Article Text

Abstract
Chancroid is a sexually transmitted disease (STD) caused by the Gram negative bacterium Haemophilus ducreyi and is characterised by necrotising genital ulceration which may be accompanied by inguinal lymphadenitis or bubo formation. H ducreyi is a fastidious organism which is difficult to culture from genital ulcer material. DNA amplification techniques have shown improved diagnostic sensitivity but are only performed in a few laboratories. The management of chancroid in the tropics tends to be undertaken in the context of syndromic management of genital ulcer disease and treatment is usually with erythromycin. A number of single dose regimens are also available to treat H ducreyi infection. Genital ulceration as a syndrome has been associated with increased transmission of human immunodeficiency virus (HIV) infection in several cross sectional and longitudinal studies. Effective and early treatment of genital ulceration is therefore an important part of any strategy to control the spread of HIV infection in tropical countries.
- chancroid
- sexually transmitted disease
- Haemophilus ducreyi
Statistics from Altmetric.com
Chancroid is a sexually transmitted infection caused by the Gram negative bacterium Haemophilus ducreyi. The disease manifests as genital ulceration which may be accompanied by regional lymphadenitis and bubo formation. Chancroid may also be spread to other anatomical sites by auto-inoculation, a clinical feature first demonstrated experimentally by Ducrey in 1889.1 It occurs sporadically in the developed world, usually in individuals who have recently returned from chancroid endemic areas or occasionally within the context of localised urban outbreaks which may be associated with commercial sex work.2–4 Within the resource poor areas of the world, however, chancroid remains a major cause of the genital ulceration syndrome. Recent reports from South East Asia and Africa suggest that the incidence of chancroid may be declining in the face of a rapidly rising incidence of genital herpes.5–7 This observation has fuelled recent debate as to the feasibility of chancroid eradication.5 Genital ulceration has been shown to be a major co-factor in the transmission of human immunodeficiency virus type 1 (HIV-1) infection both through cross sectional cohort studies and prospective longitudinal studies.8–10 Therefore, effective diagnosis and treatment of chancroid may play an important part in slowing down the HIV-1 epidemic in those parts of the world where both diseases are prevalent.
CLINICAL PRESENTATION
It is believed, though unproved, that H ducreyi initiates an infective process within the genital skin after the formation of epidermal microabrasions during sexual intercourse. A tender erythematous papule may develop 4–7 days later before progressing to the pustular stage. An estimated delivery dose of approximately 30 colony forming units of H ducreyi organisms has been reported to cause a papule formation rate of 95% and a pustule formation rate of 69% in the experimental human challenge model.11 Pustules often rupture after a further 2–3 days to form painful shallow ulcers with granulomatous bases and purulent exudates (fig 1). The ulcer edge is typically ragged and undermined. Clinical observations from the pre-antibiotic era demonstrate the chronicity of chancroid ulceration which can take several weeks or months to resolve in the absence of effective antimicrobial therapy.12,13 Naturally occurring chancroid is usually more prevalent in men than women. This sex difference has also been observed experimentally in both humans and macaques.14,15 Lesions typically occur on the prepuce and frenulum in men and on the vulva, cervix, and perianal area in women. Complications include phimosis in men and further phagedenic ulceration due to secondary bacterial infection. Extragenital cases of chancroid with lesions on inner thighs, breasts, and fingers have been reported but are rarely seen in clinical practice. Painful, tender inguinal lymphadenitis typically occurs in up to 50% of cases and the lymph nodes may develop into buboes. The lymphadenopathy is usually unilateral and tends to be more prevalent in men (fig 2). If not aspirated or drained through incision, fluctuant buboes can rupture spontaneously.

Penile ulceration due to chancroid.

Right sided inguinal bubo and penile ulcer in a man with chancroid.
