Article Text

Abstract
Objectives: To describe the concepts, strategies and field results of a project to scale up prevention programmes and services for female sex workers (FSWs) in Karnataka, India.
Methods: A strategy was developed to scale up urban sex worker interventions in 18 districts in the southern Indian state of Karnataka. Macro-level coverage objectives were defined by mapping the urban locations where FSWs operate and estimating their population size. Prevention programmes were initiated in the urban locations that contained at least 90% of the estimated urban FSW population in each district. Within each location, a micro-planning process was used by FSW peer educators and outreach workers to design local outreach and service delivery plans.
Results: An estimated 48 973 FSWs were distributed across 1551 locations and 6232 spots. Outreach was conducted by 1043 peer educators. Services were provided through 170 drop-in centres, 93 programme-run clinics, 110 outreach clinics and 157 referral clinics. Within the first 3 years of the programme the cumulative number of individual FSWs contacted at least once was >78 000, with monthly contact established with 81% of the in situ population; >45 000 FSWs had visited a clinic and >10 000 visited monthly. Direct and indirect condom distribution by the programme amounted to more than 30 per contacted FSW, which is estimated to meet the condom requirement.
Conclusions: A strategy that involves geographically defined coverage and micro-level outreach planning can rapidly and effectively provide outreach and services to large dispersed FSW populations.
Statistics from Altmetric.com
HIV prevention in the context of female sex work has been identified as a top strategic priority in many global regions.1–3 Data from Asia indicate that commercial sex networks are the single most important feature of the sexual structure that determines the trajectory and size of HIV epidemics.4 5 Mathematical models based on Asian sexual structures indicate that scaling up prevention in female sex work to substantially increase condom use is likely to have a dramatic impact on the overall HIV prevalence in those settings.6 The effectiveness of the mass campaigns in Thailand and Cambodia to increase condom use in commercial sex encounters is widely credited with reversing the HIV epidemics in those countries.7
Much has been written about the design of HIV prevention programmes in female sex work.8 9 Most of the focus of previous literature has been on success factors in the context of an individual programme focused on a particular FSW setting, and many of these examples are of limited scale. An exceptional example is the 100% condom campaign in Thailand, which was a structural intervention in the context of a particular sex work organisational context that was dominated by somewhat formal brothel structures.7 In contrast, much of the sex work in Asia is dispersed and unstructured with highly diverse organisational characteristics. Such dispersion and diversity poses substantial challenges to scaling up targeted prevention programmes. For example, most sex work in South India is street-based and relatively unstructured in its organisation. Even in locales where sex work was historically concentrated in large brothels such as Mumbai, an increasing proportion of sex work is being dispersed into less formal settings. Extending HIV prevention programmes and services to female sex workers (FSWs) in such settings requires the effective identification and characterisation of sex work locations and distributing programme resources and activities accordingly.
In this paper we illustrate concepts and strategies used to scale up targeted prevention programmes for FSWs in the state of Karnataka in south India.
Project overview and setting
The project described in this paper is called Sankalp (the Sanskrit word for “determination”), which is funded by the Bill & Melinda Gates Foundation as part of Avahan, its India AIDS Initiative. The broad context of the Avahan project and its overall scale has been previously described.10 This paper examines the approach taken by our team in the state of Karnataka. Management and implementation of the project is a joint initiative of the University of Manitoba and the Karnataka Health Promotion Trust, an Indian non-governmental organisation (NGO) established in 2003. The key objective of the Sankalp project is to scale up prevention programmes and services for FSWs and high-risk men who have sex with men (MSM) in Karnataka. Beginning in early 2004, the project initially focused on 16 of the 27 districts of Karnataka and subsequently expanded to cover 18 districts over the ensuing 3 years. Thirteen of the 18 districts are in central and northern Karnataka, with the remaining 5 districts comprising the capital city of Bangalore and 4 nearby districts in southern Karnataka. The overall population of the 18 districts is approximately 45 million (approximately 17 million in urban areas), with the district populations ranging from 1 to 6.5 million (Bangalore city). These districts were selected in consultation with the Karnataka State AIDS Prevention Society primarily on the basis of perceived need: (1) most of the districts had either no or minimal existing prevention programs for FSWs or MSM; (2) the perceived size of the FSW population in these districts was higher than the remaining districts; and (3) the HIV prevalence in antenatal clinic sentinel surveillance sites (2003) was substantially higher in the selected districts (1.5%) than in the remaining districts (1.1%). The predominant focus of the project, and the subject of this paper, is on FSWs working in urban areas. Prior to the Sankalp project, only 7 of these districts had any prevention programme for FSWs and, in those districts, coverage was estimated to be low.
