Article Text

Abstract
Background Sexually transmitted infections (STI) are a significant public health problem both worldwide and in Europe. This article reviews trends in the epidemiology of the major bacterial STI in eastern European countries, their key determinants, as well as challenges and opportunities for enhancing STI control in the region.
Search strategy Publications were sought through computerised searches in PubMed from 1995 to 2008 using using free text and relevant medical subject headings with no language restrictions. Conference abstracts and other unpublished manuscripts were excluded.
Results The reported rates of STI in many eastern European countries have either decreased (syphilis and gonorrhoea in the eastern/Russian regions, gonorrhoea throughout eastern Europe) or been relatively stable (syphilis in the southeastern region, chlamydia throughout eastern Europe), in the past decade, but are still significantly higher than in western Europe. There is a significant east–west geopolitical gradient in reported STI rates throughout eastern Europe (STI rates: Russia/eastern region>>southeastern region>central region). Challenges for STI control include: the need to strengthen public health components of control; improvements in surveillance and improvement, as well as quality assurance, in diagnostic strategies. Gains in STI control may be achieved through greater collaboration and harmonisation of practicss at the European level.
- Chlamydia trachomatis
- eastern Europe
- epidemiology
- gonorrhoea
- sexually transmitted infection
- syphilis
Statistics from Altmetric.com
Sexually transmitted infections (STI) are a significant public health problem worldwide and also in Europe, causing substantial morbidity and mortality. They disproportionately affect women, marginalised communities and those with high-risk sexual lifestyles, and these factors make STI an important focus for European public health policy.1 Since the early 1990s, the countries of eastern Europe have experienced extraordinary shifts from communist regimes towards market economies and democracy. In several countries, the profound political, socioeconomic and cultural changes have been associated with epidemics of HIV and STI,2–4 decreases in health and life expectancy and the growth of informal economies, including the drug and sex trades.5
Although the term ‘eastern Europe’ was defined during the Cold War, it is still used to describe the geopolitical region encompassing the easternmost part of the European continent. The region is often further divided6 into: (1) central (Czech republic, Hungary, Poland, Slovakia, Slovenia); (2) eastern (Belarus, Estonia, Latvia, Lithuania, Moldova, Ukraine); (3) southeastern (Albania, Bulgaria, Bosnia and Herzegovina, Croatia, Kosovo, Republic of Macedonia, Romania, Montenegro, Serbia) and (4) Russia, which is defined as a transcontinental country. Although there is no general agreement on these subdivisions, they are convenient for the purposes of this review (figure 1).

The countries of Eastern Europe. Source: The World Factbook.6
In this article we review epidemiological trends in the major bacterial STI in eastern Europe, their key determinants, as well as challenges and opportunities for enhancing STI control in the region.
Search strategy
We reviewed the published literature and surveillance reports on the distribution of STI in eastern Europe to describe recent trends in the epidemiology of bacterial STI in the region. Since both medical and public health systems underwent dramatic changes from 1990 to 1995 there are concerns about the adequacy of reporting STI during this period. The current review thus focuses on the period after 1995, following the development of significant harmonisation across health systems with regard to STI reporting. Relevant publications were sought through computerised searches in PubMed from 1995 to 2008 using free text and the following medical subject (MeSH) headings: sexually transmitted diseases, bacterial, syphilis, gonorrhoea, chlamydial infection, Europe, eastern plus names of the 20 eastern European countries from the MeSH descriptor list. There were no language restrictions. We also obtained data from personal communications with physicians and epidemiologists from the region. Conference abstracts and other unpublished manuscripts were excluded because they did not provide sufficiently detailed information. When available, we analysed surveillance data for gonorrhoea, syphilis and genital chlamydial infection for the eastern European countries.
We also reviewed the main components of population change (fertility, mortality and international migration). Statistical data and measures were derived from major international sources (Eurostat, UN Population Divsion, UN ECE, World Bank).
Results
Regional description: eastern Europe—changing demography and implications for STI transmission
Eastern Europe comprises 20 countries that vary greatly in geographical area and population. The smallest in population terms is Montenegro, with 608 000 inhabitants, followed by Estonia and Slovenia, each with less than two million inhabitants. On the other hand, the Russian Federation stretches from Europe to Asia and has 144 million inhabitants. Other countries with relatively large populations include Ukraine (46 million), Poland (38 million) and Romania (21 million). Together, these four countries account for three-quarters of the region's population, totalling 330 million.
