in acquired immunodeficiency syndrome (AIDS).
A semiquantitative in situ immunofluorescence study of AIDS patients reported that the number of jejunal IgA producing plasma cells was dramatically reduced, suggesting local B cell deficiency as a contributing cause of opportunistic infections.6 Conversely, a study of HIV infected homosexual men reported only a slightly reduced number of IgA plasma cells in rectal mucosa.7 Yet others have found no reduction in intestinal IgA producing cells in AIDS.8,9 Both variable patient characteristics and different methodology may explain such discrepancies. Notably, however, oral cholera vaccination was reported to induce a specific IgA cell increase in the small intestine of HIV infected subjects, as revealed by the ELISPOT method,10 and a recent study found a normal intestinal VH gene repertoire for intestinal plasma cells in such patients.1
Here, we studied alterations in Ig class and subclass producing immunocytes (B cell blasts and plasma cells) by two colour immunofluorescence in situ staining in duodenal biopsies from HIV-1 infected patients with advanced AIDS. In addition, we related the intestinal distribution of such cells to systemic immune parameters, such as the number of circulating B cells (CD19+), T cells (CD4+ and CD8+), and β2 microglobulin (β2-M), as well as to clinical manifestations, treatment combinations, and various stages of disease progression.
This long term study gave us the opportunity to evaluate intestinal B cell perturbations in severely immunodeficient patients during a period of relatively simple treatment (1991–96) compared with that seen after highly active antiretroviral therapy (HAART).11,12 A successful HAART regimen leads to restoration of systemic immunity.11–13 Because the mucosal route may be used for future preventive or therapeutic vaccination against HIV, it would be important to know if HAART alone can help to restore local immune responsiveness.14 Here we demonstrated that hyperactivation occurs in the intestinal B cell system of poorly treated AIDS patients while HAART significantly improved mucosal immune homeostasis in association with reduction of the HIV load and/or increase in the circulating CD4+ T cell level.
MATERIALS AND METHODS
Patients
Duodenal biopsy specimens and peripheral blood samples were collected consecutively during the period 1991–98 from 31 HIV-1 infected subjects (six women, median age 36 years (range 26–40); and 25 men, median age 39 years (range 26–52)). Eighteen were homosexual men, eight were intravenous drug abusers (IVDA), and five had experienced heterosexual virus transmission (all in Africa). The endoscopic procedure was carried out due to gastrointestinal symptoms. Similar tissue and blood samples were obtained from 11 age matched HIV seronegative healthy control subjects who volunteered for endoscopy.
Serum antibody levels to HIV-1 were determined by ELISA (Organon Teknika, Boxtel, the Netherlands; or Abbott, Wiesbaden-Delkenheim, Germany) and confirmed by western blotting (DuPont, Wilmington, Delaware, USA). When clinically classified according to the criteria of the Centers for Disease Control and Prevention (CDC, Atlanta, Georgia, USA), six subjects were staged as group CDC IVA/B, 23 as group CDC IVC1, and two as group CDC IVD—the latter 25 fulfilling criteria for the diagnosis of AIDS. Because most of the patients had late stage AIDS, CD4+ cell counts were similar. Also, methodology for HIV RNA determination was available only after August 1996. Therefore, we chose to divide HIV-1 infected subjects into three clinical subgroups according to the duration of survival after duodenal biopsy: group I, AIDS related complex (ARC)/AIDS (still alive after 31–60 months; n = 11); group II, late stage AIDS (survival, 7–41 months; n = 13); and group III, premortal AIDS (survival, <5 months; n = 7). We found this classification most useful in a previous HIV study.15 Median survival time within groups II and III after the first HIV positive serum test was 81 months (range 11–156; n = 20)
Informed consent was obtained from all patients, and the study was approved by the Regional Ethics Committee II.
