Article Text

Abstract
Background: Some advocates of HIV prevention have counterposed programmes aimed at reducing numbers of sex partners to programmes aimed at increasing condom use. In this polarised debate, arguments about their relative effectiveness have been based on limited evidence.
Objectives: To explore the theoretical impact of changing partner acquisition rates and condom use on the population level incidence of sexually transmitted infections different in different populations.
Methods: A standard deterministic compartmental model of the transmission dynamics of a sexually transmitted disease is solved numerically. The change in behaviour required to prevent a single case of infection is calculated for a range of scenarios.
Results: When the transmission probability per sex act is low across partnerships, the incidence of infection responds similarly to changes in partner numbers and numbers of unprotected sex acts. High transmission probabilities alter the relationships, with the effectiveness of increasing condom use improving as the background number of unprotected sex acts decreases. The divergence in patterns of impact is marked when there is heterogeneity in the transmission probability per act across partnerships.
Conclusions: Both reducing numbers of sex partners and increasing condom use can lower the incidence of sexually transmitted infections. Unfortunately, there is no simple and general rule that will allow the efficiency of interventions to be calculated. Heterogeneity in transmission probability across infections, which may occur for both bacterial and viral infections, can reduce the effectiveness of condom use as an intervention if that use is inconsistent.
Statistics from Altmetric.com
The relative merits of HIV prevention programmes which aim to reduce numbers of sexual partners or to increase the use of condoms and thereby reduce the number of unprotected sex acts have become a subject of debate.1 2 This is epitomised by the USA’s funding for international AIDS relief earmarking funds explicitly for Abstinence and Behaviour Change Programmes based on a concern about overemphasising other prevention programmes that include condoms.3 On both sides of this polarised debate arguments often seem to be based on a priori beliefs rather than empirical evidence or theoretical considerations. Unfortunately, the provision of valid evidence of effectiveness is not straightforward, partly because the interventions are complex and partly because the relationship between intervention and impact is not straightforward.
In biomedical research the efficacy of interventions is best determined by randomised controlled trials.4 However, for complex interventions aimed at preventing infectious diseases through a change in the behaviour of a population, the unit of randomisation needs to be the community and the trial end point needs to be the incidence of infection.5 Such trials are necessarily large, complex, expensive and take several years—and their findings are hard to generalise.6 Of the two such trials with published results, neither has shown an impact on the incidence of HIV.7 8 Failing such definitive—if context-specific—evidence, recourse can be made to intermediate steps in a chain linking the funding of interventions to their impact. The link between funding and impact can be made in a theoretical framework where funding provides inputs, leading to outputs which are to generate an outcome which, in turn, is to have an impact.9 Here, if we know through randomised controlled trials that the activities constituting an output produce an outcome measured in terms of risk behaviours, and we also know that these risk behaviours change the incidence of a sexually transmitted infection (STI), then we can argue that the intervention will be effective. The outcomes might be self-reported delays in first sex, reduced numbers of sexual partners, reduced contact with potentially risky partners such as sex workers or increases in condom use.10 More convincing still, an individual randomised controlled trial may be able to show a reduced incidence of a STI in those receiving an intervention.11 12 However, even in this case we still need to assume that the reduced incidence for the individual will translate into an effect at the population level.
