Article Text

Abstract
Design/setting: A cohort study of 1037 people born in Dunedin, New Zealand, in 1972 or 1973.
Participants: At assessment at age 32 years, 884 participants (432 women and 452 men; 87.1% of the surviving cohort) provided both sera and information on sexual behaviour.
Main outcome measures: The proportion of participants with antibodies to HSV-2 infection at ages 26 and 32 years was measured, and the incidence rates from first coitus to age 26 years and from age 26 to 32 years calculated, adjusting for the number of sexual partners and same-sex contact in these age periods.
Results: At age 32 years, 14.6% of men and 22.5% of women had antibodies to HSV-2. The incidence rates for men and women from first coitus to age 26 years were, respectively, 6.5 and 14.3 per 1000 person-years. The incidence rates for men and women from age 26–32 years, respectively, were 14.3 and 15.8 per 1000 person-years. When adjusted for sexual behaviour, the incidence rate ratio, comparing the older with the younger age periods, was 2.9 (95% confidence interval (CI) 1.7 to 4.9) for men and 2.0 (1.2 to 3.4) for women. The adjusted incidence rate ratio when comparing women to men from first coitus to age 26 years was 2.5 (1.6 to 4.0), and from age 26–32 years was 1.3 (0.78 to 2.2). A test for interaction indicated that men and women had different patterns of incidence over time (p = 0.039).
Conclusion: In the general population, the risk of acquiring HSV-2 infection seems to increase with age at least to the early 30s, and differences in risk of acquisition for women compared with men become less with age. Health promotion and treatment to control HSV-2 infection should be aimed at all ages, not just at the young.
- HSV-2, herpes simplex virus type 2
Statistics from Altmetric.com
Infection with herpes simplex virus type 2 (HSV-2) is the most common cause of genital ulcers in developed countries and is a major public health issue.1,2 Although the main direct effect on people is psychosocial,3 it almost certainly facilitates HIV acquisition,4 and can cause a devastating encephalopathy if transmitted to an infant around birth.5
Accurate assessment of HSV-2 occurrence requires measurement of HSV-2 antibodies, as many infections are asymptomatic or unrecognised.2 Prevalence increases with age and is higher among women than men.6–8 Incidence rates are best measured directly by seroconversion in cohort studies, but have been estimated from prevalence data.9 The one cohort study in a developed country with follow-up from the teenage years included only women, and did not collect information on sexual behaviour.10 It found that the incidence was higher in the age period 18–22 years than earlier, then remained similar when they were aged 23–29 years. However, it is unknown whether these age-specific incidence patterns reflect differences in sexual behaviour by age or the underlying risk of acquisition by age, nor is it known whether male patterns are similar to female patterns.
We measured antibodies to HSV-2 at ages 21, 26 and 32 years and linked these to sexual behaviour in a population-based birth cohort to determine whether there is an effect of age and sex on incidence of HSV-2 independently of sexual behaviour. We expected that the incidence would be higher at older ages and among women.
METHODS
We studied those participating in the Dunedin Multidisciplinary Health and Development Study, a longitudinal study of a cohort born in Dunedin, New Zealand, between 1 April 1972 and 31 March 1973. The sample was first followed up at 3 years of age when 1037 of 1139 eligible children were seen.11 Subsequently, they were seen every 2 years until 15 years, then at 18, 21 and 26 years, and most recently at 32 years. We asked questions on sexual behaviour, which were mostly based on those used in the 1990 British National Survey of Sexual Attitudes and Lifestyles, presented by computer at ages 21, 26 and 32 years.12 Information on the first heterosexual intercourse, including age, was asked only at age 21 years.
