Article Text

Abstract
Objectives: The epidemiology of human papillomavirus (HPV) infection in men in Kenya is largely uncharacterised. We set out to determine the prevalence and determinants of HPV infection among sexually active fishermen along Lake Victoria in the Kisumu district of Kenya.
Methods: Genital swabs were obtained from 250 consenting fishermen from 18 beaches and a detailed sociodemographic questionnaire was administered. HPV positivity was determined by polymerase chain reaction amplification and detected by dot blot hybridisation with generic HPV and β-globin probes. HPV positive samples were genotyped using the Roche Linear array assay.
Results: Overall, 144 (57.6%) fishermen had detectable HPV DNA, 106 (42.4%) were infected with oncogenic HPV types, with HPV-16 being the most frequent type (12.4%). Among HPV positive men, 105 (72.9%) were infected with more than one HPV type and 20 (13.9%) were infected with more than six different types. HIV seropositive men (PR 1.49, 95% CI 1.19 to 1.86) and those divorced or separated (PR 1.62, 95% CI 1.13 to 2.33) were more likely to be infected with HPV. HIV infection (PR 1.22, 95% CI 1.01 to 1.47) was the only factor independently associated with infection with multiple types of HPV.
Conclusion: The prevalence of oncogenic HPV infection is high among this population and is associated with HIV serostatus and marital status. This community could benefit from enhanced sexually transmitted infection and HIV prevention interventions.
Statistics from Altmetric.com
Human papillomaviruses (HPVs), the causative agents of benign and malignant lesions of cutaneous and mucosal epithelial tissues,1 are a significant source of morbidity and mortality worldwide. Mucosal HPVs cause genital warts in men and women and have been linked to cancers of the cervix, vulva, vagina, anus and penis.2 HPVs are classified according to their oncogenic potential: low risk HPV types, which rarely cause precancerous cervical lesions and cervical cancer; and high risk (ie oncogenic) HPV types, which are the cause of virtually all cancers and precancerous intraepithelial lesions of the uterine cervix.3 4
In communities where women tend to marry as virgins and remain monogamous afterward, the sexual behaviour of men is a more important determinant in the transmission of oncogenic HPV and risk of cervical cancer.5 Therefore, factors that reduce the probability of HPV acquisition or transmission by men are likely to reduce the risk of HPV related disease among both men and women.6 The prevalence of oncogenic types of HPV in men has been associated with reported contact with sex workers,7 more sex partners7 8 and previous sexually transmitted infections (STIs),9 10 providing further evidence of the importance of sexual behaviour in the transmission.
Fishermen along Lake Victoria in Kisumu, Kenya, are high-income earners who migrate back and forth from their home villages away from their wives to work in the fishing industry. Women who come to these beaches to scale and trade fish reportedly exchange sex for fish or money (personal communication, Fisheries Department Kisumu, Kenya, 2003). The majority of the fishermen belong to an ethnic group that does not culturally practice circumcision—a factor that further predisposes them with increased risks of acquisition of HIV and certain STIs.11 We sought to determine the prevalence and determinants of HPV infection among the men in this fishing community.
METHODS
Design and study population
This cross-sectional study was designed to determine the prevalence of STI, including HPV, among fishermen in the Kisumu district, in order to guide the design and subsequent conduct of a trial evaluating the efficacy of a male microbicide in reducing acquisition of STI. Men who were at least 18 years old and worked in the fishing industry were eligible to participate. Beaches (ie clusters) were sampled with probability proportional to size and an equal percentage of men were selected from each cluster resulting in a self-weighted sample. A total of 250 men gave informed consent and were enrolled in the study. A detailed, structured, behavioural face-to-face interview gathered information on genital hygiene, migration patterns, sexual behaviour and interest in participating in microbicide research. Blood specimens were collected for HIV, herpes simplex virus (HSV) and syphilis serology, while urine samples were collected for Chlamydia trachomatis and Neisseria gonorrhoeae analysis. This study was approved by the ethical review committees of the Kenya Medical Research Institute and the University of Washington.