Clinical features
All HIV positive subjects suffered from different opportunistic and/or non-opportunistic infections. Eight of the patients had chronic intermittent diarrhoea of which two had cryptosporidiosis, two systemic cytomegalovirus infections, and four herpes simplex type II infection; 13 had oesophageal candidiasis; six suffered from systemic infection with Mycobacterium avium intracellulare complex, and seven showed symptoms of wasting (>10% unwanted weight loss). In addition, one patient had skin or mucosal lesions consistent with Kaposi’s sarcoma and one had non-Hodgkin’s malignant B cell lymphoma. Other serious infections such as Pneumocystis carinii pneumonia were found in one patient, two had toxoplasmosis (encephalitis), six chronic hepatitis C, and one tuberculous lymphadenitis (table 1).
Clinical and immunological features of human immunodeficiency virus 1 (HIV-1) infected patients in relation to treatment regimen
Four patients still received antiretroviral monotherapy with zidovudine at the time of sampling, eight also used other nucleoside analogues (NA) such as didanosine or stavudine (d4T), 11 tolerated satisfactorily combination therapy with one of these drugs together with lamivudine and HIV proteinase inhibitors such as indinavir (Crixivan) or nelfinavir (Viracept), usually called HAART, whereas eight others had discontinued all antiretroviral treatment because of intolerable side effects. None received Ig replacement therapy.
Quantitation of Ig isotypes, B lymphocytes, T cell subsets, β2 microglobulin, and HIV RNA in peripheral blood
Measurements of serum IgG, IgA, and IgM were performed by nephelometry with commercial standards (Behringwerke, Marburg, Germany) whereas quantification of serum IgG subclasses was performed with monoclonal antibodies (mAbs) in commercial kits (The Binding Site, Birmingham, UK). Blood samples were collected as near the time of biopsy as possible (usually within 1–2 hours before) and analysed on the same day, or frozen at −20°C or −70°C for later analyses.
CD19+ B cells, and CD4+ and CD8+ T cells in peripheral blood were counted by a standardised flow cytometric method. β2-M was measured by a microparticle enzyme immunoassay (Abbott IMX; Abbott Laboratories, Abbott Park, Illinois, USA). HIV RNA was measured by a standardised reverse transcriptase-polymerase chain reaction assay (Amplicor HIV-1 Monitor; Roche Diagnostic System, Brachburg, New Jersey, USA). The detection limit of the kit was 400 HIV-1 RNA copies/ml; lower values were also included. Eleven healthy HIV seronegative adults with normal serum Ig levels served as controls.
As normal reference data for circulating lymphocyte subsets, we used results from 60 healthy HIV seronegative blood donors16 recorded as described previously.17 Reference data from 18 similar donors were also available in our laboratory for serum concentrations of β2-M. The HIV RNA level in normal controls was set at <400 copies/ml plasma.
Tissue sample collection
All gastrointestinal endoscopies of HIV positive patients were performed solely on clinical indications, mostly to evaluate symptoms such as dysphagia, diarrhoea, or cachexia. Multiple mucosal biopsy samples were obtained endoscopically (Olympus GIF K10) from the distal duodenum of both HIV positive patients and controls. Endoscopic signs of chronic inflammation were occasionally observed in the distal oesophageal (three patients), prepyloric gastric (one patient), or duodenal (two patients) mucosa. Two specimens from each subject were processed for conventional histological evaluation. Other specimens were fixed in 2% paraformaldehyde for electron microscopic evaluation or processed for immunohistochemistry (see below).
Histological evaluation
A tissue section from each biopsy series was stained with haematoxylin and eosin for histological evaluation. In addition, scanning electron microscopy was performed to classify villous changes, as previously described.18 Such combined evaluation showed normal villi in all 31 HIV positive subjects. Only two patients had histological signs of moderate chronic duodenal inflammation. All biopsy control subjects had histologically normal duodenal mucosa.