At ages 21, 26 and 32 years, we performed HSV-2 serology on serum using an indirect enzyme-linked immunosorbent assay (HerpeSelect 2 ELISA IgG, Focus Technologies, Cypress, California, USA).13,14 In our experience, the manufacturer’s recommendation—that an index value of >1.10 should be presumptive for antibodies to HSV-2—yielded a high rate of false-positive results. Hence we used a cut-off value of 3.5, and those that gave an equivocal result (between 0.9 and 3.5) were resolved using HSV-2 western blot.15
At the age 32 assessment, we calculated prevalence using data from all participants who had their sera tested. We calculated incidence rates (per 1000 person-years) for each age period, including only those who tested negative for HSV-2 at the previous assessment and had experienced coitus, taking into account years since first coitus. First coitus was defined as the first of either heterosexual intercourse or same-sex contact. For those of whom age at first heterosexual intercourse was unavailable, we estimated age of first coitus on the basis of the first assessment at which sexual contact was acknowledged. The numbers of sexual partners were assessed on the basis of reports of heterosexual intercourse, and for men reports of anal intercourse with male partners for the time period. Those who had had coitus but reported no such partners in a subsequent time period were included in the analysis, as HSV-2 may be transmitted through other sexual activity, and information on opposite sex partners without intercourse was not collected.
We calculated incidence rates and 95% confidence intervals (95% CI), associated incidence rate ratios and 95% CI, using robust Poisson regression in Stata V.8, including years since the first coitus as an exposure variable. For analyses that compared rates across assessments, we clustered the study members by their study identification number to account for repeated measures. To assess whether rates across assessments differed by sex, the model was refitted, including an interaction term for sex and age. To test for linear trend, analyses were repeated using number of sexual partners as a continuous variable.
RESULTS
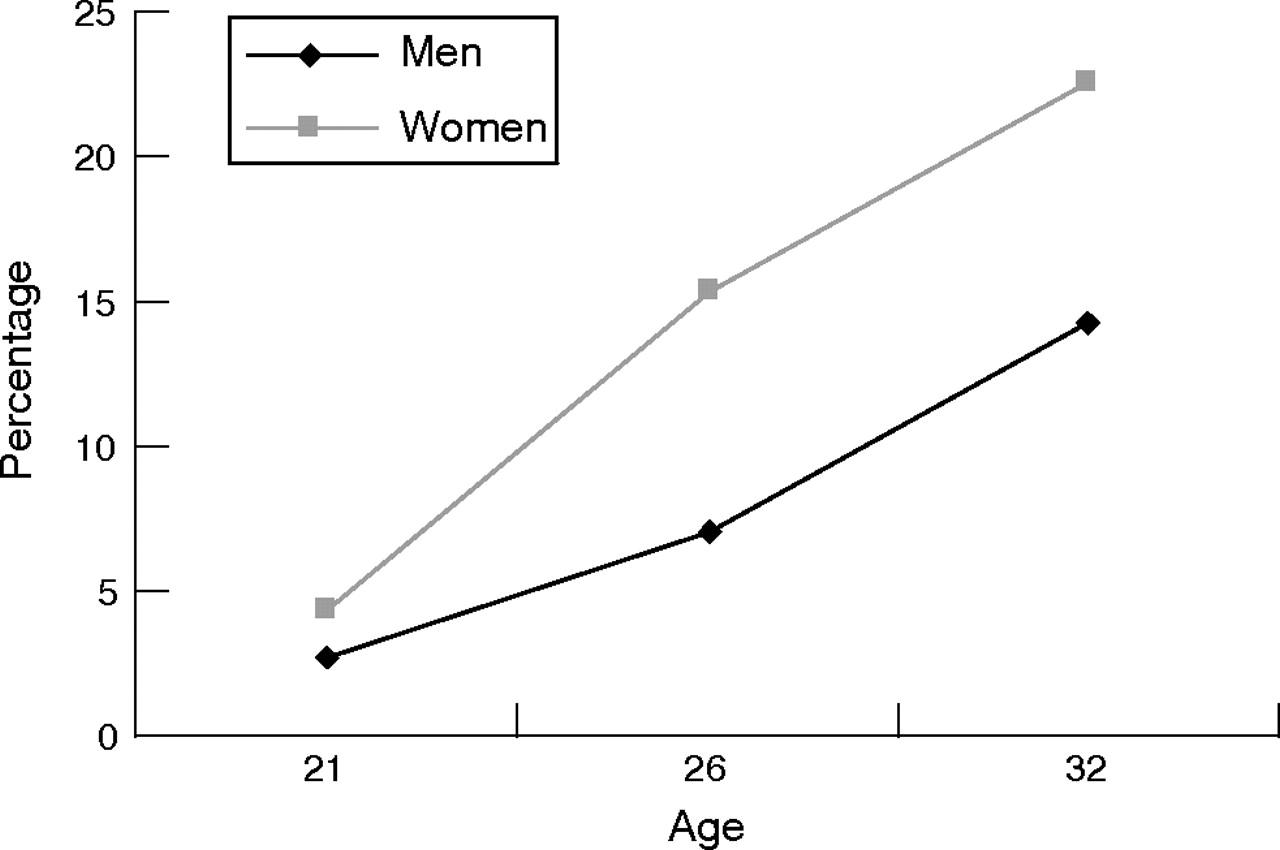
At age 32 years, we tested sera from 884 participants (432 women and 452 men, 87.1% of the surviving cohort) for HSV-2 antibodies. The overall prevalence of HSV-2 infection was 18.4%, higher among women (22.5%) than among men (14.6%; p = 0.003). As reported previously, the prevalence at age 21 years was 4.3% and 2.7% for women and men, respectively, and at age 26 years, 15.3% and 7.1% (fig 1).13,14