Genital swab sample collection
Genital specimens for HPV detection were collected by firmly rubbing over the external genital area with two cotton tipped plastic shafted swabs pre-wetted with sterile normal saline: one over the glans and corona sulcus of the penis, and the other over the shaft of the penis, the scrotum and the perianal region.12 Both swabs were immediately placed in the same plastic tube containing 1 ml Specimen Transport Medium (STM) (Qiagen, Valencia, CA, USA), transported to the laboratory in Kisumu, Kenya, and stored at −80°C. Specimens were shipped to the HPV laboratory in the Department of Pathology, University of Washington, Seattle, USA, for HPV DNA testing.
Laboratory assays
Genomic HPV DNA was isolated from the collected genital swabs and stored in STM using the QIAamp DNA mini kit (Qiagen, Valencia, CA, USA). Samples were first digested with 20 μg/mL proteinase K at 37°C for 2 hours. DNA was extracted from 400 μl of the proteinase K-digested samples using QIAamp blood DNA mini column following the manufacturer’s protocol. HPV positivity was determined first by polymerase chain reaction (PCR) amplification using HPV L1 consensus primers MY09/MY11/HMB01 and β-globin primers PC04/GH20, followed by dot blot hybridisation with generic HPV and β-globin probes.13 HPV positive samples were genotyped using the Roche linear array assay detecting 37 HPV types (6, 11, 16, 18, 26, 31, 33, 35, 39, 40, 42, 45, 51, 52, 53, 54, 55, 56, 58, 59, 61, 62, 64, 66, 67, 68, 69, 70, 71, 72, 73, 81, 82, 83, 84, CP6108, IS39).14
Serum was divided for three sets of tests. HIV positivity was first determined using two rapid tests: Determine HIV-1/2 (Abbott Laboratories, Illinois, USA) and Uni-Gold HIV (Trinity Biotech PLC, Bray, Ireland), and the results confirmed using the p24 ELISA kit Vironostica (Organo Tednika, the Netherlands). Syphilis infection was determined using Macro-vue rapid plasma reagin test (Benex limited, Ireland). The HSV infection was first determined using HerpeSelect HSV-2 ELISA (Focus Diagnostics, Cypress, CA, USA) and the results confirmed by western blot assays at the Virology Laboratory University of Washington. Finally the fast catch urine specimens were shipped to the centre for AIDS and STD laboratory, University of Washington, USA, for chlamydia and gonorrhoea testing using the APTIMA Combo 2 assay (Gen-Probe Inc, San Diego, CA, USA). All the assays’ procedures and results interpretations were done according to manufacturer’s instructions.
Statistical analyses
The overall and type-specific HPV prevalence was determined for the entire group of men. In bivariate analyses, prevalence ratios (PR) and 95% confidence intervals (CI) for the association between HPV infection and demographic or behavioural characteristics was calculated using Poisson regression and taking clustering by boat into account. In multivariate analyses, a manual backward elimination approach was utilised to reach the most parsimonious model, including factors that were independently associated with HPV infection at the significance level of p⩽0.05. All statistical analyses were performed using STATA v 9.2 (StataCorp LP, Texas, USA).
RESULTS
Characteristics of the study population
The mean age of the 250 men was 31.3 years (range 18–63 years) and the majority were married (69.2%), reported no condom use in the last two sexual acts (73.0%) and were not circumcised (92.8%). Approximately 13.9% of the married men were polygamous. Approximately 19.1% of all men spent 1–5 months living with their wife or regular partner, and 69.1% reported that at least one of their last two sexual partners was not their wife or any of their regular partners. Approximately 62.4% of all men reported travelling at least once in the last month, of whom 16.7% reported engaging in a sexual act at least once during the last travel. The prevalence of HIV-1 was 25.6% (95% CI 20.3 to 31.5), HSV-2 58.4% (95% CI 52.0 to 64.6), syphilis 9.6% (95% CI 6.3 to 14.0), chlamydia 3.2% (95% CI 1.4 to 6.2) and gonorrheoa 1.2% (95% CI 0.3 to 3.5).
