Article Text

Abstract
Objective: To present an epicardial manifestation of the lipodystrophy syndrome, a side effect of antiretroviral treatment in HIV positive patients, which illustrates the important danger of false diagnosis.
Patient: A 52 year old man with HIV (stage C3), diagnosed 10 years previously, was being treated with a combination of nelfinavir, nevirapine, and stavudine. Echocardiographic examination showed a low echogenic pericardial space that had increased from 4 mm to 18 mm over a 10 month period. The diagnosis of paracardial adipose tissue was verified by magnetic resonance tomography. Doppler echocardiographic parameters were not significantly altered (ratio of early to late ventricular filling 0.88 v 0.73, Tei index 0.30 v 0.36).
Conclusion: Even a pericardial manifestation of lipodystrophy causes negligible functional impairment, misinterpretation of the lipodystrophy as a pericardial effusion and a subsequent puncture can have serious complications. Hence, it is strongly suggested that further differential diagnosis be used for HIV positive patients with an echocardiographic suspicion of pericardial effusion. Differential diagnosis by magnetic resonance tomography is possible.
- lipodystrophy syndrome
- HIV
- differential diagnosis
- paracardial adipose tissue
- magnetic resonance tomography
Statistics from Altmetric.com
- lipodystrophy syndrome
- HIV
- differential diagnosis
- paracardial adipose tissue
- magnetic resonance tomography
Since the introduction of antiretroviral treatment the prognosis of HIV infected patients has improved greatly.1, 2 The commonly used antiviral treatments, including a combination of nucleotide analogues, nucleoside reverse transcriptase inhibitors, and proteinase inhibitors, are well tolerated by most patients. However, during the past two years antiretroviral treatment of HIV infection has increasingly been associated with metabolic alterations.3 Most frequently, alteration of adipose tissue, including an increase in visceral adipose tissue or a decrease in peripheral subcutaneous adipose tissue (lipodystrophy), is observed. Additionally, both triglyceride and cholesterol serum concentrations can increase.4 Alterations of adipose tissue are detected mainly in superficial layers and abdominal organs; however, other parts of the human body can be affected as well. We present a paracardial manifestation of lipodystrophy, which must be differentiated from pericardial effusion.
CASE REPORT
A 52 year old man with HIV (stage C3) was admitted to our hospital. The well known HIV infection had been diagnosed 10 years previously and was treated with a combination of the protease inhibitor nelfinavir, nevirapine, and stavudine. At the time of admission, his CD4 cell count was 81 cells/mm3 and the HIV concentration < 50 copies/ml. He had no history of heart disease. Cardiac examination found no pathological results. However, signs of lipodystrophy syndrome were present, including an increased body mass index and a decrease in peripheral subcutaneous adipose tissue. Magnetic resonance tomography of the abdomen showed an increase of adipose tissue surrounding the internal organs of the intestine. Increased serum concentrations of triglycerides (4.1 mmol/l) and cholesterol (7.2 mmol/l) were detected.
Exertional dyspnoea was the indication for a transthoracic echocardiographic examination (fig 1). The first echocardiographic examination showed diastolic dysfunction with a ratio of early to late ventricular filling (E/A ratio) of 0.73 and a Tei index of 0.36.5 The left ventricle was not dilated, and contracted well. A 4 mm wide epicardial space was detected. Ten months later, echocardiographic examination showed an increase of the epicardial space to 18 mm in diameter and a calculated volume of 470 ml. The E/A ratio measured 0.88. The Tei index was 0.30. Still no signs of impaired ventricular filling were apparent.