Two colour immunofluorescence staining
Prior to ethanol fixation and low temperature paraffin embedding, biopsy specimens were extracted in cold isotonic phosphate buffered saline, pH 7.5, for 24–48 hours to remove interstitial diffusible Ig components.19 At least 10 serial sections from each tissue block were cut at 6 μm, dewaxed, and subjected to two colour immunofluorescence staining. The method used has been described previously, including characteristics of the fluorochrome conjugates,20 the source of IgG subclass specific mAbs,21 and other details of the staining procedure.22 Briefly, each of four serial sections was subjected to paired staining for one of the four IgG subclasses and total IgG by first applying murine mAb (ascetic fluid 1/800) to IgG1 (HP6070, clone 2C7), IgG2 (HP6009, clone GOM2), IgG3 (HP6048, clone CB1-AH7), or IgG4 (HP6011, clone RJ4) and subsequently a mixture of fluorescein labelled (“green”) rabbit antimouse IgG and rhodamine labelled (“red”) anti human IgG (γ chain specific) conjugate. A similar mAb based staining procedure was used to evaluate the IgA1 (clone 69–11.4) and IgA2 (clone 16–512H5) subclasses22 in relation to total IgA, as detailed elsewhere.20 In addition, pairs of fluorescein and rhodamine labelled antihuman heavy Ig chain conjugates were applied to determine the mucosal IgG, IgA, and IgM immunocyte class distribution by direct staining23 with the following specificity combinations: μ chain (“red”) and γ chain (“green”); γ chain (“red”) and α chain (“green”); and α chain (“red”) and μ chain (“green”). All incubations took place at room temperature for 20 hours.
Fluorescence microscopy and mucosal immunocyte enumeration
Cells with a distinctly fluorescent cytoplasm (immunocytes) were observed in a Leitz Orthoplan microscope equipped with ×10, ×25, and ×40 immersion objectives, an ×10 ocular, and a Ploem-type vertical illuminator with interference filters for selective observation of red or green emission. Results were recorded by single and double exposures on Ectachrome professional 800/1600 ASA daylight film.
The IgM:IgG immunocyte ratio in each specimen was determined by enumerations of red IgM cells (median 149, lower range 19) and green IgG cells (median 20, lower range 5) in the same sections. Also, IgG/IgA and IgA/IgM staining combinations (see above) were performed to evaluate the complete IgM:IgA:IgG duodenal immunocyte ratio for every subject. In addition, a median of 60 cells (lower range 32) with red (IgG specific) emission were examined for concomitant green (IgG subclass specific) fluorescence. The proportion of immunocytes containing one of the four IgG subclasses was then calculated in relation to the total number of IgG producing cells detected in the evaluated area of the same section. Several series of sections often had to be counted to obtain a sufficiently high number of IgG cells. The reliability of this approach was attested to by the fact that the proportions of green cells (all four subclasses) on average added up to nearly 100% (median 94.3%, range 76.9–111.8%) for each specimen. The IgA subclass proportions were evaluated with a similar approach, providing a median sum of 101.5% (range 78.6–108.2%) in HIV positive patients and 99.6% (range 84.1–129.7%) in controls.
The total number of each immunocyte isotype was based on counts made in a defined “mucosal tissue unit” constituting a 6 μm thick and 500 μm wide section block of the mucosa at full height from the muscularis mucosae to the tip of the villi. We used a previously described modification24 of our original quantitative method25 by photographing the “red” IgM immunocytes in a serial section from each specimen through an ×10/0.45 Leitz immersion objective, including a well oriented and morphologically satisfactory field at each end of the section. Colour slides were subsequently projected at a magnification of ×500 on a screen, and the 500 μm wide mucosal unit was defined. The total number of IgM immunocytes per unit was enumerated, and the corresponding numbers of the other immunocytes were calculated on the basis of the previously determined isotype ratios. All enumerations were performed by the same observer throughout the study without knowledge of the actual clinical data. The reproducibility of this approach was excellent, as documented in previous studies.24,26,27 The same microphotographs were used to determine total mucosal height (μm) from the muscularis mucosae to the tip of the villi.25
Statistical analysis
Differences among the various categories of HIV positive patients and controls were determined by the non-parametric Mann-Whitney test for unpaired samples (two tailed), as well as by the Kruskal-Wallis test (χ2 approximation) for multiple samples. Correlations between the immunocyte proportions (IgG, IgA, and IgM classes as well as IgG subclasses) and corresponding serum levels at the time of biopsy sampling were determined by the Spearman rank correlation test (SPSS for Windows), as were correlations between mucosal immunocyte Ig classes or subclasses and circulating B cell subsets or β2-M in HIV positive patients.