Because controlled trials have been unable to demonstrate the relationship between changing risk behaviour and the incidence of STIs, we have had to rely on observational studies and theoretical models. In the former, changes in the incidence of infection can be related to observed changes in behaviour,13–15 but it is often difficult to separate out the influence of different changes in behaviour and even more difficult to attribute them to specific interventions. In the latter, explicit assumptions are made about patterns of risk behaviour and their influence on the incidence and prevalence of STIs is explored.16 17
Since STIs are, by definition, transmitted via unprotected sex acts within sexual partnerships, reducing the frequency of either unprotected acts or partnerships should lower their incidence. The very familiar equation for the basic reproductive number R0 = β.c.D represents the reproductive potential of the infection in an entirely susceptible and, crucially, homogeneous population where everyone has the same sexual behaviour. Since the basic reproductive number is the product of transmission probability per sexual partnership (β), the mean rate of sexual partner change (c) and the mean duration of infection (D), a particular percentage change in either the rate of partner acquisition or the transmission probability per partnership is equivalent, and a 50% reduction in transmissibility would have the same impact as a 50% cut in the mean rate of sexual partner change. Unfortunately, the non-linear relationships between risks and infections that characterise infectious disease epidemiology and the heterogeneities in risk behaviour invalidate any such simplistic assumption.18
Initial models of the spread of STIs assumed that acquiring an infection depended upon the rate of acquiring sex partners.19 20 This simplifying assumption meant that, when a partnership between a susceptible and an infected individual was formed, infection was either transmitted or it wasn’t and this depended on the transmission probability per sexual partnership. An empirical justification for this was provided by the observed high transmission probability per sexual act in the case of gonorrhoea21 and the lack of a relationship within partnerships between the number of unprotected sex acts and the transmission of HIV.22 23 Such models inevitably showed that reducing rates of partner acquisition would reduce the incidence of STIs, but could not represent the use of condoms since the number of unprotected sex acts with a partnership was not included. In such a model, condoms could only be included if they were used effectively throughout a relationship and therefore equated to a reduction in partner acquisition. But, logically, if transmission takes place during sexual intercourse then, as the number of sexual acts increases, the risk of transmission within the partnership should increase. A simple Bernoulli relationship should exist and was used in a wide range of models exploring an individual’s risks of acquiring HIV or other STIs.24–28 This relationship could also be made explicit in the models with sexual partner acquisition by making the transmission probability per partnership depend upon the number of sex acts within the partnership.27–30 Just as the model population can be stratified according to rates of sexual partner change, it can also be stratified according to the number of unprotected sex acts within partnerships, or correlations between sexual partner change rates and numbers of acts per partnership can be assumed. In this paper we explore the different impact of reductions in partner numbers and of condom use (represented by changes in the numbers of unprotected sex acts per partnership) on the predicted incidence of different STIs and investigate the importance of the biological and behavioural assumptions, using a standard deterministic mathematical model of STI transmission dynamics.29 30
METHODS
The model considers an exclusively heterosexual population stratified both by sex and into three sexual activity classes with characteristic rates of sexual partner change and numbers of unprotected sex acts in each sexual partnership that they form. In the model, infection with the same agent is allowed to take on two guises which allows us to represent symptomatic and asymptomatic infections or other similar biological variations. Such a model has typically been used to represent gonorrhoea and chlamydia in a large population.19 31 However, here we use it to represent a wide range of different STIs in one framework, thereby losing some of the specific characteristics of the particular infections in order to focus on a comparison of the role of partner numbers and unprotected sex acts across infections.31 Both susceptible (Xki) and infected (Ysk,i) classes are stratified into six groups according to sex, k, (k = 1 for men and k = 2 for women, k′ refers to the opposite sex from k) and activity class (i). Infection is also stratified according to type of infection(s). The type of infection (s) is a general structure which allows for different associated parameters such as rates of recovery or transmission probabilities, but in the results presented here we use it solely in the heterogeneous examples to generate heterogeneity in transmission probabilities. The population is assumed stable with

and a fraction φk in each sexual activity class of each sex. The following ordinary differential equations describe changes in these classes:


where cki is the mean rate of sexual partner change. In these equations βs′k,i,j is the transmission probability per sexual partnership from someone of sex k′ in activity class j with infection type s′ to someone of sex k in activity class i and is a function of the transmission probability per sex act αs′k and the number of sex acts over the course of the partnership ni,j:

Note that when α is low, β is approximately proportional to n (ie, it increases approximately linearly with n) whereas, when α is high, the relationship is highly non-linear with β initially increasing rapidly with n but then increasing much more slowly as β “saturates” as it approaches its maximum value of 1.
The number of sex acts within a partnership depends upon the activity classes of both partners and is varied in different scenarios (see below).
The proportion of infections that are of type s is given by the fraction θsk. The term ρk,i,j is the probability that, when someone of sex k from group i forms a sexual partnership, it is with someone of the opposite sex from group j. The values of ρk,i,j can vary on a scale from fully assortative to random, defined by the parameter ϵ:

where δi,j = 1 when i = j and δi,j = 0 when i≠j. When ϵ = 1, mixing is fully assortative whereas, when ϵ = 0, it is random. The number of partnerships between the groups of men and women in this analysis is balanced by assuming similar patterns of behaviour across the two sexes. The rate of recovery from infection (σsk) can depend on the infection type s and includes both spontaneous resolution of infection or the impact of treatment and is the inverse of the mean duration of infection.