Long axis two dimensional echocardiographic images of the left and right ventricle before and after 10 months' retroviral treatment. As indicated by the arrows (left panel), echocardiographic examination showed a tremendous increase of the low echogenic seam, compared with the results 10 months previously (right panel).
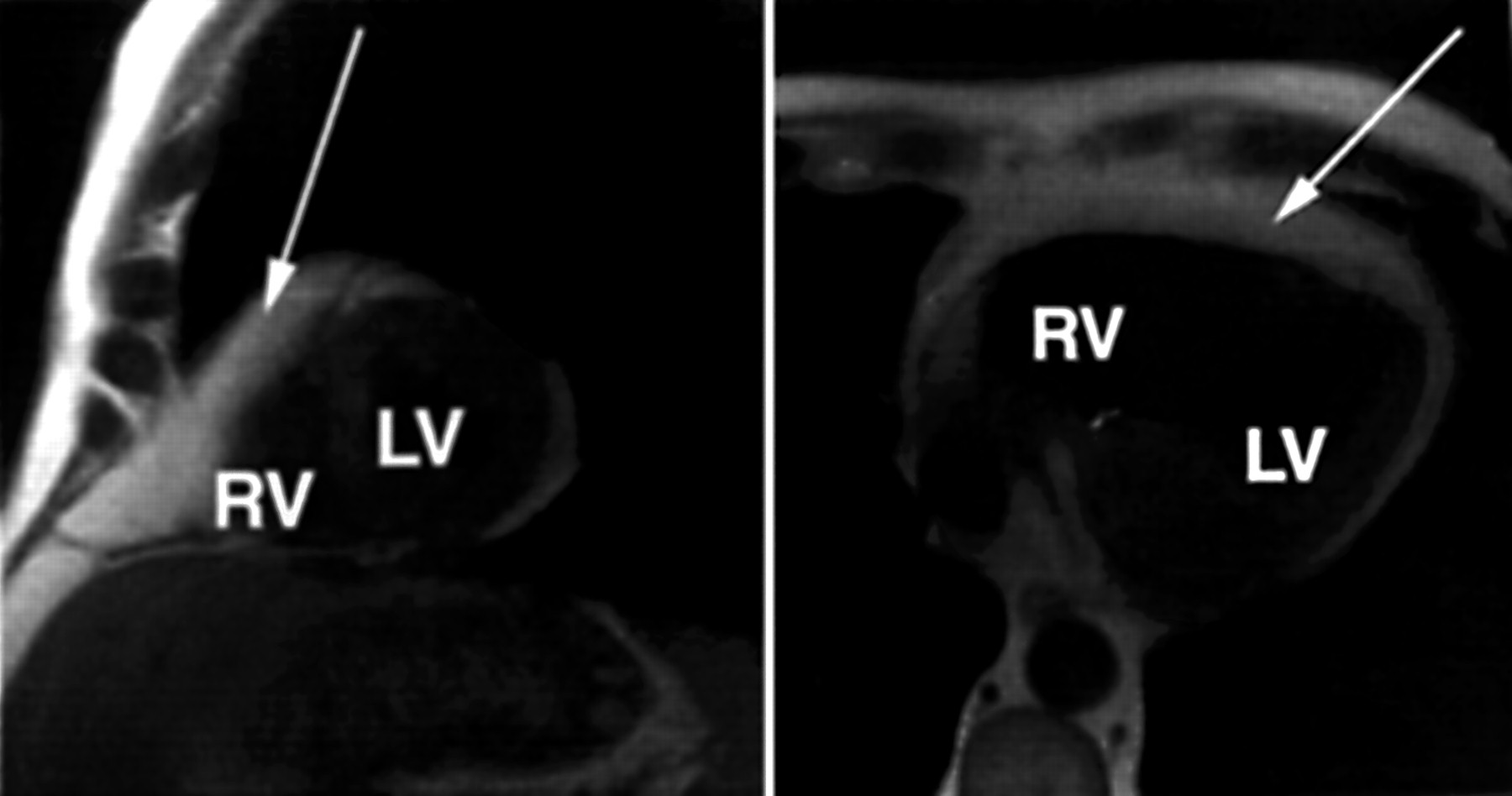
Because both paracardial adipose tissue and pericardial effusion display as a low echogenic edge, magnetic resonance tomography was performed. The T1 weighted turbo spin echo sequences showed a high signal intensity around the ventricles indicating paracardial adipose tissue. However, mediastinal adipose tissue and not epicardial adipose tissue was increased. No fatty infiltration of the myocardium was observed (fig 2).

{kind=link}
{kind=link}
ECG triggered T1 weighted turbo spin echo magnetic resonance images acquired in the short axis plane (left panel) and in the transverse plane (right panel) through the middle of the left and right ventricles. Note that the echocardiographic pericardial finding can clearly be identified as an increase of paracardial adipose tissue. The paracardial adipose tissue is sharply demarcated from the myocardium. There is no increase of adipose tissue inside the myocardium.
DISCUSSION
The presented patient had the typical signs of the lipodystrophy syndrome, including changes in superior lipid tissues and increases of adipose tissue surrounding the abdominal organs. In addition, a paracardial manifestation of the lipodystrophy syndrome was detected. While in the normal heart adipose tissue is located mainly near the coronary vessels and at the apex of the heart, the adipose tissue in the present patient surrounded both ventricles. Additionally, the adipose tissue increased from 4 mm to 18 mm in diameter over 10 months.
Lipodystrophy is a symptom in many HIV positive patients, based on alterations of adipose tissue in the human body.6 Adipose tissue is reduced especially in the cheeks, arms, and legs, while it is increased elsewhere, mainly in the neck and abdomen. However, these changes affect not only the superficial adipose tissue layers but also internal organs. Primarily organs of the abdomen, such as liver, kidneys, and bowel, are surrounded by thick layers of adipose tissue. The changes of abdominal adipose tissue are often accompanied by gastrointestinal dysfunction. Surprisingly, the tremendous increase of paracardial adipose tissue, as shown in the present case report, did not worsen ventricular function. Compared with the previous echocardiographic result, the diastolic function improved slightly and there were no signs of restriction or constriction of the ventricles. The Tei index, a measure of global ventricular function, was not increased in either echocardiographic analysis.
Although the paracardial adipose tissue did not worsen ventricular function, further differentiation of an echogenically low epicardial space is important. The usual cause of a low echogenic space in echocardiography is a pericardial effusion. Additionally, previous studies showed that pericardial effusion is often associated with HIV infection.7–10 Therefore, the first diagnosis might be a pericardial effusion. However, in patients with a paracardial adipose tissue seam, a puncture for therapeutic aspiration or diagnostic reasons following an incorrect diagnosis of pericardial effusion may have fatal consequences. Puncture of the epicardial adipose tissue would not produce pericardial fluid and a push forward may lead to perforation of the right or left ventricle and the potential for cardiac tamponade.
Therefore, we strongly suggest that differential diagnosis be used in HIV positive patients under retroviral treatment who exhibit a low echogenic space. In particular, if left ventricular function is not impaired, a paracardial manifestation of lipodystrophy syndrome should be suspected.
Magnetic resonance tomography can reliably differentiate between pericardial fluid and paracardial adipose tissue. T1 weighted sequences with and without fat suppression can clearly distinguish adipose tissue from pericardial fluid. Because of the low Houndsfield units of adipose tissue, computer tomography may be used as an alternative to distinguish between adipose tissue and pericardial fluid. Although these techniques are much more expensive, we strongly suggest that HIV positive patients under retroviral treatment undergo differential diagnosis especially if changes in ventricular function such as E/A ratio and Tei index are only slight.
REFERENCES
Linked Articles
- Miscellanea