METHODS
Conceptual approach
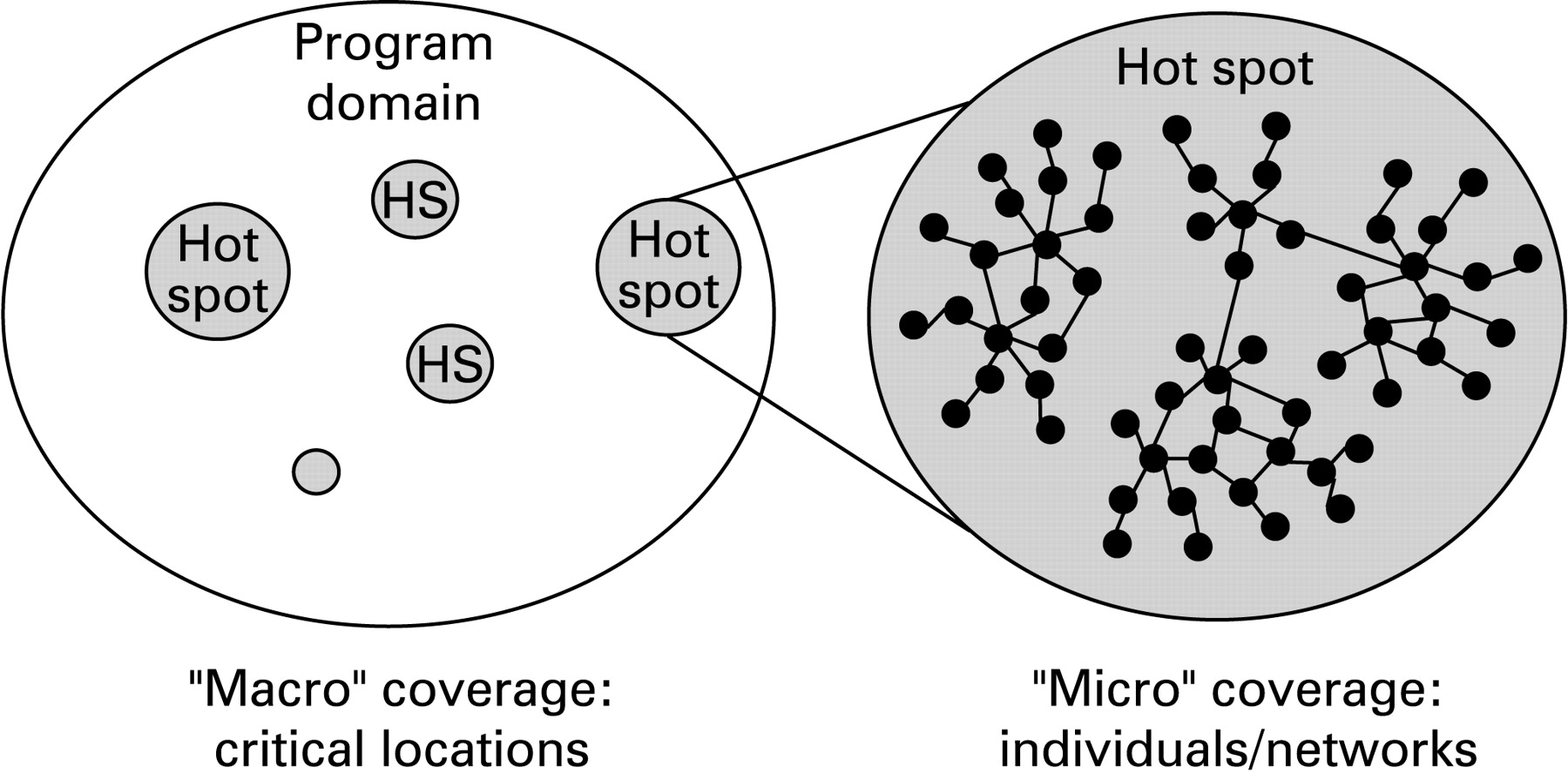
Conceptually, the basic metric for scaling up prevention programmes is “coverage”, which can be simply defined as the proportion of the target population that receives a defined set of programmes and services. Crucial to this concept is the determination of denominators which specify the size of the target population. Programmatically, achieving high coverage depends on two levels of strategic planning and implementation. The first level of planning focuses on situating programmes and services in the geographical/administrative regions that contain a high proportion of the target population (“hot spots”). This macro-level planning determines the upper limit of coverage since the geographical/administrative regions where no programmes and services are provided have essentially nil coverage of the target population. The second level of planning occurs within the locations where programmes and services are situated and relates to the proportion of individuals within each location that are reached by the programmes and services. This micro-level planning and programme achievement sets the upper limit of coverage within each location. The overall coverage is then a composite of macro- and micro-level coverage (fig 1). Based on this conceptual framework, our strategy for scaling up involved the following key steps:

comprehensive mapping to determine the size and distribution of key populations;
macro-level establishment of programmes and services in those urban locations that contained at least 90% of the estimated key population;
micro-level planning and implementation of outreach and service delivery to cover a high proportion of the key population individuals within each location.
The methods for implementing this strategy are described below.
Mapping methodology
Mapping was conducted in all 210 census-designated cities and towns (typically with a population of at least 15 000) in Karnataka, although this paper focuses on the results of mapping in 156 towns and cities (including Bangalore) in the 18 project districts. Excluding Bangalore, most cities had populations of <50 000, with only 20 cities having a population >100 000 and <500 000 and one city with a population of approximately 750 000. Our mapping methodology was based largely on the understanding that most FSWs in south India, particularly those who are most active, congregate and/or