Following the demise of state socialist regimes at the turn of the 1990s, eastern Europe has been undergoing a turbulent period of interlinked political, economic and demographic change. Before the onset of societal transition, the region experienced positive population growth. However, during the past 15 years, population growth has declined in most countries, with moderately positive growth rates sustained only in the southeastern region.7 In the first half of the 2000s, half of the countries experienced depopulation of approximately −0.5% per year. This is in contrast to the moderate population growth in the western part of the continent, represented by the European countries that first joined the European Union (the EU-15) in table 1 and web appendix.
A key factor responsible for the depopulation in eastern Europe is the abrupt fall in birth rates. From levels near replacement (2.1 children per woman), fertility rates declined to a region-wide total fertility rate (TFR) of only 1.29 in 2000–5. In 12 countries, the TFR dropped below 1.3, a level considered to be the limit of ‘lowest-low’ fertility,8 whereas 15 countries had a TFR below the EU-15 average. The decline in fertility rates has steeply accelerated the rate of demographic ageing, placing an increasing strain on social protection systems.9
Key demographic and socioeconomic indicators for east European countries
The decline in fertility reflects a profound change in reproductive behaviour. Before the onset of societal change, early age at childbearing was a distinctive feature of the east European reproductive pattern, and women typically had their first child at the age of 22–23 years. Subsequently, the ‘ageing of fertility’ has gained strong momentum in the region. The difference between conventional and tempo-adjusted TFR reveals that in several countries (eg, Bulgaria, the Czech Republic, Estonia, Hungary, Romania) delayed childbearing has made a major contribution to the observed decline of period fertility rates.10
The region has also witnessed a considerable rise in the proportion of children born out of wedlock, reaching an average of 27% in 2005. In Bulgaria, Estonia, Latvia and Slovenia the proportion is above 40%, whereas in the Czech Republic, Hungary, Lithuania, Romania, the Russian Federation and Slovakia it is over 25%. The weakening connection between childbearing and marriage has resulted from a decline in marriage rates and the increasing popularity of consensual unions.11 The demographic trends towards later parenthood, declining marriage rates and less formal and more fragile unions, coupled with a decrease in the age of first sexual activity,12 have implications for sexual and reproductive health as they increase the likelihood of having multiple sexual partners, an important determinant of STI transmission.
The fall of the Iron Curtain quickly removed obstacles that limited the movement of people across borders and gave rise to new migratory patterns, both permanent and temporary, between east and west and within eastern Europe.13 In some countries, ethnically based migrations were common, including the return of individuals to their motherland. Civil conflicts also led to large flows of asylum seekers.14 In 2000–5, half the countries in the region experienced negative net migration while the other half reported a positive balance of migration flows. The increase in international mobility may increase the challenges for sexual health as it has significantly expanded the scope of contacts with foreigners, including those from high STI/HIV prevalence countries.15
Mortality in eastern Europe remains higher than in the EU-15, particularly for men. At the same time, there is a noticeable diversity within the region (table 1, web appendix). The period following 1970–80 was generally one of stagnation when life expectancy ceased to rise in the region, and declined in several countries, particularly for men.16 However, towards the end of state socialism, life expectancy rose in the Czech Republic, Hungary, Poland, Slovakia and Slovenia, and these countries have now closed part of the gap with older EU member states.17 However, in Belarus, the Russian Federation, Moldova and Ukraine, recovery from the rise in mortality of the early 1990s is still incomplete, and life expectancy remains below the levels observed at the eve of transition.18 These patterns also mirror the general state of public health systems, which clearly play a role in controlling the spread of STI.
Varying conditions at the time of social change and the varying speed of reform resulted in wide socioeconomic differences, but challenges remain. In general, the populations of the new EU states are enjoying higher levels of gross domestic product than other countries in the region, but economic growth has not necessarily translated into enhanced social cohesion. As a consequence, high income inequality and the risk of social exclusion are encountered in many countries. With persistent weaknesses in social ‘safety nets’, these circumstances may increase the risk of behaviours and lifestyles (such as drug abuse and sex work) that are conducive to the transmission of STI.