Prevalence of HPV infection
All the 250 genital swab specimens were positive for the β-globin gene and were considered sufficient for HPV DNA analysis. Genital swab specimens from 144 of 250 (57.6%, 95% CI 51.2 to 63.8) men contained detectable HPV DNA (table 1). The prevalence of oncogenic HPV types was 42.4%. The most prevalent oncogenic HPV types were HPV-16 (12.4%), HPV-35 (10%), HPV-52 (9.6%) and HPV-18 (6.8%). The overall prevalence of low-risk HPV types was 43.2%, with HPV-62 (11.2%), HPV-6 (9.6%) and HPV-70 (8.4%) being the most prevalent types.
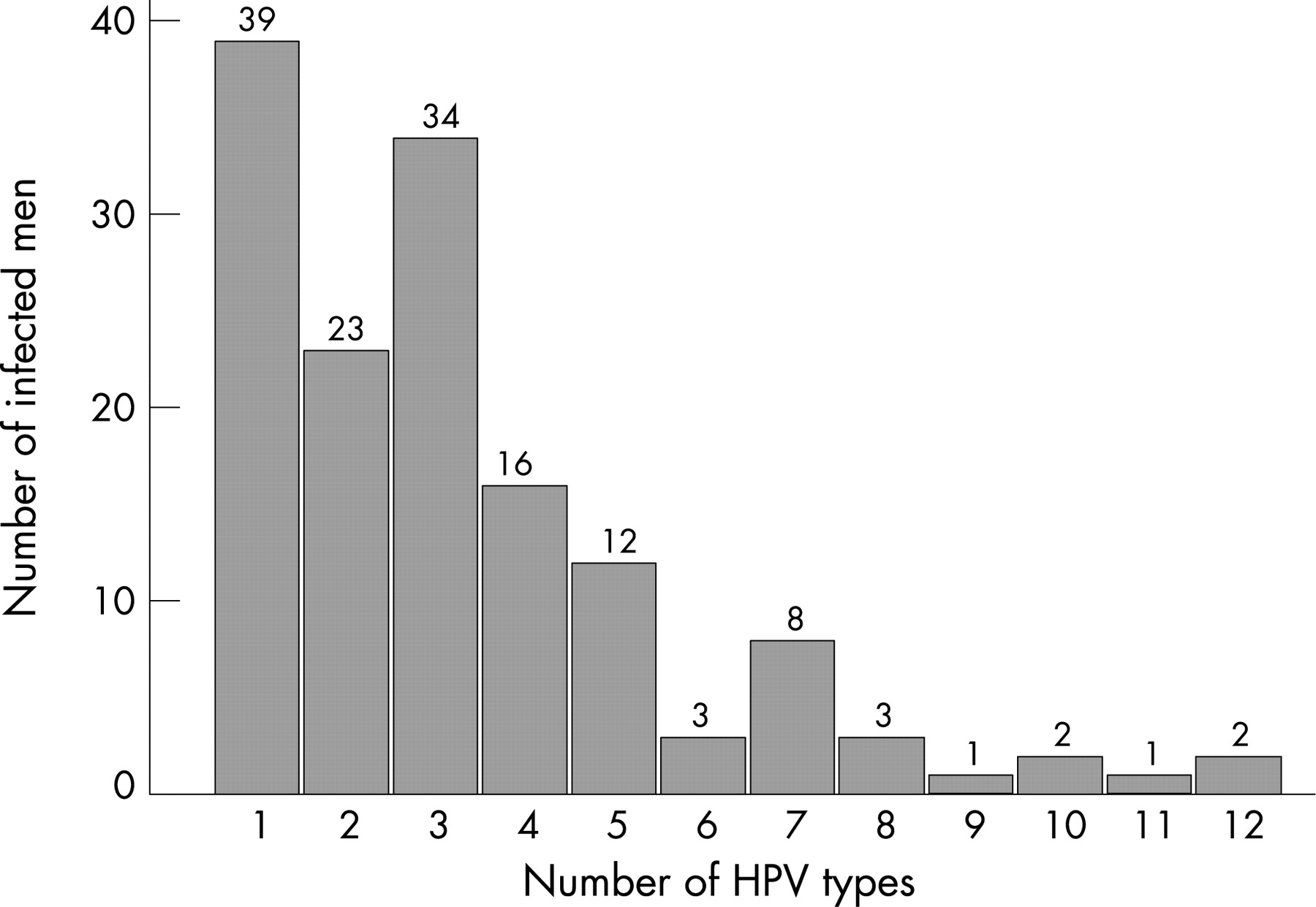
Of the 144 HPV positive men, 105 (72.9%) were infected with more than one HPV type (table 1). HPV-16 (28.6%) was the most common type among men infected with multiple HPV types. Among HPV positive men, 32 (22.2%) were infected with five or more different HPV types, including two men infected with 10, one man infected with 11 and two men infected with 12 different HPV types (fig 1).