It has been reported that the proportion of genital ulcers attributable to herpes simplex virus (HSV) in sub-Saharan Africa is increasing and mixed infections with two or more of H ducreyi, Treponema pallidum, and HSV are well described.16–18 The effect of concurrent HIV infection on the clinical progression of chancroid is unclear at this time. Published data suggest that HIV seropositive men have increased numbers of genital ulcers which may heal at slower rates.19,20 This is of importance in view of the epidemiological synergy that co-exists between HIV infection and genital ulceration in areas of the world where both are common.8 HIV-1 has been detected in chancroid ulcer material obtained from both men and women.21,22 In addition, chancroid ulcers contain numerous CD4 positive T lymphocytes which could increase the susceptibility of an individual infected with H ducreyi to subsequent infection by HIV.23
DIAGNOSIS
Clinical diagnosis and laboratory culture of H ducreyi were used as “gold standards” for the diagnosis of chancroid in the past. The advent of DNA amplification tests has recently demonstrated both to be inaccurate measures of the true prevalence of H ducreyi infection among patients with genital ulcer disease. Physical examination findings have a low sensitivity and specificity for diagnosing primary syphilis, chancroid, and genital herpes, even in areas where these diseases are common and where attending physicians are experienced in the management of genital ulcer disease.24–26 The sensitivity of H ducreyi culture relative to the multiplex polymerase chain reaction (M-PCR) has been shown to be approximately 75% in studies which have used genital ulcer derived swabs.27,28 Currently available clinically based and research based methodologies for the diagnosis of chancroid have previously been reviewed by the author.29 It should be pointed out that Gram stained ulcer material should not be examined as a means to diagnose chancroid owing to poor sensitivity and specificity of this test.30
H ducreyi is a fastidious bacterium requiring a relatively expensive nutritive base to grow on and is an extremely difficult organism to culture from clinical specimens in the hands of inexperienced laboratory staff. As a result, conventional laboratory culture facilities are often not available in STD clinics or simply not affordable in resource poor countries. In those clinical settings with laboratory support, clinicians are often faced with the dilemma of whether to treat a patient empirically for chancroid at the first visit or whether to request staff in their microbiology laboratory to provide a suitable medium with which to culture H ducreyi on a subsequent day in the hope that the patient is not lost to follow up. Even if culture facilities are available, it often takes several days for results to become available.
The role of Stuart’s, Amies’, and thioglycolate hemin based transport media has been evaluated as transport media for H ducreyi.31 Increased survival of H ducreyi from less than 24 hours to up to 4 days was seen when specimens were held at 4°C. The use of transport media in locations with a refrigeration facility may overcome the significant cost of distribution of culture media with short shelf lives to clinics where the disease is only seen sporadically. There did not appear to be any major advantage in the overall rate of recovery of H ducreyi using transport media compared to direct plating.
Most H ducreyi strains grow best at 33°C in a humid atmosphere containing 5% carbon dioxide.32 Improved H ducreyi isolation rates are seen using microaerophilic conditions in which culture plates inoculated with H ducreyi are incubated in a closed anaerobic jar without a catalyst but with two CO2 and H2 generating sachets.33 Numerous artificial media have been developed and have been reviewed elsewhere.29,34
Several DNA amplification based techniques have been developed in an attempt to improve the sensitivity of the laboratory diagnosis of chancroid.28,35–38 The technique of M-PCR involves the addition of multiple primer pairs to the reaction mixture in order to simultaneously amplify distinct DNA sequences from different targets in the processed lesion material. The research based M-PCR described by Orle et al offers a highly sensitive and specific way to detect the three most common aetiological agents of genital ulcer disease—namely, HSV, Treponema pallidum, and H ducreyi.28 Specimens for M-PCR may easily be transported from the STD clinic to a remote laboratory and can be stored at −70°C if required for batch testing. The ability to perform DNA amplification based techniques requires access to laboratories with specialised molecular biological expertise. As such, this expensive technology will continue to have a role in research and outbreak investigation but is not likely to be made available to clinicians in most worldwide settings where patients with chancroid seek STD care.