Infrastructure for STI diagnosis, treatment and surveillance
In eastern Europe the case management of STI is based on laboratory and individual clinical diagnosis.19 20 A survey conducted in the early 2000s to assess the adequacy of STI prevention and control policies and programmes in Europe documented almost universal provision of STI care through dermatovenereology or dermatology clinics in eastern Europe.19 Although this represents the traditional mode of delivery of STI care in these countries, some new developments warrant attention. In particular, a significant proportion of clients will not attend licensed public services because they perceive them as not user-friendly or lacking confidentiality. Instead, many prefer to attend private providers or self-medicate.21 Data on the proportion of care delivered in private practice by country or region are unavailable. In addition, a significant proportion of STI care is now provided by non-specialists.22 23 This is demonstrated by a study from Estonia, which showed that the majority of outpatient STI care and/or prescriptions in 2004 were prescribed either by gynaecologists (60%) or by dermatovenereologists (30%), with general practitioners providing less than 10% of STI care. The locus of care differed by STI: 90% of syphilis treatment was provided by dermatovenereologists, whereas almost two-thirds of patients with Chlamydia trachomatis or trichomoniasis were treated by gynaecologists.22
The provision of previously free services has been severely eroded. STI consultations, Gram staining and syphilis serology are free of charge, at least in principle, in almost all east European countries. However, in most countries, patients must pay for treatment or purchase drugs.19 21
According to an assessment of diagnostic capacity and clinical practice conducted in the early 2000s, STI management in the eastern region countries was suboptimal and adherence to evidence-based guidelines was low. The need for quality assurance of diagnostic strategies, testing and assays used in many east European countries was recognised.24 Comparable information on the other east European regions is not available. However, chlamydia testing is not routinely available in most countries.19 25As a result, data on genital chlamydia occurrence are limited. The most commonly used diagnostic test for C trachomatis is direct immunofluorescence25 26; however, in recent years nucleic acid amplification testing has been more widely implemented.
The mainstay of east European surveillance systems for bacterial STI is clinician case reporting (M Skerlev, personal communication, 2009).19 20 27 Universal physician case reporting is mandatory for gonorrhoea and syphilis in all countries and for chlamydia in some.19 Reporting is mandatory for all healthcare providers irrespective of their role (STI specialist, non-specialist) or funding (private/state-funded care). By law, new cases of laboratory-confirmed infection must be reported by treating/diagnosing physicians to health departments. Sentinel reporting or laboratory-based reporting to monitor disease trends are not routine, but results of pilot projects have been published.28 Surveillance data on adverse health outcomes of STI, such as ectopic pregnancy or pelvic inflammatory disease, are unavailable.
It is extremely difficult to determine STI prevalences accurately in different transmission groups (eg, homo vs heterosexual) in eastern Europe for various reasons.29 First, only a limited number of countries collect this information. Second, non-disclosure of sexual orientation remains common in eastern Europe.29 A recent survey carried out among lesbian, gay, bisexual and transgender communities in five central and east European countries showed that only 2–55% of people would feel comfortable revealing their sexual orientation, gender identity or same-sex practices to a healthcare provider.30 Slovenia recently conducted its first National Survey of Sexual Lifestyles, Attitudes and Health.31 Only 1% of men and 0.9% of women reported sexual intercourse with a partner of the same gender compared with 2.6% for both men and women in a similar study in the UK.32
Partner notification for syphilis and gonorrhoea (and chlamydia in a few countries) is obligatory by law in most east European countries.19 21 27 Further information on partner notification is extremely limited. Infrastructure including funding and training of specialists is generally non-existent, so, despite being required by law, partner notification is inconsistently executed and often involves only simple patient referral (requesting the patient to inform sexual partners).
Description of overall trends
A number of broad similarities in STI incidence and trends can be observed across the regions of eastern Europe, but there are important differences in STI rates between the regions, in particular for rates of bacterial STI in the late 1990s. During this period, the reported incidences of syphilis and gonorrhoea in the eastern region and Russia were at least five times higher than in other east European countries. These higher rates persist despite a general reduction in rates of syphilis and gonorrhoea throughout the late 1990s and early 2000s. These decreases coincided with the emergence of several injection drug use (IDU)-driven epidemics in the same region.33 34 Although a modest decline in bacterial STI incidence has been documented in some countries from the central region of eastern Europe, overall trends have been relatively unchanged during this period.