meet clients in definable geographical locations. Accordingly, our approach was to focus on identifying these locations, characterising each location in terms of specific “spots” within that location and the operational characteristics of sex work there (ie, how and where FSWs meet clients and where transactions occur), and estimating the number of FSWs that frequent the location and spots. This approach is an adaptation of the PLACE (priorities for local AIDS control efforts) methodology described by Weir and colleagues11 which identified locations where individuals frequented to acquire new sexual partners. We incorporated two levels of data collection and analysis. Level 1 involved a systematic process of interviewing secondary and tertiary key informants (including pimps, taxi and rickshaw drivers, police officers and NGO workers) to identify locations where FSWs can be found, with a focus on locations where they meet clients. Typically, 40–75 key informant interviews were conducted in each town or city, depending on the size. Since the capital city of Bangalore is so large (population 6.5 million), it was segmented into 49 zones and the level 1 data were collected separately in each zone. The locations were tabulated on a daily basis and all those mentioned by multiple key informants and/or those where a key informant indicated that a large population of FSWs could be found were identified for a second level of data collection which occurred at the location with primary key informants (FSWs at the locations). Level 2 interviews sought detailed information about the specific spots within a location, the number of FSWs who worked at a particular location or spot on a typical day, and the general organisational typology of sex work at that location (eg, street-based, brothel-based, home-based). For example, a large train station would be considered a location, but it may have several distinct spots where FSWs can be found (eg, front gate, platform). Level 2 interviews also sought to identify other locations in the vicinity not identified by level 1 key informants. This process of “snowballing” proceeded until location identification became redundant and no new locations were identified. Data collection was conducted and supervised by a team of 170, including members of key populations (FSWs and MSM). Overall, across all 27 districts a total of approximately 76 700 key informant interviews were conducted.