SYNDROMIC MANAGEMENT
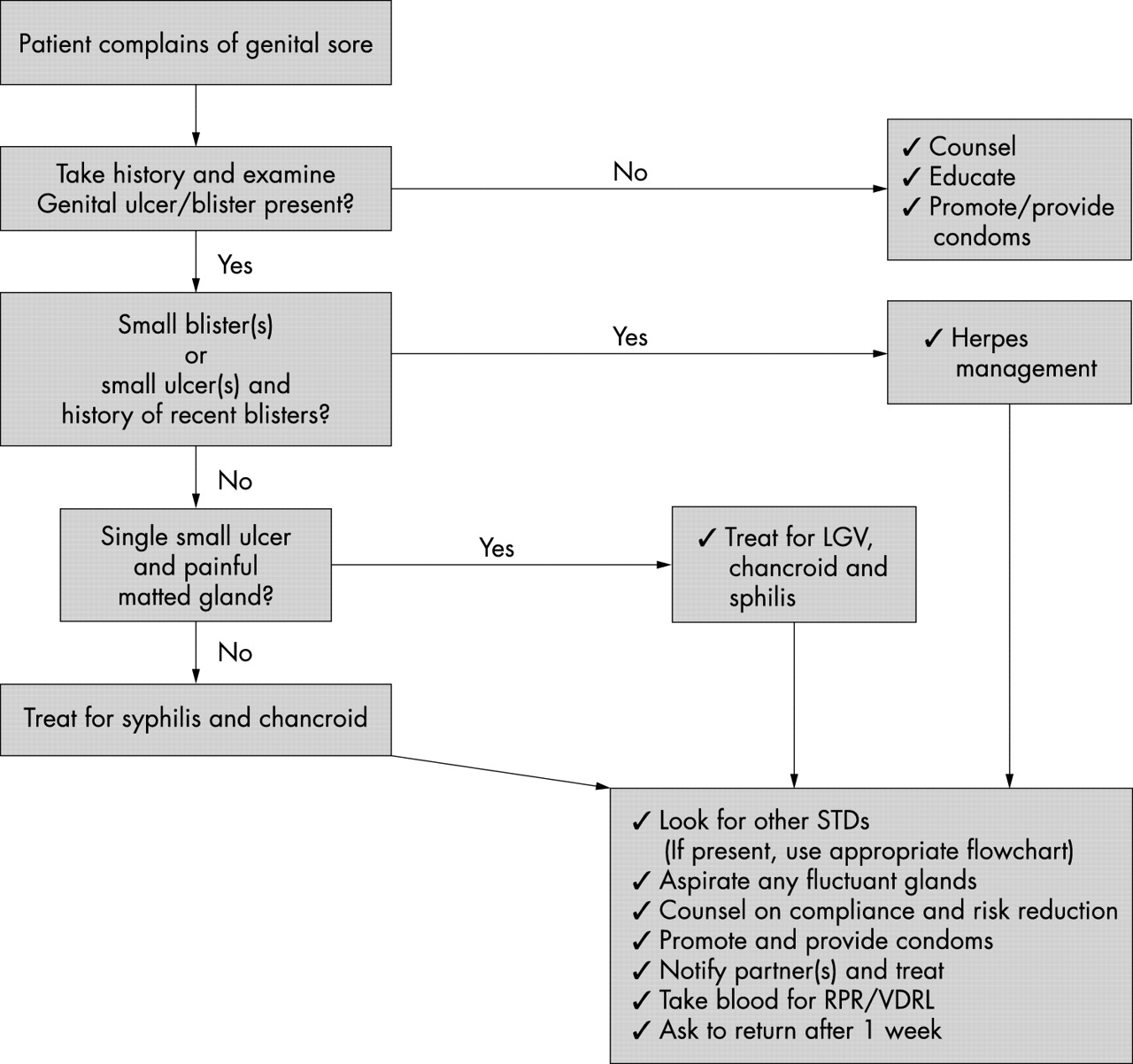
The World Health Organization (WHO) developed and advocates the use of syndromic management to address the limitations of both aetiological and presumptive aetiological diagnosis and management of symptomatic STDs.39 The principle behind this approach is that patients are treated at the first visit with a combination of antimicrobials that will treat the local probable aetiological agents. Syndromic management flow charts for the management of genital ulcers have been prepared which provide simple instructions to health providers on how to manage the patient and his/her sexual contact(s) (fig 3).40 The process requires little or no clinical description of the ulcer itself and does not require laboratory identification of the causative pathogen(s). Syndromic management has been proved to be more successful than a hierarchical algorithm or clinical diagnosis in the management of genital ulcer disease in Rwanda.41 It is envisaged that M-PCR will have an important role in validating syndromic algorithms for the management of genital ulcer disease as the aetiology of this syndrome varies geographically and over time. It may be appropriate to perform laboratory diagnostic and antimicrobial susceptibility testing on specimens from ulcers of patients failing to respond to antimicrobial therapy in situations where reinfection from an untreated partner has been excluded.