Disease-specific trends: syphilis
Syphilis rates have fallen markedly in the eastern region and Russia over the past decade, although the rates have not fallen to the levels reported before the socioeconomic changes in the early 1990s. Reported cases are concentrated among young heterosexual men and women (M Skerlev, personal communication).35–44 In 2001, of the syphilis cases diagnosed, 50% were in women in Russia (M Gomberg, 2008, personal communication) and 54% in Estonia.37 Data on transmission route in men (ie, whether heterosexually or homosexually acquired) are unavailable. Over half the syphilis cases were either late latent or of unknown duration (figure 2).38–40 45

Trends in rates of syphilis in selected countries from the eastern Europe. (A) Eastern region and Russia. (B) Southeastern region. (C) Central region. Sources: Mavrov and Bondarenko,27 The Estonian Health Inspectorate,37 WHO,41 ESSTI,42 Rubins et al,43 Polish Government44 and M Gomberg, 2008, personal communication.
Compared with the eastern region and Russia, lower or considerably lower rates of syphilis are reported from the southeastern and central regions, respectively. There was a brief increase in syphilis cases around the turn of the century in some countries (Romania, southeastern region; Czech Republic, central region).40 45 In the Czech Republic this reported increase in syphilis was attributed to sex workers, and many cases were among refugees/asylum seekers or immigrants from the eastern region.40 41 Data from Slovenia in the late 1990s suggested that 62% of reported cases were directly or indirectly linked to a foreign infection source, and among these, 73% were traced to countries in the eastern region.45 Since the early 2000s, a slow decrease in syphilis incidence has been reported in several southeastern/central region countries (but not in Poland or Slovenia). Without supporting evidence it is hard to interpret the factors behind the increase in syphilis in some central region countries. For HIV, recent publications have identified men who have sex with men as the most affected population group in Slovenia.46
Disease-specific trends: gonorrhoea
A decline in gonorrhoea rates was noted in many east European countries from the middle 1990s, especially in the eastern region.41 42 In Estonia, cases of gonorrhoea fell steadily from 1144 in 1999 to 288 in 2005.37 Whereas a decrease in new gonorrhoea cases was also observed in the southeastern region, the decline has not been as steep (M Skerlev, MB Geza, personal communication, 2009).41 Rates of reported cases from the central region have decreased slightly throughout the past decade.39 40 42 There is a clear gradient in the reported numbers of gonorrhoea cases across eastern Europe. The highest incidences are observed in the eastern region/Russia. After a substantial decline, the gonorrhoea incidence in the eastern region/Russia is now at approximately the same level as countries with the highest gonorrhoea incidences in the southeastern region (eg, Romania). Central region countries report the lowest gonorrhoea incidences, similar to those in many west European countries (figure 3).1

Trends in rates of gonorrhea in selected countries from eastern Europe. (A) Eastern region and Russia. (B) Southeastern region. (C) Central region. Sources: Mavrov and Bondarenko,27 The Estonian Health Inspectorate,37 WHO,41 ESSTI,42 Rubins et al,43 Polish Government44 and M Gomberg, 2008, personal communication.
Gonorrhoea cases are concentrated among young heterosexual individuals (M Gomberg, 2008, personal communication).36 37 However, whereas most cases in the eastern region occur in women (eg, 60% in Estonia),37 different patterns are reported in the central region (eg, 76% male in Slovakia, 67% male in Slovenia in 2005).42 Data on transmission routes among men (ie, homosexual or heterosexual) are unavailable.