Macro-level programming
Mapping results were used for macro-level planning with the objective of ensuring that outreach programmes and basic services were quickly established in cities and locations that contained at least 90% of the estimated FSWs in each of the project districts. Interventions in 14 of the 18 districts were contracted to NGO partners, with the remaining 4 district programmes being implemented directly by the University of Manitoba and Karnataka Health Promotion Trust. In each district an initial intervention team consisting of outreach workers, field supervisors and a small number of FSW peer educators was established to initiate outreach and to establish basic clinical services. “Drop-in centres” were to be established where there were large population concentrations of FSWs (at least 250).
Micro-level programming
Once basic programme teams were established, micro-level planning was conducted for each identified FSW location within each town/city. This planning was done primarily by local peer educators from the location, with the support of NGO project staff (outreach workers and field coordinators). The micro-planning entailed three activities:
Peer-led mapping: local FSW peer educators systematically validate and define the local spots and logical geographical boundaries of sex work within that area.
Spot profiling: describing the organisational and operational configuration of sex work in each location, including where clients are encountered, where sexual transactions take place, the size of the FSW population, the turnover rate, the timing of sex work (ie, time of day, days in the week), age distribution of FSWs and the usual client volume.
Peer social network analysis: for each location the peer educators make a list of all the FSWs that they know personally, and then lists are compared and decisions taken about which peer educator will take responsibility for outreach to each individual FSW.
These activities rely primarily on visual aids for planning since most peer educators are illiterate. In addition to planning outreach per se, micro-planning includes identifying optimal locations for drop-in centres and programme-run clinics where there are large concentrations of FSWs, or outreach and referral clinics when FSWs are more dispersed. Condom distribution is planned through direct methods (ie, peer educators directly supplying condoms to FSWs) or indirect methods. Indirect condom distribution is primarily through strategically placed condom “depots”, which can either be via local non-FSW individuals such as petty shop owners or through “condom boxes” which contain free supplies of condoms that are regularly checked and refilled. Peer educators and outreach workers track the number of condoms distributed directly to FSWs and through indirect channels (condom depots) for each location and compare this with the estimated need based on the number of FSWs and their client volume.
Measuring and monitoring achievement
We established a field-based monitoring system using a framework that is congruent with basic outreach and service delivery objectives of the project. The system is based on tracking the outreach and service delivery to individual FSWs by their peer educators. Outreach activities to individual FSWs are tracked by peer educators and outreach workers using simple field tools, including “peer outreach cards” on which each individual field contact is logged, and peer monthly calendars in which peer educators and outreach workers track services provided to each FSW on a peer educator’s roster. The key programme and service delivery indicators tracked by this system include:
Contacted at least once: indicates which FSWs have been contacted by a peer educator at least once.
Regular contact: indicates which FSWs have been regularly contacted by programme outreach staff, defined as contact at least twice a month.
Ever visited the clinic: indicates which FSWs have ever visited a project clinic.
Clinic visit in past month: indicates which FSWs have visited the clinic within the past 1 month.
Condom gap: the gap between the number of condoms distributed directly and indirectly and the estimated requirement based on the number of FSWs and the client volume.
A central concept of this framework is the use of systems by which peer educators can continuously assess “opportunity gaps”, which are defined by the number of individual FSWs who have not received key outreach and service delivery programme components. By tracking outreach and service provision on an individual basis, peer educators plan their daily and weekly activities to focus on those who have not received services and thereby minimise the “opportunity gaps” within their own roster. At a higher level, field coordinators and programme managers use aggregate data on outreach and service gaps from each location, town and district to optimise programme tactics and service configurations. Data from peer outreach cards and clinic records are entered into a standardised management information system (MIS) database in each district. Data from the MIS system are then analysed by a central monitoring and evaluation team.
RESULTS
Mapping and macro-level implementation
In the 18 project districts the initial urban mapping exercise estimated that there were 48 973 FSWs distributed across 1551 locations and 6232 spots. Overall, there is an estimated average of 13 FSWs per 1000 adult men in urban areas of these districts (range 5–21 per 1000 men). Almost half (24 222) of the estimated FSWs were in the capital city of Bangalore. In each of the remaining districts the top three towns/cities generally contained 45–50% of all the estimated urban FSWs but, to achieve a macro-level target of 90% coverage of urban FSWs, it was determined that programmes and services were required in 178 cities and towns reaching approximately 2500 spots within those urban areas.