RESULTS
Mucosal immunocyte distribution
The median proportions of duodenal IgA (74.6%), IgM (19.5%), and IgG (3.4%) immunocytes in HIV positive patients were similar to those in healthy controls (median 74.0%, 21.0%, and 3.4%, respectively). However, the total number of Ig producing cells was significantly increased (p<0.008) in patients compared with controls (median 175 v 120 cells/mucosal unit) and the same was true for the IgA class (p<0.02), but not for IgM and IgG considered separately (fig 1). This increase was not explained by thickening of the mucosa—the total height of which was, on average, lower in HIV positive patients (median 330 μm) than in controls (median 425 μm). Regarding the clinical subgroups, subjects with mucosal infections such as P carinii pneumonia, cryptosporidiosis, or candidiasis often showed especially high duodenal IgA immunocyte counts (fig 2).

Scatter diagram showing the number of duodenal IgA, IgM, and IgG producing cells per mucosal section length unit (500 µm) in human immunodeficiency virus (HIV) positive patients compared with healthy controls. Vertical columns represent medians. Total mucosal height (mh) from muscularis mucosae to tips of villi is similarly indicated. *p<0.02 versus controls.
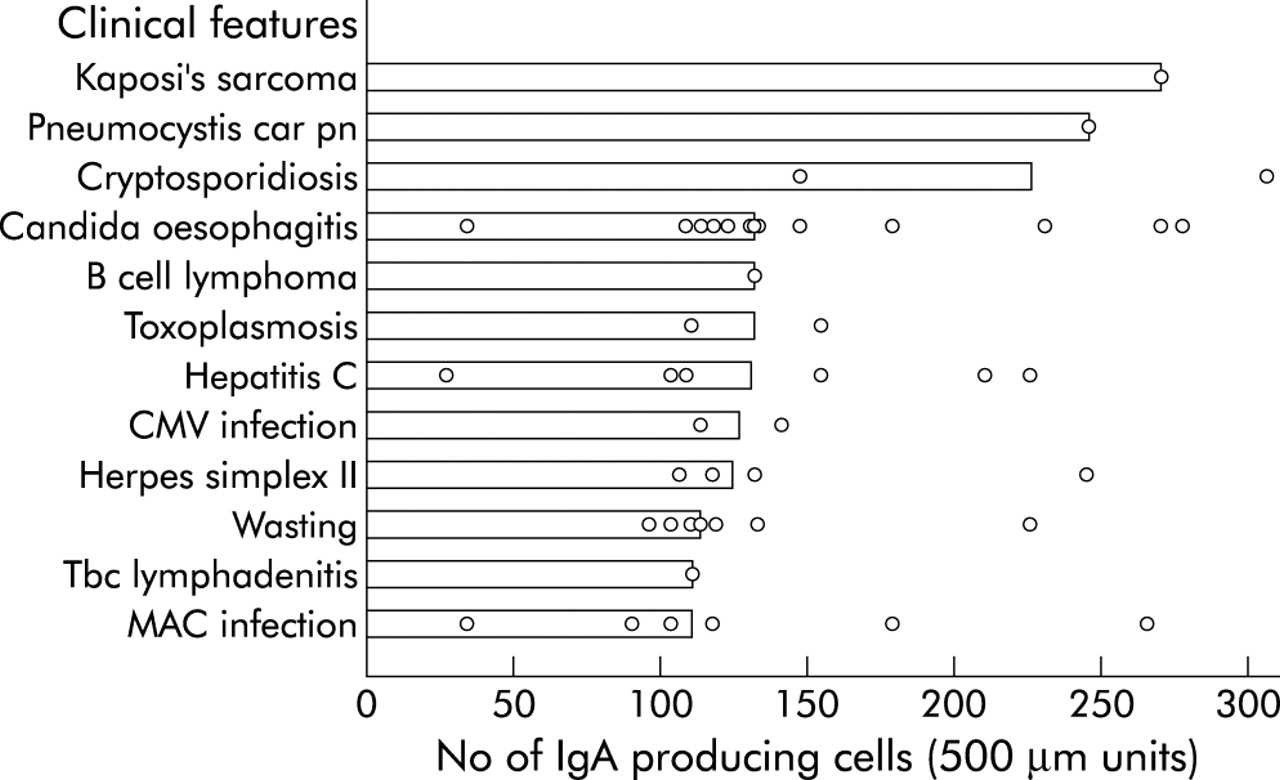
Scatter diagram showing the number of duodenal IgA producing cells per mucosal section length unit (500 μm) in relation to clinical features of individual human immunodeficiency virus (HIV) positive patients. Medians are represented by horizontal columns. CMV, cytomegalovirus; MAC, Mycobacterium avium intracellulare complex.
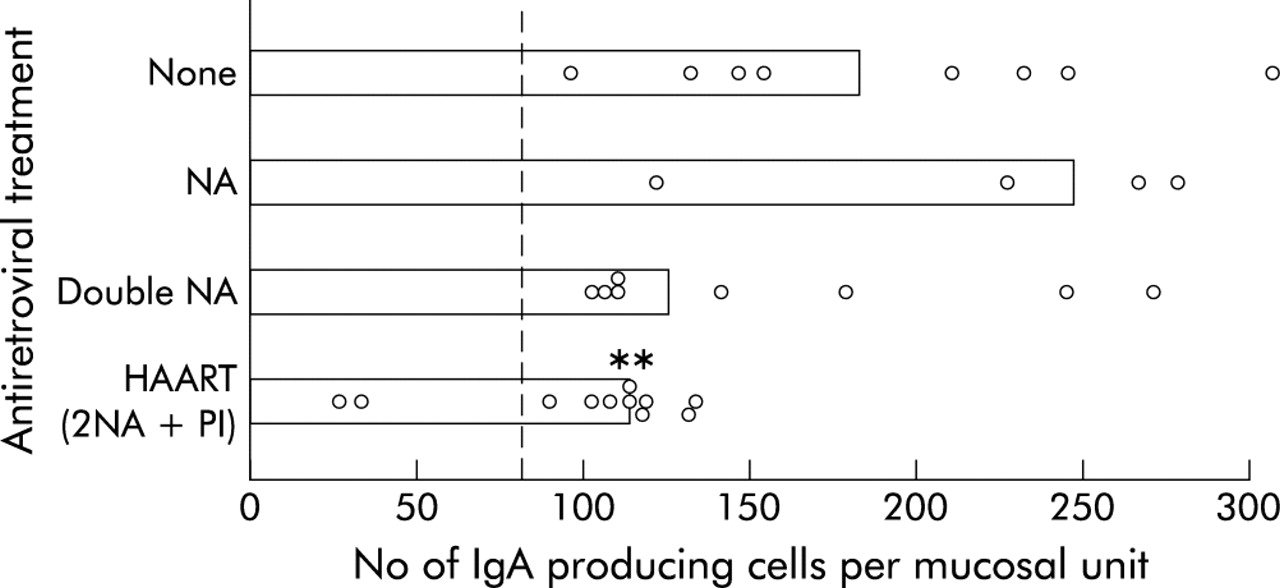
When we compared the number of duodenal IgA immunocytes in different treatment groups (fig 3), patients receiving HAART showed significantly (p<0.005) lower numbers (median 112 cells/mucosal unit) than those without antiretroviral treatment (median 181 cells/mucosal unit). There was likewise a decrease in the total immunocyte number, including all three Ig classes (p<0.003), in patients on HAART compared with those receiving no antiretroviral treatment. Also, patients on double nucleoside analogues (2 NAs) tended to have a lower number of IgA immunocytes (median 124 cells/mucosal unit) compared with those receiving no or single nucleoside therapy (median 181 and 245 cells/mucosal unit, respectively).