Data on gonococcal antimicrobial resistance across eastern Europe are scant, and this remains an area for future investigation. Kubanova et al47 report on a Neisseria gonorrhoeae susceptibility study involving isolates from Russian gonorrhoea patients (n=1030) collected between January 2005 and December 2006. Virtually all isolates were susceptible to ceftriaxone. However, during 2005 and 2006 in total 5%, 48%, 70% and 77% displayed intermediate susceptibility or resistance to spectinomycin, ciprofloxacin, tetracycline and penicillin G, respectively. Furthermore, 4% of the isolates were β-lactamase producing during these years.47
Disease-specific trends: genital chlamydial infection
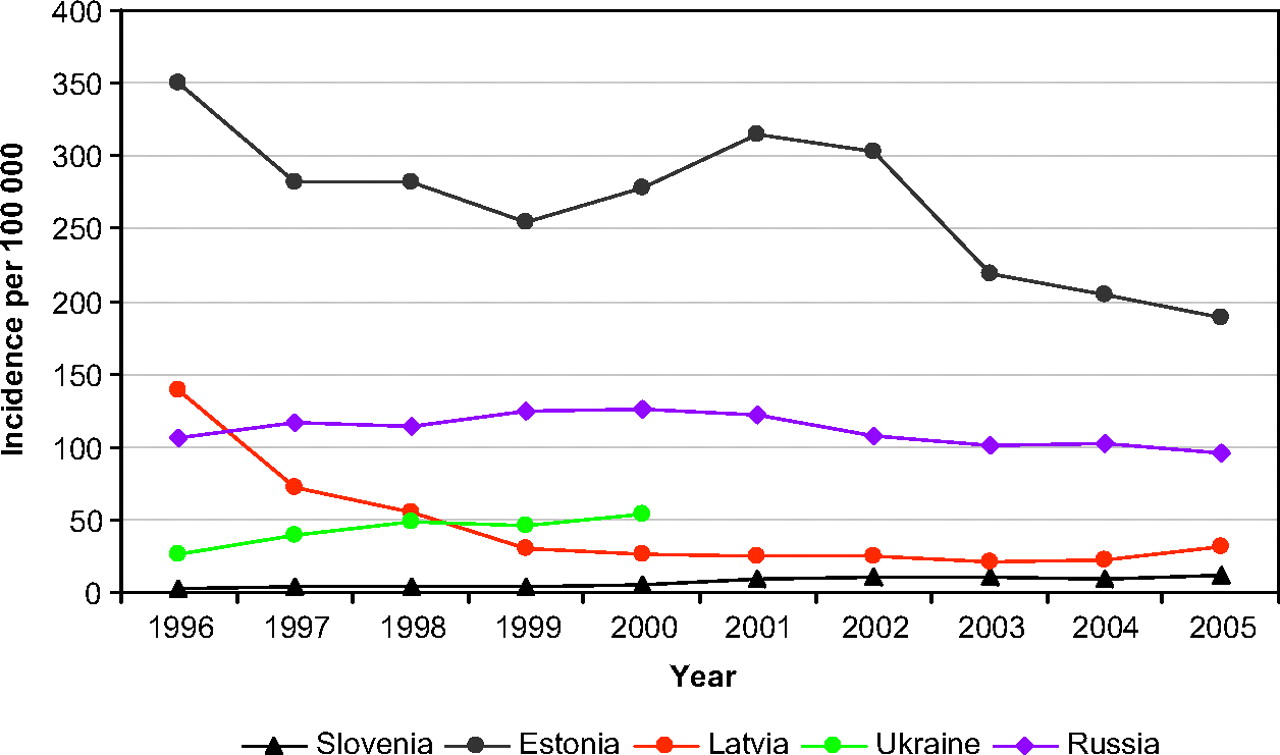
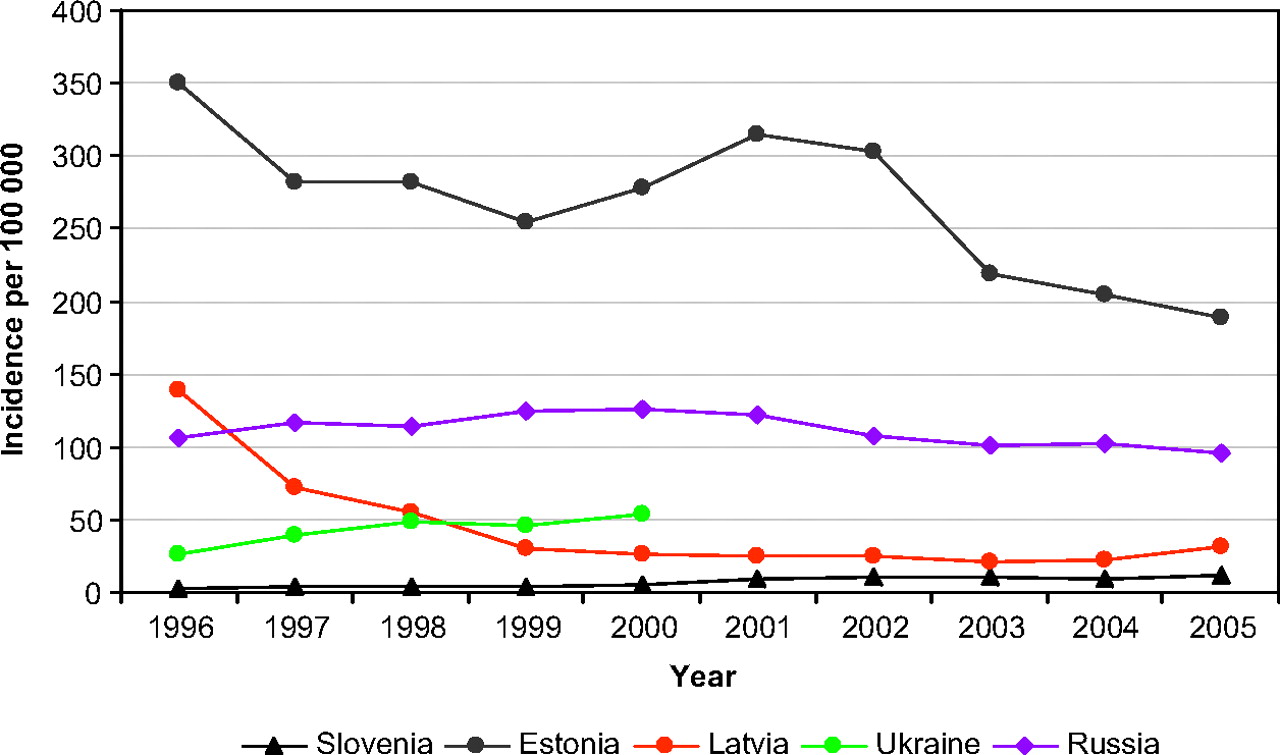
Routine testing and/or clinical case notification of genital chlamydial infection is not widely practised in eastern Europe, and therefore relatively little information is available. Chlamydia screening has not been implemented in the region (except for antenatal screening in Estonia).48 In countries where some testing and/or reporting is implemented (ie, Russia, Ukraine, Latvia, Estonia) genital chlamydial infection is now among the most commonly diagnosed bacterial STI. Relatively stable rates of diagnosis (Ukraine, Russia)25 (M Gomberg, 2008, personal communication) or a slight decline (Estonia, Latvia)37 42 have been observed since the mid-1990s. The highest numbers of new cases are reported from Estonia, where the rate was 189/100 000 in 2005.37 However, chlamydia rates in Estonia are considerably lower than those reported from the neighbouring west European countries.1 In comparison with other east European countries, higher rates of chlamydia in Estonia might reflect the availability of testing rather than a truly greater incidence (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Chlamydia continues to be most commonly reported in young people (ie, under 25 years), and