Accordingly, outreach teams and services were rapidly deployed to these 178 cities and towns and within 20 months the following project infrastructure was established:
170 drop-in centres, 93 programme-run clinics, 110 outreach clinics, 157 referral clinics.
1043 peer educators, 490 full-time outreach workers, 74 project doctors and 102 other clinic staff (primarily nurses), 232 management, field coordination, technical and administrative staff.
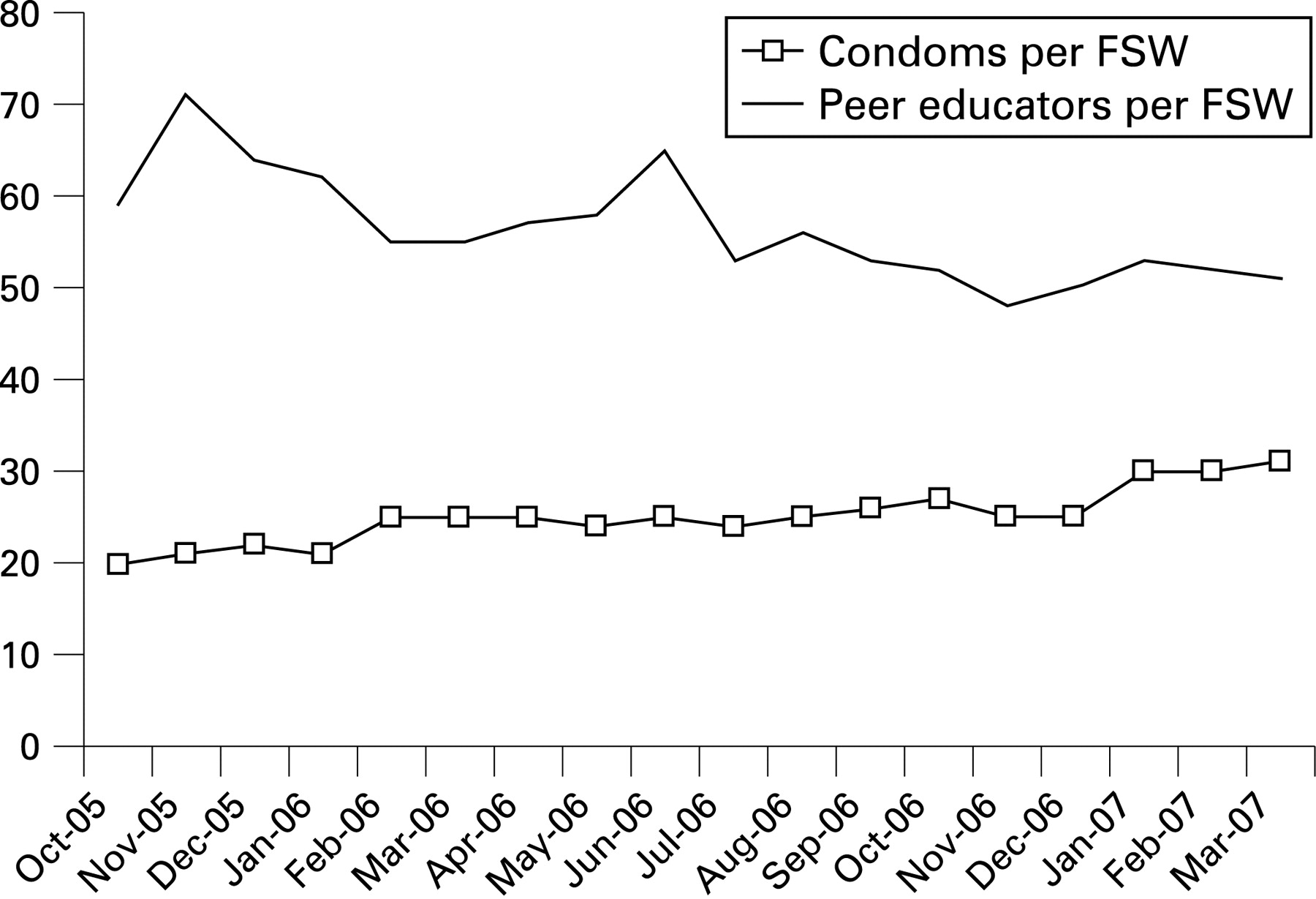
One key metric of programme implementation is the peer educator to FSW ratio, with an objective of having at least 1 peer educator for every 50 FSWs. Figure 2 shows the trend in peer educator ratio across all districts between October 2005 and March 2007, during which time it reduced from over 60 to approximately 50. Spikes in the ratio occurred in November 2005 and June 2006 when programmes expanded into new zones of Bangalore.