Scatter diagram showing the number of duodenal IgA producing cells in human immunodeficiency virus (HIV) positive patients according to administered antiretroviral treatment. Medians are represented by horizontal columns. Mean number in the healthy control group is indicated by a broken vertical line. NA, nucleoside analogue; PI, proteinase inhibitor; HAART, highly active antiretroviral therapy. **p<0.005 versus untreated.
The proportion of IgG1 immunocytes (fig 4) was increased (p<0.02) in HIV positive patients (median 81.8% of total IgG) compared with healthy controls (median 68.4%). Also, IgG3 immunocytes (median 3.4% v 1.9% in controls) and the IgA2 immunocyte proportion (median 32.1% of total IgA v 27.5% in controls) tended to be increased, although IgA1 (median 69.2% of total IgA) was the dominating duodenal IgA isotype as normal. Notably, patients receiving HAART tended to show lower IgG1 ratios than those without antiretroviral treatment (median 77% v 84%).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Scatter diagram showing the percentage distribution of duodenal IgG subclass producing cells in human immunodeficiency virus (HIV) positive patients compared with healthy controls. Vertical columns represent medians. *p<0.02 versus controls.
Infection parameters in peripheral blood related to mucosal immunocytes
When circulating T lymphocyte subsets in HIV positive patients were compared with values for healthy blood donors,16 the number of CD8+ cells tended to be reduced (median 0.37×109/l (range 0.057–1.87×109/l) v 0.405×109/l (range 0.18–1.23×109/l)), and the number of CD4+ cells was, as expected, significantly decreased (median 0.022×109/l (range 0.0012–0.25×109/l) v 0.815×109/l (range 0.5–1.58×109/l); p<0.0001). Two clinical groups contributed more than other patients to this low value: group II (late stage AIDS) and group III (premortal AIDS) with 0.019 and 0.015×109/l, respectively, while subgroup I (ARC/AIDS) showed a less reduced CD4+ cell number (median 0.114×109/l (range 0.009–0.25×109/l)).
Plasma HIV RNA could be determined in only 12 HIV positive patients. Levels increased as expected terminally, revealing the following median virus loads: group I, 57 000 copies/ml; group II, 70 000 copies/ml; and group III, 191 000 copies/ml. Compared with untreated patients, we found a trend towards a higher median CD4+ cell number (0.086×109/l (n = 10) v 0.016×109/l (n = 8)) and a lower median plasma HIV RNA level (42 000 copies/ml v 93 500 copies/ml; n = 2) in patients on HAART. Also, untreated patients tended to have increased mucosal height (median 403 μm; n = 8) compared with the HAART group (median 325 μm; n = 11). Surprisingly, however, we found only one untreated patient with histologically verified duodenal inflammation, as we also did in the HAART group.
All HIV positive patients are listed in table 1, categorized as in fig 3, to display individual clinical and immunological features in relation to treatment regimen. It is apparent that reduction of the HIV load and/or increase in the CD4+ T cell level in blood was associated with HAART. However, the HIV mRNA level remained quite high in four of the 11 patients receiving HAART. Notably, two of them had been treated for only 6–8 days while the two others may have developed resistance to the drugs after 10–15 months. In three of these four patients, the duodenal IgA immunocyte number remained relatively high (table 1).