among women.37 42 49 Some data on chlamydia prevalence are available from the region. A prevalence of 6.9% among women and 2.7% among men (18–35 years of age; 11% among women 18–20 years of age) in a population-based sample was reported in Estonia.50 A study conducted among female college students in Lithuania reported a 5.6% prevalence among participants aged 18–31 years (7.1% among sexually active female students 20–24 years of age).51 In contrast, a Slovenian study found 3% of men and 1.6% of women infected with chlamydia (4.1% among men and women aged 18–24 years).52
According to a few publications and surveillance reports, trichomoniasis is the commonest STI in Ukraine and Estonia, with relatively stable notification rates over the past decade.20 27
Discussion
Since the mid-1990s, demographic and socioeconomic trends have increased the potential for STI transmission in eastern Europe. At the same time, the contribution of these risks to an actual increase in STI depends on the interplay of many factors, which cautions against making generalisations about the region as a whole. Developments since the 1990s have increased rather than reduced the diversity between individual countries. The east–west geopolitical gradient in reported STI rates is obvious throughout the eastern European regions, with higher rates in the Russia/eastern region, intermediate in the southeastern region and lowest in the central region. Acknowledging homogeneity in surveillance systems but heterogeneity in diagnostic opportunities and treatment practices across the eastern European countries, reported rates of STI appear to have either decreased or been relatively stable in many east European countries in the past decade. Despite a substantial decrease in reported rates of STI cases (especially syphilis and gonorrhoea) reported in most countries, STI rates in eastern Europe are still significantly higher than those reported from other/western European countries.