{kind=link}
Demographic and sexual behaviour associated with HPV infection
In bivariate analyses, HIV positive men were more likely to be infected with HPV than HIV negative men (PR 1.41, 95% CI 1.16 to 1.71) (table 2). Furthermore, among HPV positive men, those who were infected with HIV were more likely to be infected with multiple HPV types than those who were HIV negative (PR 1.22, 95% CI 1.03 to 1.44).
In multivariate analyses (table 3), HIV positive men were almost 50% more likely to be infected with HPV compared to HIV negative men (PR 1.49, 95% CI 1.19 to 1.86). Men aged 31–40 years were less likely to be infected with HPV (PR 0.60, 95% CI 0.41 to 0.89) compared to men aged 21–25 years; the separated or divorced men showed a 62% increase in likelihood of HPV infection compared to currently married men (PR 1.62, 95% CI 1.13 to 2.33). Finally, among HPV positive men, those who were infected with HIV showed a 22% increase in likelihood of infection with multiple HPV types compared to those who were HIV seronegative (PR 1.22, 95% CI 1.01 to 1.47).
DISCUSSION
To our knowledge, this is the first study on prevalence of HPV infection among high-risk men in Kenya. The prevalence of HPV infection in sexually active men in this fishing industry was 57.6%. Infection with more than one HPV type was also very common both as an absolute percentage (42% of fishermen) and as a percentage of all HPV positive men (72.9%). The percentage infected with multiple types was higher among HIV positive men. This study shows one of the highest HPV prevalence estimates for a heterosexual male population reported to date. Examples of previous studies of men from both developed and developing countries reported HPV prevalence estimates of 39.4% among HIV infected men attending a special HIV clinic in the Netherlands, 41.6% of whom were infected with multiple HPV types;15 42.7% in sexually active populations in Mexico with multiple infections detected in 26.8% subjects;16 18.1% among healthy male volunteers in Japan,17 and 45% in men attending a STD clinic in Denmark with 7% having multiple infection.18
HPV-16 was the most prevalent oncogenic type in our study, followed by HPV-35, HPV-52 and HPV-18. This is consistent with the results of most studies conducted in both random and selected male populations, which have shown HPV-16 to be the most prevalent type;10 18 a study of men attending a special HIV clinic in the Netherlands reported HPV-52 to be the most prevalent type.15
We identified independent risk factors for HPV infection consistent with previous reports and some unique factors. Men aged 31–40 years were less likely to test positive for HPV compared to men aged 21–25 years and this was not shown for any other age category. A decreasing prevalence of HPV with age has been found in several female populations,18 19 and in other studies in male populations18 it has been suggested that this age pattern in women and men is at least partly explained by an acquired immunity to HPV that is strengthened over time because of repeated exposure.18
Infection with HIV was associated with increased likelihood of HPV infection and of infection with multiple HPV types. An increase in HPV positivity has been reported for both HIV-seropositive women20 and men.21 It is not surprising that individuals infected with HIV have a high prevalence of anogenital infection with HPV as well given the overlap in risk factors for both. Before the implementation of highly active antiretroviral therapy (HAART), nearly all HIV positive men who had sex with men were shown to have anal HPV infection, usually with multiple HPV types. 22 In some of these cases HPV was detected in the absence of sexual risk factors—for example, anal HPV infection in HIV positive women and men with no history of receptive anal intercourse23—suggesting that HPV may also be acquired at a given site through spread from other genital sites or through fingers or fomites.22 24 25 Recent evidence suggests that about half the HPV infections in HIV positive women can be accounted for by recent sexual acquisition, whereas the other half most likely represents re-activation of previously acquired HPV types.25