{kind=link}
Seroprevalence of HSV-2 at 21, 26 and 32-year assessments.
Table 1 shows the incidence rates for the two age periods; p values resulting from the comparison of these rates are given in the text. For the period from first coitus to age 26 years, the incidence rate for men (6.5 per 1000 person-years) was less than half that for women (14.3 per 1000 person-years; p = 0.001). For the age period 26–32 years, the rates were similar for men and women: 14.3 and 15.8 per 1000 person-years, respectively (p = 0.69). The incidence rates increased between these age periods for men (p = 0.002) but not for women (p = 0.64). Among the women, there was a linear trend for the incidence to increase with number of partners both up to age 26 years (p = 0.005), and from age 26 to 32 years (p = 0.001). For the men, this relationship was not so clear (p = 0.11 up to age 26 years, and p = 0.13 from age 26–32 years). Within each stratum of the number of sexual partners (except women with no or one partner), the incidence was higher from age 26–32 years. Men with same-sex contact from age 26–32 years were more likely to become infected (p = 0.035), but this relationship was not found when younger, or for women.
Relationship between herpes simplex virus type 2 (HSV-2) incidence rate (per 1000 person-years) and the number of sexual partners and same-sex contact in the period from first coitus to age 26 years, and from age 26–32 years
Table 2 shows the comparisons of incidence by age period and sex. Comparing age periods, the unadjusted incidence rate ratio was 2.2 (95% CI 1.3 to 3.6) for men, but only 1.1 (95% CI 0.73 to 1.7) for women; the test of interaction indicated that men and women had different patterns of incidence over time (p = 0.039). When adjusted for number of sexual partners and same-sex contact, the incidence rate ratio increased for men to 2.9 (95% CI 1.7 to 4.9) and for women to 2.0 (95% CI 1.2 to 3.4). The marked change, particularly for the women, is because the pattern of sexual partnerships is very different in the two age periods. Comparing incidence by sex in the two age periods, the incidence rate ratio was 2.2 (95% CI 1.4 to 3.4) for women compared with men up to age 26 years, but was only 1.1 (95% CI 0.69 to 1.8) for the age period 26–32 years. When adjusted for number of sexual partners and same-sex contact, the incidence rate ratio increased for women compared with men to 2.5 (95% CI 1.6 to 4.0) up to age 26 years, but only to 1.3 (95% CI 0.78 to 2.2) for the age period 26–32 years.