The model was solved numerically using a fourth order Runge-Kutta method in Berkeley Madonna. The mean rate of partner change (c) and ratios of rates between activity classes (ri) are specified, allowing the respective partner change rates to be derived.
The impact of interventions is calculated for the steady state. For simplicity we assume that changes in behaviour occur across the population. The mean rate of sexual partner change can be reduced by a fraction b so that ck,i = (1–b)c′k,i where c′k,i represents the situation in the absence of the intervention. Similarly, the proportion of unprotected sex acts can be reduced by a fraction a so that ni,j = (1–a)n′i,j.
The different STIs can be crudely represented in this framework through the choice of values for the rate of recovery from infection and the transmission probability per sex act. Broadly, a short duration of infection and a high transmission probability is associated with bacterial infections and a long duration of infection and low transmission probability per act with viral infections. Representation of further specifics of a particular infection such as a fraction of infections remaining asymptomatic and having a lower recovery rate or a fraction having a higher likelihood of infection are also possible. In the examples chosen for illustration, a bacterial infection has a mean duration of 6 months and a transmission probability per act of 0.25, whereas a viral infection has a mean duration of 10 years and a transmission probability per act of 0.01. An additional example where the mean duration of infection is 10 years and 10% of infections have a transmission probability per act of 0.25 and 90% a transmission probability per act of 0.001 is labelled as “heterogeneous”.
For illustration, a range of sexual behaviours is explored. Prior to interventions, all the results presented assume a mean rate of sexual partner change of 0.5 new partners per person per year, with 1%, 29% and 70% of both men and women falling in the three sexual activity classes, which have a ratio of rates of sexual partner change of 100 to 10 to 1, respectively. The mixing is assumed to be midway between assortative and random. These parameters generate the rates of sexual partner change and mixing probabilities presented in table 1. Five different patterns of numbers of unprotected sexual acts per partnership for each combination of partners’ activity classes are used (I–V), which are made explicit in table 1. Patterns I, II and III assume the same number of acts across all partnerships with 2, 12 and 104 acts per partnership, respectively. In patterns IV and V the number of sex acts is determined by the partner in the highest (IV) or lowest (V) activity class, respectively.
RESULTS
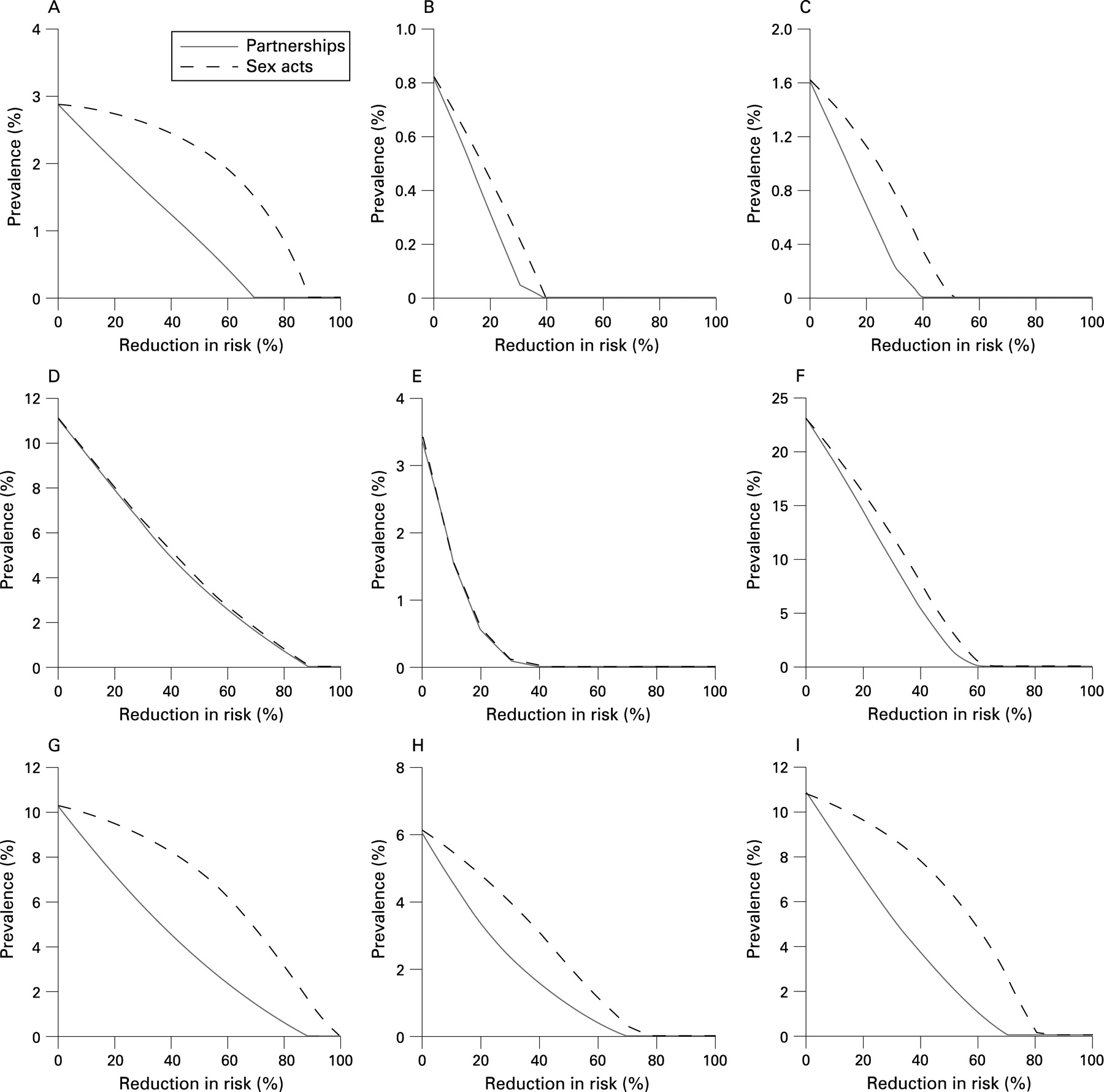