Micro-level planning and programme coverage
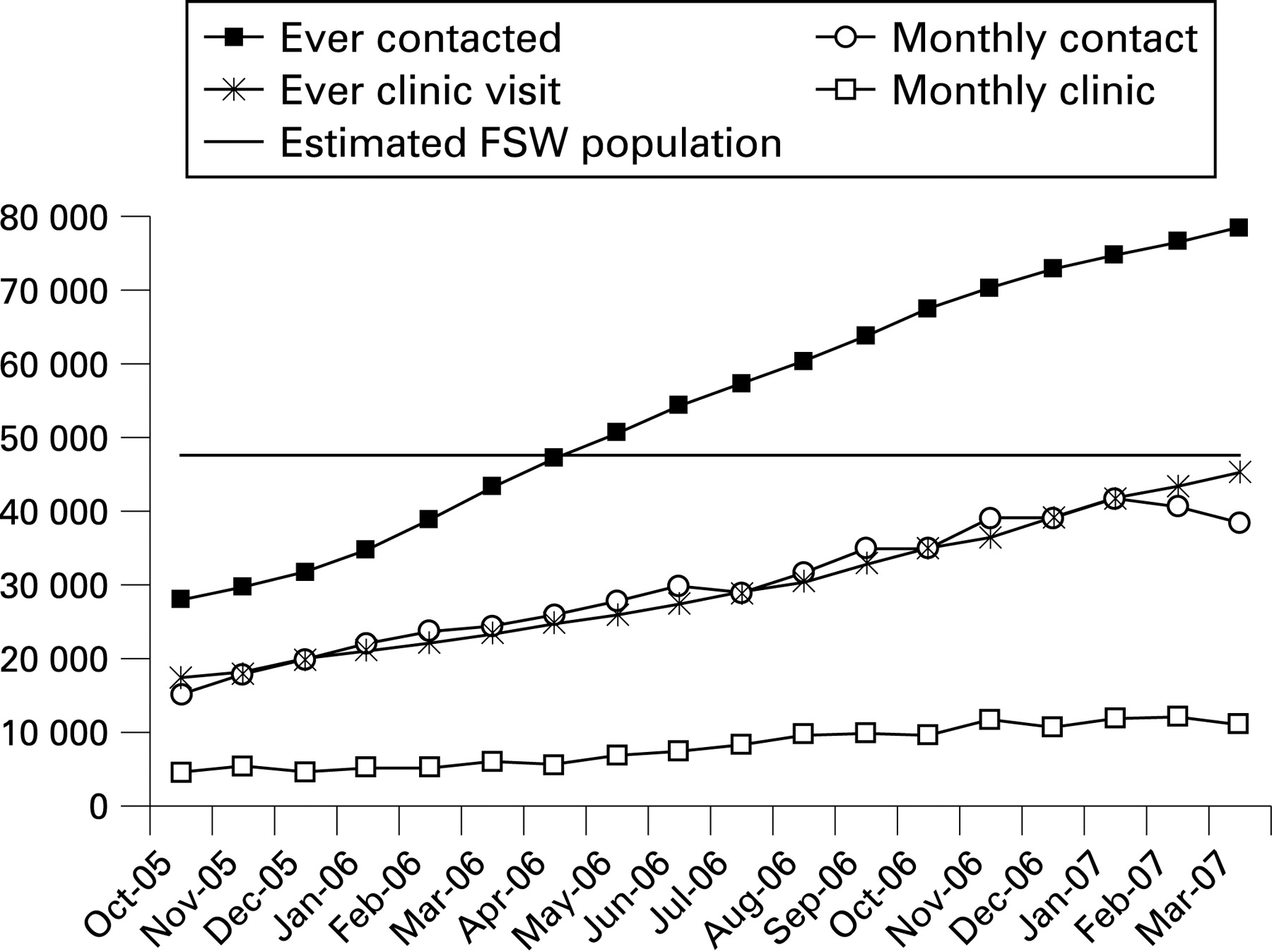
Micro-level planning was conducted at all locations for all spots in each of the 178 towns and cities. At each location a specific outreach plan was developed whereby each peer educator had a specified list of FSWs for whom she was responsible for outreach, education and monitoring. Figure 3 illustrates a composite of the key outreach and service delivery achievements across all districts between October 2005 and March 2007. During that time period the estimated average number of FSWs at all locations was 47 466. By October 2005 a total of 27 801 FSWs had ever been contacted by a peer educator or other outreach worker. Most of those had been contacted in earlier time periods in non-Bangalore city districts since Bangalore urban outreach was initiated in phases during late 2004 and throughout 2005. Over the ensuing 18 months the cumulative number of different FSWs ever contacted through outreach rose steadily to almost 80 000, which is substantially higher than the estimated number of FSWs present at any given time. Since this figure includes all FSWs who have worked at those sites, it indicates a relatively high level of turnover of FSWs. Turnover is due to both the presence of FSWs who only work occasionally in a given location and the natural influx of new FSWs to replace those that move out or stop sex work altogether. Over time, there has also been a steady rise in the number of different FSWs who have been contacted within that month, which is a measure of the regularity of contact through outreach. The proportion of FSWs having been contacted within the month increased from 32% in October 2005 to 81% in March 2007. There was a steady increase in the proportion of FSWs who had ever visited a project clinic, from 37% to 95%. The proportion who had visited the clinic in the previous month increased from just under 10% to 23%.

{kind=link}
{kind=link}
{kind=link}
Condom distribution increased over time and, by March 2007, had reached a level of more than 30 condoms per contacted FSW per month. Since the average monthly client volume per FSW is just over 25, there is no apparent gap in condom availability.
DISCUSSION