For the whole AIDS material, no relationship was found between the relative or absolute numbers of mucosal immunocytes and level of circulating CD4+ or CD8+ T cells, CD4:CD8 ratio, or B cell numbers in peripheral blood. Likewise, when duodenal IgA immunocyte counts were compared with serum levels of IgA, no correlation was found. However, among the three clinical groups, a trend towards increased duodenal IgA immunocyte number from group I (median 112.2 (range 25.5–224.8)) towards group II (median 135.7 (range 32.4–276.1)) was found but this was not apparent for group III (median 121 (range 88.9–305.4)).
Serum immunoglobulins and β2 microglobulin
Hypergammaglobulinaemia (mostly IgG) was found in 16 of the blood samples (median 18.3 g/l (range 8.7–44.6 g/)l). IgG1 (median 11.2 g/l) and IgG3 (median 1.8 g/l) subclasses were particularly increased. IgA level tended to be only slightly increased in the three clinical groups (medians 3.9, 3.4, and 3.1 g/l, respectively). Also, IgM level (median 1.5 g/l) was quite normal. The lowest IgA level (median 3.1 g/l) was observed in patients on HAART, and the highest in those without antiretroviral treatment (median 4.2 g/l).
The β2-M level in HIV positive patients (median 3.7 mg/l, n = 28) was significantly increased (p<0.0001) compared with controls (median 1.2 mg/l). The median level was fairly similar among the three clinical groups (4.2, 3.5, and 3.6 mg/l, respectively). No relationship was observed between serum β2-M and circulating CD4+ or CD8+ cells, duodenal IgA immunocytes, or any of the other immunological variables.
Long time survivors
Four of the 11 patients in group I (ARC/AIDS) were so called “long time survivors”, living for 3–5 years after inclusion in the study and altogether for 15–17 years after seroconversion. Three were IVDAs and one was homosexual. All had numbers of duodenal IgA immunocytes and circulating CD4+ cells similar to the other HIV positive patients but often relatively low serum IgG1 levels. Serum IgA and β2-M concentrations were in the upper normal range, and the plasma HIV RNA level was markedly raised (median 85 000 copies/ml). Only two received HAART and one was not treated with NAs. The only one with undetectable HIV RNA, a 38 year old female IVDA on antiretroviral treatment with stavudine (d4T) alone, was surviving on methadone therapy, although she had wasting syndrome, AIDS dementia, and chronic hepatitis B and C virus infection. She had remarkably high serum Ig levels, especially IgG (33.6 g/l), and also relatively many duodenal IgG immunocytes (15.2%), mainly of the IgG1 subclass, which was also the major serum isotype. All other immunological variables were near average AIDS values.
DISCUSSION
The apparent paradox that systemic B cell hyperactivity in vivo is associated with poor immune responsiveness in vitro and an ineffective antibody response in HIV positive patients appears to be directly related to virus replication.2 Here we showed that the same paradox exists in the gut, and that intestinal B cell hyperactivity can be substantially controlled by effective antiretroviral therapy such as HAART. However, the intestinal B cell system appears to be more robust than the systemic counterpart because overproduction of IgA in the lamina propria has not been consistently found in previous studies of HIV positive patients.1,3,6–9
The increased duodenal IgA response found in our in situ investigation was probably not significantly directed against HIV. Thus others have demonstrated decreased levels of HIV specific intestinal IgA antibodies in AIDS compared with early HIV infection when duodenal biopsies were cultured ex vivo and mucosal extracts analysed by western blotting.28 Likewise, there was a lack of simian immunodeficiency virus (SIV) specific IgA response in the gut of SIV infected non-human primates.29 Notably, however, mucosal IgG antibodies were detected both against HIV28 and SIV,29 apparently reflecting systemic involvement of local immunity with increased mucosal IgG synthesis,29,30 as previously noted in several types of intestinal disease.20,25,26 Here we likewise found a slightly increased number of duodenal IgG producing cells in AIDS patients, and a significantly increased proportion of the IgG1 subset. This isotype has strong complement activating and opsonic properties,20,21 and can induce antibody dependent cell mediated cytotoxicity. Therefore, this systemic type of local immunity could contribute to altered homeostasis in the intestinal mucosa.31
An increase in duodenal IgA immunocyte number appeared to be related to different treatment subgroups and was quite small in most patients on HAART. This finding appeared to reflect control of viraemia, as revealed by reduced plasma HIV RNA levels. To a certain degree this local immune restoration was paralleled by a favourable circulating CD4+ T cell number. Conversely, high numbers of duodenal IgA immunocytes were often seen in patients suffering from severe secondary mucosal infections such as P carinii pneumonia, cryptosporidiosis, or candidiasis.