The prevalence of infection is greatly influenced by both biological parameters and patterns of sexual behaviour, with an interaction between the two. For illustration, we hold patterns of partner change constant but vary the number of acts in each sexual partnership using the five patterns (table 1). For a bacterial STI with a high transmission probability per act, moving from two acts per partnership (pattern I) to 12 (pattern II) greatly increases prevalence but a further increase to 104 acts per partnership (pattern III) has little effect because, after 12 acts, the transmission probability per partnership is already close to 1. If those with many partners have few acts across all their partnerships (pattern IV), the prevalence is similar to that when all partnerships have a low number of sex acts because those with many partners are particularly important in the epidemiology of bacterial STIs. Prevalence increases when those with many partners have an increased number of sex acts in partnerships with those with lower numbers of partners (pattern V), but this does not reach the level seen for patterns II and III as the partnerships that are key to sustained transmission (ie, partnerships between individuals who both have many partners) still only include two sex acts. Prevalence of the bacterial STIs is limited to a few percent because of the short duration of infection, meaning that infection is largely confined to those with many partners.

Representing a viral infection by changing the mean duration of infection to 10 years and decreasing the transmission probability to 0.01 leads to a much higher prevalence (fig 1B, note different axis from 1A). Here, as the number of sex acts across all partnerships increases from 2 to 12 to 104, the prevalence continues to increase as the transmission probability per partnership has not saturated after 12 sex acts per partnership. In this case, pattern IV has a higher prevalence than pattern A because the likelihood of transmission to and from those with a low number of partners plays a role. In pattern A with only two acts per partnership across all activity groups, there is insufficient transmission to sustain the infection. Prevalence is lower in pattern V than in pattern III because of the lower transmission probability per partnership in the large fraction of partnerships between those with a medium number of partners.
When there is heterogeneity in the transmission probability (α = 0.25 for 10% of infections; α = 0.001 for the rest), the prevalence of the infection is lower than the viral infection but higher than the bacterial infection (fig 1C) because of the assumed 10-year mean duration of infection. The relationship between prevalence and pattern of number of sex acts is similar to that seen for the viral STIs except that there is a relatively higher prevalence for patterns I and IV. Here, those with a high number of sex partners and few sex acts per partnership can still play an important role in the epidemiology of the infection when they acquire an infection that is one of the 10% that are of high transmission probability.