In presenting our particular approach to scaling up targeted prevention programmes, we recognise that strategies need to be context-specific. The success of the 100% condom campaign in Thailand was based largely on a society-wide structural intervention that focused on changing the norms in sex work through public education, legal enforcement and policy decisions by sex work establishments.7 A structural intervention in the brothels of Sonagachi in Kolkota, India has been successful at maintaining high rates of condom use by empowering the community to reduce their risk and vulnerability through solidarity and mutual support.12 Both of these successful projects occurred in a sex work context that is highly concentrated into organised settings. In contrast, sex work in the context of our project is highly dispersed geographically with more than 50% of the FSWs working in public places. Few of the FSWs belong to a structured sex work organisational structure through which programmes and services can be delivered efficiently. Our model for scaling up is most relevant for such settings.
Although mapping of sex work locations and size estimation has been conducted in preparation for programme delivery in many settings, little has been published on the methodology and results. Kruse and colleagues describe a study that mapped sex access points for FSWs in Diego-Suarez, Madagascar and supplemented this with a capture-recapture approach to estimating the size of the FSW population.13 Family Health International has reported on a broad-based mapping study in the Indian state of Maharashtra that had similarities to our approach in that it focused on identifying commercial sex access points.14 To our knowledge, our mapping is distinguished from most others in terms of the scale, detail and rapidity of implementation. Moreover, we used standardised methods for identifying and interviewing key informants and collating and triangulating their information. We also conducted detailed spot-by-spot validation for those locations identified by key informants with the participation of local FSWs in the data collection process. However, our subsequent experience in programme implementation has revealed some important shortcomings in this mapping methodology. Most importantly, our mapping did not identify certain sex work pockets, particularly a type of small mobile brothel-type sex work that is prevalent in some of the larger cities. The mapping also missed some low-volume home-based sex work settings. Despite these shortcomings, we believe that this rapid geographically-based mapping is essential and adequate for prioritising and establishing initial outreach and service delivery points. However, once established, local teams need diligently to pursue information on other sex work locations and networks in their vicinities.