Only a slight difference in total duodenal immunocyte numbers appeared between clinical group I (ARC/AIDS) or group II (late stage AIDS) and group III (premortal AIDS), although the latter category tended to have decreased IgA cell counts. This could reflect a relative deficiency of anti-inflammatory IgA in the intestinal mucosa.5,32 We have previously reported a marked duodenal decrease in potentially cytotoxic T cell receptor (TCR) γ/δ+ intraepithelial lymphocytes (IELs) in a similar premortal AIDS group.15 Thus combined deficiency of IgA immunocytes and TCR γ/δ+ T cells in the end stage of AIDS could reduce the antimicrobial defence at the mucosal surface and in part be responsible for a fatal outcome.
Circulating β2-M probably reflects cellular interferon γ stimulation and was found to be significantly elevated in our HIV positive patients, as previously reported in AIDS33 and other types of immunodeficiency, such as common variable immunodeficiency34 and IgA deficiency.34,35 We previously reported that β2-M was inversely correlated with duodenal TCR γ/δ+ IELs in end stage AIDS.15 That such elevation was not observed in the present study can most likely be ascribed to the beneficial effect of HAART on advanced patients, or perhaps that the preterminal group died of diseases unrelated to AIDS (for example, cerebral haemorrhagia, cardiac left ventricle dysfunction, aortic valve stenosis, and neurolues).
Studies of the approximately 5% long time AIDS survivors have gained increasing importance in HIV research. Four such patients in our study did not reveal any special findings, except that one with a particularly good prognosis (low HIV RNA level) had a rather high level of serum IgG and relatively many duodenal IgG immunocytes. This may suggest good complement activating systemic type of HIV specific immunity at the mucosal surface of this patient because such intestinal IgG antibody activity is known to occur in AIDS.4,28
In conclusion, mucosal expansion of duodenal IgA and IgG1 (and less so IgG3) immunocytes was shown to occur in AIDS patients, but such hyperactivity of the intestinal B cell system is significantly controlled by HAART. Secondary intestinal infections are common in AIDS, and it is important to define how the adaptive mucosal defence behaves in HIV positive patients. Although the intestinal immune system appears to be more robust to HIV induced perturbations than the systemic counterpart, mucosal homeostasis clearly depends on effective antiretroviral therapy. Such information may be useful for future development of mucosal AIDS vaccines.14
Acknowledgments
This study was supported by grants from the Research Council of Norway, the Norwegian Cancer Society, Anders Jahre’s Foundation for the Promotion of Science, the University of Oslo, and Medinnova, Rikshospitalet. We thank the technical staff at LIIPAT, the Department of Infectious Diseases, the Department of Clinical Chemistry, and the Section of Gastroenterology, Ullevaal University Hospital, Oslo, Norway, for valuable contributions. Erik Kulø Hagen and Hege Eliassen are gratefully acknowledged for assistance with the manuscript preparation.