The resulting distribution of prevalence and of numbers of cases across the activity classes is illustrated for the bacterial and viral STIs for patterns of sexual acts IV and V (fig 1D and E). The prevalence is always highest in those with many sex partners, but the relative prevalence in those with many sex partners is higher for the bacterial infections. For viral STIs, if those with many partners only ever have two sexual acts per partnership (pattern IV), the prevalence is lower in this group than with bacterial STIs despite the higher overall prevalence. In all of the scenarios significant numbers of infections occur in the larger lower activity classes, but this is particularly marked for the viral infections with pattern V sex acts.
The relationship between prevalence and reductions in risk (either reduced numbers of sex partners or increased condom use) is explored in fig 2 for numbers of sex acts using patterns II, IV and V and for the biological parameters representing bacterial, viral and heterogeneous infections.

Throughout, if a sexual partnership does not exist then there is no potential for transmission of infection. As partner numbers decrease, prevalence decreases linearly in the case of bacterial STIs and non-linearly for viral and heterogeneous infections; note that the rate of decline decelerates with diminishing returns as the infection moves towards extinction. This is the opposite of what would be expected for an infection in a homogeneous population and can be explained by the heterogeneity in risk which allows large initial gains in the broad swathe of the population with low risk. With larger reductions, the infection becomes more concentrated in the small high-risk fraction of the population where it is harder to control. The change in decline is more marked for a viral or heterogeneous infection where those with lower numbers of sex partners play a greater role in transmission and when those with many partners always have a low number of sex acts per partnership (pattern IV), which reduces the relative importance of the links between the different sexual activity classes because infection is more able to persist in the lower activity classes.
The relationship between condom use and prevalence is more complex. For bacterial STIs the transmission probability per sexual partnership saturates as it approaches the maximal value of 1 over a few sex acts. To bring down the per partnership transmission probability (β) markedly, condom use has to move the number of unprotected sex acts into the region where β is sensitive to change (ie, down to just a few unprotected acts at most). Thus, when every partnership involves 12 sex acts, a large increase in condom use is required to start to reduce prevalence.