Comparison of incidence rates (a) by age period according to sex and (b) by sex according to age period
DISCUSSION
Our main finding is that incidence rates of HSV-2 among uninfected men and women in their late 20s and early 30s, after adjustment for sexual behaviour, are two to three times as high as in younger ages, as those in younger ages. Comparing men and women, incidence rates for women, after such adjustment, are about two and a half times higher than those for men up to 26 years, but only slightly higher from age 26–32 years. Hence, increasing age is independently associated with increasing incidence (or risk) for both men and women; the steeper rise for men resulted in a much reduced sex difference in the older age period.
The strengths of this study are that serological analyses were undertaken three times over an 11-year period; that it included men and women from a general population sample with an exceptionally high rate of follow-up; and that the results were linked to sexual behaviour. Limitations include the relatively small sample size, and that data on condom use were not available for the entire period. Adjusting for condom use over the 12 months before ages 26 years and 32 years made no appreciable difference to the results (data not shown). Although information on sexual behaviour was collected using a computer-presented questionnaire, some degree of bias in social desirability according to sex might have influenced the responses on partner numbers.16 Nevertheless, this is likely to act similarly at each age and hence not affect our comparisons over time. We did not collect data on the sexual behaviour of partners, hence there may be residual confounding. As we did not test for HSV-1 infection, our figures will underestimate the overall risk of any genital herpes infection.
Previous studies have not shown increasing risk of HSV-2 over early adulthood. Although the cohort study by Christenson et al10 showed similar incidence rates for women aged 18–22 and those 23–29 years, these were not adjusted for sexual behaviour.10 If they had been, they would have probably found adjusted incidence rates to be higher in the older age groups, as we found. Two studies did control for partner numbers and found HSV-2 acquisition to be higher at younger ages—among discordant monogamous heterosexual couples in one study,17 and among sexually transmitted disease clinic attenders in the other study,18 enrolled in an unsuccessful vaccine trial. But these studies were not population-based, and in one study all were exposed to symptomatic HSV-2 infection.17 In the general population, exposure to HSV-2 is seen to differ by age. Hence, findings of these studies are not generalisable.
Several factors are likely to explain the increasing risk of HSV-2 acquisition with age. Firstly, as a person gets older there will be a tendency for new sexual partners also to be older, and he or she is more likely to harbour HSV-2 as prevalence increases with age. Secondly, over the age periods studied, sexual relationships will tend to last longer. As the risk of HSV-2 transmission per sex act is low,17 longer relationships would increase the risk if risk per act is independent of the number of acts. Third, condoms may be used less in heterosexual relationships when older.19 An alternative explanation is that the risk for HSV-2 was increasing over all ages when the cohort was examined, because of temporal changes in sexual behaviour. It is difficult to disentangle such a possible effect from that of age in a cohort, and there are no appropriate New Zealand prevalence data to check for this.
We expected from prevalence data that the younger women would have a higher incidence than similar-aged men, as was the case. This is most likely explained by different patterns of age mixing among men and women, with women tending to have older partners,20 and different transmission risk; men to women transmission is more efficient than women to men transmission.21 That the women to men ratio of adjusted incidence rates declined with age was unexpected, as prevalence rates are always higher among women than among men, as our study found.7 Changing patterns of dissortative age mixing by age20 may have some bearing on this. Although women in our sample were more likely than men to have older partners at each age, the sex difference was less at age 32 years (data not shown). Another factor suggested to reduce transmission rates for women when older is that they may be better able to negotiate condom use.20
We are not aware of any other population-based studies in developed countries which have examined the women to men ratio of incidence rates with age. The study of sexually transmitted disease clinic attenders found no initial sex difference, but adjusting for sexual behaviour increased the risk ratio for women to 1.8 (95% CI 1.1 to 2.8) compared with men.18 This is compatible with our results as that study had a wide age range and did not examine the sex ratio by age. In contrast, among discordant couples in the vaccine trial, the women to men ratio of HSV-2 acquisition per sex act was nearly 6.17 This high ratio may be a consequence of the unusual population. The lack of any difference between incidence rates for men and women from age 26–32 years in our study, even after adjusting for sexual behaviour, reflects the fact that incidence increased more steeply for men than for women from the younger to the older age period. The reason for the steep increase for men is unclear.