{kind=link}
{kind=link}
{kind=link}
Syndromic protocol C for genital ulcer disease evaluated in Lesotho by Htun et al40 (reproduced from
TREATMENT
Recommended and alternative treatment regimens from the WHO, the Centers for Disease Control and Prevention (CDC), and the United Kingdom’s Clinical Effectiveness Group are presented in table 1.42–44 There is some debate concerning the duration of ciprofloxacin therapy for chancroid; the WHO recommends a single 500 mg oral dose whereas the CDC recommends 500 mg twice daily for 3 days. A recent double blind randomised controlled trial in Kenya demonstrated comparable cure rates for both single dose ciprofloxacin (92%) and a 1 week course of erythromycin (91%).45 Pregnant women should be treated with either erythromycin or ceftriaxone regimens. Patients with underlying immunosuppression due to HIV infection should be carefully followed up as reduced healing of genital ulcers and persistence of H ducreyi in the lesions has been reported in this group.19,46–48 There also appears to be an increased likelihood of treatment failure in uncircumcised individuals with chancroid.19,48,49 Treatment failures have been reported in African patients treated with single doses of either intramuscular ceftriaxone or oral fleroxacin.19,48 Undiagnosed co-existing HSV infection, particularly in immunosuppressed HIV seropositive patients, may also account for some of the observed cases where treatment has failed to cure chancroid.
Recommended treatment regimens for chancroid from the World Health Organization (WHO), the Centers for Disease Control and Prevention (CDC), and the United Kingdom Clinical Effectiveness Group (CEG)
Plasmid mediated antimicrobial resistance has been documented for a number of agents, including penicillins, tetracyclines, chloramphenicol, sulfonamides, and aminoglycosides.50 Much less is known about chromosomally mediated resistance to antimicrobials in H ducreyi but decreased susceptibility has been described for penicillin, ciprofloxacin, ofloxacin, and trimethoprim.50 There is little, if any, antimicrobial surveillance occurring in countries where chancroid is common. Based on the emergence of resistant strains in Rwanda,51 the WHO has recommended that chancroid is not treated with trimethoprim/sulfamethoxazole based regimens unless the antimicrobial susceptibility profiles of local H ducreyi isolates are known.42
Fluctuant buboes should be aspirated in order to provide symptomatic relief for the patient and to avoid the further complication of spontaneous rupture.42,52 Incision and drainage of fluctuant buboes, with subsequent packing of the wound, has also been recommended as an effective management strategy for chancroid and avoids the need for frequent bubo re-aspirations.53 This latter study was performed in New Orleans and not in the tropics; it is as yet unclear as to whether a similar approach in the tropics would be associated with an increased postoperative morbidity.
OTHER MANAGEMENT ISSUES
In countries where the practice of syndromic management is adopted, patients with genital ulcers should receive treatment for both chancroid and syphilis. Therapy for granuloma inguinale should be added to the regimen in endemic areas and treatment for lymphogranuloma venereum should be given if inguinal buboes are present. Patients with genital ulcers should be seen after treatment to ensure that healing has occurred, to exclude the possibility of reinfection, and to ensure that partner notification has taken place. All patients with genital ulcers should receive appropriate health education and safer sex practices should be discussed. Serological screening for both syphilis and HIV infection should be offered at the time of genital ulcer presentation and again after 3 months at the end of the window period for both diseases. In clinics where diagnostic facilities are available, patients should be appropriately screened for all pathogens causing genital ulceration as well as for other STDs.
CONCLUSIONS
Chancroid remains an important cause of the genital ulceration syndrome in the tropics where erythromycin has been the mainstay of therapy. Single dose oral azithromycin or ciprofloxacin and intramuscular ceftriaxone regimens offer advantages in terms of improved patient compliance. There are some data to suggest that HIV seropositive and uncircumcised patients are more likely to fail single dose therapeutic regimens and so these groups of patients need more intensive follow up. WHO recommended syndromic management for genital ulceration includes therapy for both chancroid and syphilis. In those parts of the world where diagnostic facilities exist, the diagnosis of chancroid is normally made by laboratory culture of H ducreyi. The more sensitive DNA amplification techniques remain research tools at the present time.
REFERENCES
Footnotes
-
Series editor: David Lewis
Linked Articles
- Web top 10
- Web top 10