However, when those with many sex partners only have two sex acts per partnership, a small change in condom use can have an effect. The situation is very different for a viral infection. Here, the transmission probability per partnership has not saturated and each incremental change in condom use alters the risk in the population, making the effect of increased condom use very similar to reductions in numbers of sexual partnerships. The heterogeneous infection is more like a bacterial infection: the transmission probability per partnership rapidly saturates for those infections where there is a high per act transmission probability. These are the important partnerships in terms of transmission and, as condom use in these partnerships increases, its effect accelerates. This is less important where many partnerships have a low number of sex acts (comparing pattern IV with pattern V).
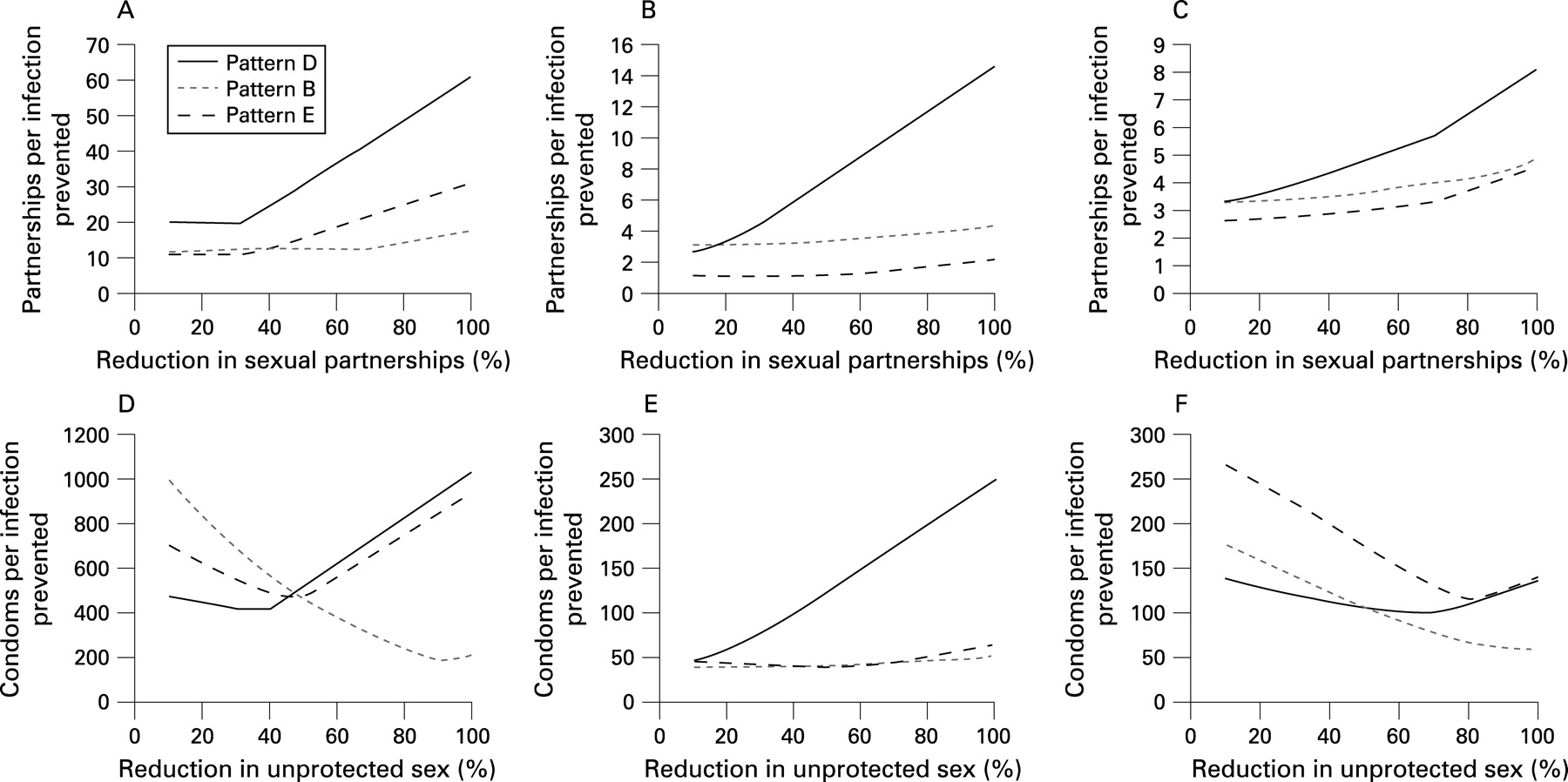
In considering the efficiency of interventions, we want to know how much effort is required to prevent a case of infection and this is illustrated in fig 3. Here the reduction in the number of partnerships or unprotected sex acts required to reduce the number of prevalent cases of infection by 1 is illustrated. The information in these figures is fully determined by the results presented in fig 2 so can be explained on that basis. Clearly, as there are many more sex acts than there are partnerships, the two work at different orders of magnitude. There is more scope to reduce the prevalence of infections that are more widespread so, generally, the greater the initial prevalence the smaller the behaviour change required to prevent each case of infection. Once infection has been eliminated, all further behaviour changes are wasted so the number of partnerships or sex acts generating the decline in infection numbers obviously increases. This is often the case for pattern IV where control of infection is facilitated by the small number of sex acts across all the partnerships of those with many partners (fig 3A–E). Before this point, in relation to increasing intervention size, an accelerating decline in prevalence decreases the incremental behavioural change needed whereas a decelerating decline in prevalence causes a decrease in efficiency, leading to an upward slope. When reducing partner numbers in all cases (fig 3A–C), efficacy remains relatively stable or decreases as each partnership removed contributes to preventing infections. This is also true for condom use in the case of virus infections (fig 3E) as each condom is contributing. However, for the bacterial and heterogeneous infections (fig 3D and F), efficiency can increase (ie, the number of condoms required per infection prevented decreases) because their impact improves as the number of unprotected acts in each partnership approaches zero.

{kind=link}
{kind=link}
{kind=link}
DISCUSSION
The predicted relationship between reductions in numbers of sexual partners or increased condom use and prevalence of infection has been explored in a selection of biological and behavioural scenarios representing the gross behaviour of different STIs. The complex relationships emerging preclude any simple or universal formula relating programme outcomes to an impact of infection numbers. Thus, in planning and evaluating interventions, the epidemiological context needs to be considered.