Our finding of extensive spread within the population illustrates Garnett’s analysis that an infection such as HSV-2, characterised by long duration and low infectivity, would be expected to manifest in the population as a slowly rising epidemic reaching a high prevalence throughout the population and not just among those with marked risk.22 In contrast, an epidemic of a more easily transmitted and short-lived (particularly when treated) infection such as gonorrhoea will rise rapidly, but will persist only if driven by substantial high-risk groups and poor access to care.
Key messages
-
Taking sexual behaviour into account, the risk of acquiring HSV-2 was higher for both men and women between 26 and 32 years of age than when younger.
-
Although women are at greater risk than men up to 26 years, the risks were similar between 26 and 32 years.
-
Although increasing numbers of sexual partners increases the risk of HSV-2, in this study two thirds of new HSV-2 infections in women aged 26–32 years, and about half in the men, occurred among those who reported ⩽4 partners in that period.
-
Health promotion and treatment to control HSV-2 infection should be aimed at people of all ages, not just at the young.
The results are likely to be generalisable to many other developed country populations. Our age-specific prevalence at various ages in this study were within the range of the general population estimates in several European countries,6 higher than in the UK,23 but somewhat lower than in the US.8 However, they may not be generalisable to developing countries and some subpopulations in developed countries.
The implications of HSV-2 incidence increasing with age relate to both clinical practice and public health. People and clinicians should be aware that overall there is an increased possibility of acquiring HSV-2 infection from any one new sexual partner as people get older. We found that two thirds of HSV-2 infections in women aged 26–32 years occurred among those who reported⩽4 partners, compared with <20% for women ⩽26 years of age. For men the proportions were 48% and 12%. This finding is especially relevant to women, as the late 20s and early 30s are now the commonest ages of childbearing, and women with new infections are at most risk of transmitting the virus to their infants.
Public health policy in relation to sexually transmitted infections has tended to focus on young people. Indeed the highest number of attendances for genital herpes infection at sexual health clinics in New Zealand and the UK is among women aged 20–24 years.24,25 Yet, to control the epidemic in populations where a high prevalence of infection drives the incidence, it is important to address all factors that contribute at any age. This includes the availability of suppressive treatment. In addition, if the randomised trials of HSV-2 antiviral treatment currently under way do show an effect on the incidence of HIV infection,4 then controlling HSV-2 will be a proven method of controlling HIV spread.
Acknowledgments
We thank the study members and their families for their long-term commitment to the Dunedin Multidisciplinary Health and Development Study (DMHDS), and the staff involved in the collection of the data and other aspects of the DMHDS. We also thank Associate Professor Richie Poulton (the Director of the DMHDS), Dr Edward Coughlan and Dr Debbie Williams for helpful comments.
REFERENCES
Footnotes
-
Published Online First 17 August 2006
-
Funding: This study was funded by the Health Research Council of New Zealand.
-
Competing interests: None.
-
Ethical approval: Ethical approval was granted by the Otago Ethics Committee.
-
Contributors: ND and CP were responsible for the design of this aspect of the DMHDS, the data collection, interpretation of the findings and drafting of the paper. TvR, helped by PH, was responsible for the statistical analysis, and both of them contributed to the interpretation of the findings. JT and AC were responsible for the serological analyses. All authors contributed to the writing and revision of the paper. ND is the guarantor.
-
Objective: To determine how the risk of acquisition of herpes simplex type 2 (HSV-2) infection varies with age and sex in early adulthood.
Linked Articles
- Correction