Besides changes in the underlying determinants of STI epidemiology (socioeconomic, demographic, political and health systems related) significant developments in proximate determinants of STI infection,53 such as substance abuse and commercial sex work, warrant attention in eastern Europe. As in most transitional societies, sex work has expanded into an important mode of coping with economic inequality and societal unrest.54–58 Beyond sex workers' own risk of STI/HIV acquisition, in the absence of condom use sex workers may play an important role in the spread of STI into the general population.59 The rise in explicitly commercial sex work has occurred concurrently with an increasing diversity of sex work settings and geographical spread of sex work. Some key issues are emerging in the context of STI transmission and sex work in eastern Europe; first, migration, both internal and external. As reported, a substantial proportion—often more than half—of sex workers' clients are migrants either from rural areas, regional cities, or other countries in the region.55 60 Similarly, sex workers tend to migrate from poorer rural areas of countries, from poorer countries within the east European region, or from eastern Europe to wealthier (western European) countries for work, and then return home with their earnings.61 62 The importance of within-country migration is reflected by the high numbers of sex workers in east European capital cities (in 2005 it was estimated that there were between 30 000 and 150 000 sex workers in Moscow; at least 20 000 in St Petersburg; and 10 000–20 000 in Minsk).61 Another factor is sex workers' vulnerability and risk of violence in conjunction with limited access for harm reduction, prevention and health care.61 63 64 As a result, consideration should be given to decriminalising sex work, and revising or eliminating national policies that reduce sex workers' rights and access to health services.61 64–69
Illicit drug use rose sharply at the end of the 1990s in eastern Europe, but this growth probably stabilised around 2005 (expert opinion suggests that the numbers of new users had been decreasing since 2000).70 Over the past 10 years, the increasing problem of drug use and a limited response in eastern Europe has led to epidemics of HIV and hepatitis. International research has indicated that alcohol and drug consumption can impair judgement and may increase the likelihood of engaging in risky sexual behaviours.71 72 A multisite study in Russia found prevalences of positive syphilis serology of 6–20% among injection drug users.73 Empiric data on non-injection substance use and bacterial STI rates from the region are scarce.
This study has limitations. There is currently no single, comprehensive source of information on incidence and trends in diagnosed STI in eastern Europe. The overall picture was assembled from sources that vary in their coverage, detail and accuracy. In part this reflects the variations in data availability, surveillance, STI treatment and care services across the region. Data on only a limited number of countries from the eastern European subregions were available. Acknowledging the potential caveats of passive surveillance in the region, there is some homogeneity in infrastructure for STI diagnosis, treatment and reporting systems that enables comparisons of disease rates and monitoring trends across eastern Europe.
The challenge facing STI control policies in the region will be deciding how to adapt to the simultaneous socioeconomic, demographic, political, health behaviour and health system changes. Clearly, the reduction in preventive health services in many countries and the changes in STI provision (from universal dermatovenerological access to STI provided through multiple medical specialists) create new requirements to strengthen the public health component of STI control. The ability to control STI requires an effective and comprehensive public health surveillance capacity. Overcoming barriers to STI surveillance (including the lack of appreciation of the value of high-quality surveillance data and a weak societal commitment) and developing comprehensive surveillance systems is of great urgency.
Key messages
STI rates reported from most eastern European countries are still significantly higher than those from other/western European countries.
Reported rates of STI have either decreased or been relatively stable in many eastern European countries in the past decade.
There is an east–west geopolitical gradient in reported STI rates within eastern Europe (STI rates Russia/eastern region>>southeastern region>central region).
Gains in STI control may be achieved though greater collaboration and practice harmonisation at the European level.
Acknowledgments
The authors are grateful to Drs Michael Gomberg (Russia), Airi Põder (Estonia), Mihael Skerlev and Marko Potočnik, (Croatia), Molnar B Geza (Romania) and Magdalena Rosinska (Poland) for sharing country-specific STI data and contextual information with us. The authors also thank Emma Savage and the ESSTI network for sharing collected data.
References
Supplementary materials
Web Only Data 86/1/6
Files in this Data Supplement:
Footnotes
Supplementary web appendix is published online only at http://sti.bmj.com/content/vol86/issue1
Funding This study was finances by the National Institutes of Health, Norwegian Financial Mechanism/EEA (grant EE0016), the Estonian Ministry of Education and Science (target funded project 0132703s05) and Estonian Science Foundation (grant 7619).
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Whistlestop tour