Despite this complexity, some general insights are possible. First, the impact (and therefore cost-effectiveness) of behaviour change interventions will depend on the prevalence of the STI in the absence of behaviour change. Second, for bacterial and heterogeneous-type infections, reducing the numbers of partners has a greater impact on prevalence than a similar proportionate increase in condom use within partnerships. For example, in behavioural scenario V (in which the number of sex acts is determined by the lower activity class partner) the prevalence of a bacterial infection is halved with a reduction in partnerships of about 20% or a 30% increase in condom use and, for a heterogeneous infection the prevalence is halved with a 30% reduction in partnerships and 60% increase in condom use (fig 2C and I). In contrast, for viral infections the effect of reduced partnerships and increased condom use is similar. Third, if transmission probabilities per act are high (typical of bacterial STIs), then condom use needs to be consistent across nearly all the sex acts within sex partnerships to be effective. If some sexual partnerships involve few sex acts, the use of condoms can protect these more readily. Fourth, if transmission probabilities are low (typical of viral STIs), then even inconsistent use of condoms can be beneficial unless the number of sex acts in the partnership is so great that the per partnership transmission probability also saturates here.
Our findings are similar to those of Pinkerton and colleagues who explored the impact of reducing partners and acts on an individual’s risk of acquiring infection and showed that partner numbers mattered more for bacterial than viral STIs.27 28 However, our analysis additionally shows that, for bacteria, when those with many partners only ever have few sex acts with those partners, then increasing condom use can be nearly as effective as reducing partner numbers (fig 2B). Furthermore, we show that a viral infection with a low average transmissibility per act can behave more like a bacterial STI, with condom use being less effective, if a fraction of infections have a higher transmissibility.
Because these general rules depend on the likelihood of transmission per sex act, it is important to understand what this is for each infection. Fortunately, we have a reasonable understanding of the average per act transmission probability for many STIs. However, it also matters whether this varies across partnerships as appears to be the case for HIV. A crude categorisation of the different infections would liken the bacterial STIs (gonorrhoea, syphilis and Chlamydia) to the bacterial STI represented here. In addition, human papilloma virus (HPV) appears to have a high transmission probability32 and so belongs in this category. The viral infections herpes simplex virus (HSV) and hepatitis B virus (HBV) are represented by the viral STI in our modelling exercise, whereas HIV (with its high transmission probability with high viral loads) would be represented by the heterogeneous infection. Our aim has been to apply a single generic model structure for all STIs. In fact, much of the heterogeneity in transmissibility of HIV appears to be due to the early stages of infection which lasts less than a year.33 This would accelerate the spread of an HIV epidemic, but our equilibrium analysis should be robust to this timing of high infectiousness.
The relationships uncovered by this analysis are not those expected from more simple theory and may not apply if infection is even more concentrated in a high-risk group (or groups) or, alternatively, has saturated across the entire population. In a homogeneous population we expect prevalence at steady state P to be related to the basic reproductive number, thus: P = 1 − 1/R0.18 Reductions in numbers of sex partners or decreases in the transmission probability per partnership reduce the basic reproductive number (R0). The relationship between prevalence and R0 is non-linear and, as R0 tends to 1, declines in steady state prevalence become increasingly steep. In a heterogeneous population the combination of prevalence declines in different risk groups can completely mask this shape because the proportion of overall prevalence represented by the higher risk groups increases as overall prevalence declines. However, previous analyses have shown that, as infection saturates in lower risk groups, reductions in partner change rates would be required to bring us to the starting point of this analysis where there is a rapid decline in prevalence with small changes in numbers of partners.17 (Note that the concept of the basic reproductive number is robust but, for a heterogeneous population, its mathematical formula is highly complex, as is its relationship to steady state prevalence.34)
Our analysis is further limited by our assumption that everyone in the population changes their behaviour equally. If particular individuals reduce their number of sex partners or number of unprotected sex acts then they reduce their risk of acquiring an STI——thus reducing the prevalence of infection—and they reduce their risk of transmitting infection if they do acquire it. Due to the combination of these two effects, the more widespread a reduction in risk behaviour, the greater its impact on prevalence.