Our basic approach to peer outreach is not unique,12 15 16 but we believe that the implementation of detailed micro-planning processes and outreach programmes on this scale is uncommon. A key advantage of our approach is the high level of engagement of peer educators in the planning and monitoring of field-level programming. By providing peer educators with the skills and tools to plan outreach and services, their unique understanding of the local situation can be harnessed to optimise field strategies. By providing peer educators with a system of monitoring that they can manage, it builds a sense of ownership and achievement among them.
Key messages
A strategy was developed to scale up urban female sex worker (FSW) interventions in 18 districts in the southern Indian state of Karnataka.
Macro-level coverage objectives were defined by mapping the urban locations where FSWs operate and estimating their population size. Prevention programmes were initiated in the urban locations that contained at least 90% of the estimated urban FSW population in each district.
Within each location, a micro-planning process was used by FSW peer educators and outreach workers to design local outreach and service delivery plans.
Within the first 3 years of the programme the cumulative number of individual FSWs contacted at least once was >78 000, with monthly contact established with 81% of the in situ population; >45 000 FSWs had visited a clinic and >10 000 visited monthly.
Direct and indirect condom distribution by the programme amounted to more than 30 per contacted FSW, which is estimated to meet the condom requirement.
A strategy that involves geographically defined coverage and micro-level outreach planning can rapidly and effectively provide outreach and services to large dispersed FSW populations.
We found that an organised training and capacity building programme to support this activity is crucial for success. We developed a detailed training guide, organised a “trainer of trainer” programme and devoted substantial management resources to oversee the initial activities in each district. While the initial planning process was well understood and well implemented in most districts, we have found that a high turnover of peer educators and outreach staff can have a rapidly deleterious effect on the outreach and monitoring processes. Individual-level tracking is difficult to maintain when peer educators change, so a strong supportive structure of full-time outreach staff is required to sustain continuity. Over time, several of the district programmes have been successful in promoting senior peer educators into full-time outreach worker roles, but this requires additional capacity building inputs. Although our monitoring system tracks many indicators not described in this paper, we have found that early in the scaling up process it is important to emphasise and focus on a small number of key indicators that bear on the functioning of key aspects of the programme—specifically, outreach, service delivery and condom distribution. As additional programme elements are integrated—including structural interventions to reduce vulnerability and improve social cohesion—other monitoring tools and indicators can be added. Although we have not described them in this paper, we have also instituted periodic surveys to monitor changes in behaviour and the prevalence of HIV and sexually transmitted infections. The availability of a detailed information base on the distribution, size and characteristics of FSW populations greatly facilitates sampling and field implementation of those surveys.
As the global effort proceeds to close the “prevention gap”, particularly for the most vulnerable populations, programmes need to move beyond “best practices” to focus on sufficient scale and coverage. Doing this without sacrificing quality and effectiveness is a key challenge. This will require attention to both the macro-level planning processes, but also to ensuring that micro-level planning and implementation is strong. Systems such as the ones we have described in this paper need to be developed, adapted, improved and documented. In addition, organised mechanisms for training and capacity building in processes for scaling up need to be developed and supported so that innovations can be more rapidly disseminated and adopted.
Acknowledgments
The authors acknowledge and thank partners in programme implementation, including Swasti, Myrada, Samraksha, the Belgaum Integrated Rural Development Society, Action Aid, Suraksha and the Chaitanya AIDS Prevention Society.
REFERENCES
Footnotes
JFB was the overall project coordinator and lead author of the study. PB and SK were primarily responsible for developing and describing micro-planning tools and methods. BMR, PB, SK, NSK, RW and SM provided data interpretation and manuscript review and revision.
Funding: The project was funded by the Bill & Melinda Gates Foundation through Avahan, the India AIDS Initiative. The views expressed herein are those of the authors and do not necessarily reflect the official policy or position of the Bill & Melinda Gates Foundation and Avahan. JFB is supported by the Canada Research Chair in Epidemiology and Global Public Health.
Competing interests: None.