Several mechanisms may explain the increased prevalence of HPV associated disease in HIV positive individuals. These include direct interactions between the two viruses, attenuated immune response and chromosomal instability.26 HIV may interact with HPV at the molecular level through the action of the HIV-1 tat protein, which has been shown to transactivate the HPV long control region in vitro, leading to increased expression of the HPV E6 and E7 oncogenes.27 However, there is no evidence for permanent infection of anogenital or oral epithelium where HPV resides, and no evidence for coinfection in HPV infected keratinocytes. It is therefore unlikely that the two viruses interact directly in a sustained manner that would be expected to modify the outcome of HPV associated disease.26 Progressively lower CD4+ level has been shown to reflect an increased detection of HPV types in the anus and cervix. Moreover, HPV-specific immunity may not recover fully after immune response is restored, which may explain the relatively limited beneficial effect of HAART on HPV associated lesions.26 Immune response has been shown to have a limited role in protection against the progression of high-grade lesions to invasive cancer. If true, then other non-immune factors must be operative. Evidence now suggests that progression to cancer may reflect genetic damage in the lesions. At advanced stages of disease pathogenesis, these genetic changes render the lesion resistant to any immune reconstitution that may be brought about by HAART.26
Although this study shows a possible role of being separated or divorced as a determinant of HPV infection among fishermen, we cannot rule out the possibility of either a chance finding or uncontrolled or partially controlled confounding. For instance, we could hypothesise that the separated or divorced men engage in casual sexual activity more frequently than married men. This repeated sexual exposure to one or multiple casual partners with HPV infection over several months or years could pose a greater cumulative risk of acquiring HPV than in men who are married with consistent sexual encounters with one woman.
Some other studies among men have identified other independent factors associated with HPV infection that we did not either measure or find to be significant in this study, including circumcision status,6 28 condom use,9 type of sexual partner (casual partners and commercial sex workers),16 frequency of sexual activity, genital washing after sexual activity and perceptions about partners’ STI status. The cross-sectional nature of this study, relatively small sample size, inadequate assessment of sexual behaviours and condom use could partly explain the observed lack of association between HPV infection and the above listed independent factors.
In conclusion, the high prevalence of both oncogenic HPV (42.4%) and of HIV (25.6%) among the geographically defined sexually active men in fishing communities along the shores of Lake Victoria in the Kisumu District of Kenya suggests the need for interventions to reduce the spread of these viruses. In addition, since the annual rate of cervical cancer in Kenya is high (28.7/100,000 women),29 young adolescent women in this community would be a good target group for the prophylactic HPV vaccine that targets HPV-16 and HPV-18.
Acknowledgments
We wish to acknowledge the Director KEMRI, Director CMR, all the staff of the Fishermen study, the couple’s intervention study and the Family AIDS Care and Educational Services in Kisumu, Kenya, and the University of Washington pathology Laboratory, Seattle, USA.
REFERENCES
Footnotes
MON performed laboratory analyses and was lead author for the paper; EB and KKH conceived and designed the study; LK and AR analysed and interpreted the data; QF performed laboratory analyses; ZK supervised the conduct of the trial and data acquisition; all authors contributed to the write up.
Funding: The study was funded, in part, by the National Institute of Allergy and Infectious Disease UW STI-TM CRC Grant U19-AI31448. Ng’ayo was supported by the International AIDS and Research Training Grant from the Fogarty Institute of the NIH.
Competing interests: None.