Our analysis has separated out reductions in sexual partner numbers and numbers of sex acts and assumed that programmes can influence them independently. While we have shown that reducing numbers of partners and reducing numbers of unprotected sex acts can both be effective, in reality it may be more effective for programmes to include the range of risk reduction methods and tailor them to different groups within the population. Furthermore, in terms of efficiency, some behavioural change outcomes may be more readily achieved than others.
One of the motivations for this analysis is the debate about favouring abstinence and partner reduction programmes over condom use programmes. Consideration needs to be given not only to how sensitive modelled incidence or prevalence is to a particular mode of behaviour change, but also what size of change in that behaviour can be achieved in practice given the local context and available resources—in the case of HIV, whether increasing condom use or reducing numbers of partners will have the greater impact depends upon the magnitude of the behaviour change achievable (fig 2G–I).
In the examples we looked at reductions in numbers of partners but did not consider delays in sexual debut. Earlier analysis has shown that delaying sexual behaviour can reduce the prevalence of STIs but that its impact depends upon the compensatory changes in sexual behaviour at older ages as the sexual network is altered and that its impact is always relatively limited.35
The main purpose of this analysis has been to show how changing initial model parameters can alter the impact of interventions. Changing the model structure to better reflect the details of the biology of a particular infection may change the details of the model’s behaviour. One illustrative example used here was the inclusion of heterogeneity in transmission probabilities. Another would be the inclusion of acquired immunity to infection (eg, for chlamydia, syphilis or HPV). Such immunity would serve to lower the observed prevalence of infection and, for a given basic reproductive number, would make the infection harder to control as interventions would lower the prevalence of naturally acquired immunity.
Although the type of model used here is limited in its description of the network of sexual partnerships and the importance of partnership duration in determining patterns of concurrency and gaps between partnerships,36 37 it has provided many important insights into the epidemiology of STIs16–20 and enables us to focus on the relationship between changing sexual partner numbers, changing condom use and the incidence of STIs. However, the assumptions about the structure of the sexual partner network can also matter. For example, replacing short-lived commercial sex partners with concurrent casual partnerships could increase rather than decrease the spread of infection. A model that included a more complete description of the sexual contact network might also find that small changes in risk could prevent infection from entering parts of the network, bringing about dramatic reductions in prevalence. Despite the potential impact of more detailed network structure, the principles generating our results (ie, that reducing numbers of partnerships for those at risk always reduces the potential for spread whereas the effect of using condoms will depend on the number of unprotected sex acts and the transmission probability in those acts) should hold as models increase in detail and complexity.
Key messages
For STIs with a low transmission probabiliy per sex act, the incidence of infection responds similarly to changes in partner numbers and numbers of unprotected sex acts. High transmission probabilities alter the relationships, with the effectiveness of increasing condom use improving as the background number of unprotected sex acts decreases.
There is no simple and general rule that will allow the effectiveness of interventions to be calculated.
Heterogeneity in transmission probability across infections, which may occur for both bacterial and viral infections, can reduce the effectiveness of condom use as an intervention if that use is inconsistent.
Another simplification is our assumed symmetry in the modelled behaviour and biology of men and women. The potential higher transmissibility from men to women than vice versa would make condoms less effective when the man is infectious compared with the case when the woman is infectious. In addition, in many populations a large fraction of men have many partners and a smaller fraction of women have an extremely high number of partners.38 This is often associated with sex work and, in such cases, it is likely that there are few acts in commercial interactions which would increase the potential impact of condom use.
Unfortunately, policy makers demand decisive, simple and robust insights and there is a danger that advocates (of all intervention approaches) claim greater certainty than is warranted. However, to provide the necessary evidence we need more theoretical and empirical work in the area of this analysis—first to challenge and potentially modify the illustrative insights offered through our analysis and, second, to provide more rigorous evidence of which programmes have an impact in the field. Both randomised controlled trials and observational studies are needed with infection end points as well as self-reported behaviours, given the potential frailty of behavioural measures to social desirability bias and the complexity of the relationship between changes in individual behaviour and transmission of infection at the population level.
REFERENCES
Footnotes
Competing interests: None.
Roles: All the authors conceived the study and wrote the manuscript; GPG coded and analysed the model.