Article Text

Abstract
Objectives This study aimed to obtain nationally representative estimates of HIV and syphilis prevalence and coverage of preventive antenatal services in pregnant women in Ecuador, in order to develop a national strategy for the elimination of mother-to-child transmission of HIV and syphilis.
Methods A national probability sample of 5988 women presenting for delivery or miscarriage services was selected from 15 healthcare facilities during 2011–2012, using a two-stage cluster sample technique. Biological specimens were collected and an interview and review of medical records were performed. Agreement between these last two sources was measured. Estimates were adjusted for the sampling design.
Results Estimated national HIV prevalence (0.60%) was higher than confirmed syphilis infection prevalence (0.25%). In the coastal region, HIV prevalence (1.13%) exceeded the threshold that defines a generalised epidemic and syphilis prevalence reached 0.37%. An estimated 5.9% of women did not use antenatal care services while 73.0% completed at least four consultations. HIV testing coverage (89.9%) was higher than for syphilis (71.6%). Agreement between medical records and interviews was mostly moderate (0.40–0.75). Important variables were frequently not recorded, such as timing of syphilis testing, which was not recorded in 49.6%.
Conclusions The concentration of HIV and syphilis infections in the coastal region of Ecuador highlights the need for intensified prevention and a response tailored to local epidemic conditions. Major challenges for the elimination initiative include achieving universal, early access to antenatal care, improving coverage of HIV and syphilis testing, and improving the quality of medical records to support progress monitoring.
- HIV
- SYPHILIS
- PREGNANCY
Statistics from Altmetric.com
Introduction
Mother-to-child transmission of HIV and syphilis infections continues to be a major public health challenge globally.1 ,2 In Latin America and the Caribbean (LAC), an estimated 4700 children were infected with HIV in 2010, the majority of these through mother-to-child transmission; between 164 000 and 344 000 infants are born annually with congenital syphilis.3 Both infections are a preventable cause of morbidity/mortality among newborns.3
In 2009, the Pan American Health Organization launched a regional initiative aiming to eliminate mother-to-child transmission of HIV and congenital syphilis by 2015.4 Monitoring trends in infection prevalence and in coverage of diagnostic and prophylactic interventions in the context of antenatal care (ANC) is an essential component of the elimination strategy.
Like most LAC countries, Ecuador bases its public health disease surveillance system mainly on disease case reporting. A rising trend has been observed in HIV case reports nationally from 1070 in 2005 to 4041 in 2010 (Ecuadorian Ministry of Public Health, 2011). Syphilis case reports in pregnant women show declining rates from 0.85 per 1000 pregnant women in 2008 to 0.66 per 1000 pregnant women in 2010 (Ecuadorian Ministry of Public Health, 2011), equivalent to a maternal syphilis prevalence lower than 0.1%.
In Ecuador, approximately 357 000 women gave birth in 2011 (Ecuadorian Ministry of Public Health, 2011). In 2007–2012 the estimated percentage of women who attended ANC services at least once was 84%, while institutional delivery was estimated at 85%.5 Programmatic data from clinics testing antenatal women, based on collection and reporting of the results of diagnostic testing in pregnant women, are only available for HIV but not for syphilis surveillance. They suggest a rising trend in HIV prevalence among pregnant women, from 0.12% in 20086 to 0.24% in 2011 nationally (p<0.05), with an estimated number of 275 000 pregnant women tested in 2011 (Ecuadorian Ministry of Public Health, 2011).
Case report data may be limited due to under-reporting, delays, and low quality of reporting.7 Monitoring HIV prevalence among pregnant women based on programmatic data from antenatal clinics may also be subject to bias.8 In Ecuador, possible duplicate registrations (women tested more than once during pregnancy) and incomplete coverage of antenatal services are among the main limitations, as programmatic data do not include private health providers and other public providers besides the Ministry of Health, which covered 36.1% of women attending ANC services in 2004.9 The objectives of this study were to obtain robust national HIV and syphilis prevalence estimates in pregnant women in Ecuador, as well as to describe the characteristics of ANC associated with the early detection of both infections.10
Methods
Sample
A two-stage cluster sample technique was used. Fifteen healthcare facilities were selected from a Ministry of Health registry of live births and miscarriages, with the probability of selection proportional to the number of live births and miscarriages in 2008. To ensure recruitment feasibility, we excluded from the sampling frame facilities with fewer than 400 deliveries and miscarriages. Eligible facilities represented 75% of deliveries and miscarriages nationally in 2008. Before the selection, eligible facilities were arranged according to region and province in order to improve geographical representation. The resultant sample included facilities in Ecuador's three major geographic regions: eight facilities located in the coastal region, six in the highlands, and one in the Amazon basin. Three private facilities were among those selected. Nine (60%) were secondary level facilities (three basic hospitals and six general hospitals); five (33%) were specialised mother and child care hospitals (tertiary level facilities); and one was a national tertiary referral hospital.
In the second stage of sampling, all eligible women at the selected facilities were invited to participate in the study until the target sample size was reached. Eligible study subjects were women presenting for delivery or miscarriage services up to 48 h of post partum or miscarriage. In many Latin American settings the proportion of births attended by skilled health staff is usually high, while women frequently do not attend ANC services.11 Therefore, to minimise potential selection biases, our study population comprised women undergoing delivery or miscarriage instead of women seeking ANC. This approach also prevents duplicate/multiple recruitment during successive ANC visits, and facilitates recruitment thanks to longer lengths of stay.11
We aimed to recruit a total of 6000 women, with targets at each facility set proportional to size. The study was powered to estimate syphilis and HIV infection prevalence with ≤2% error at the 95% confidence level, assuming prevalences of 0.2% for HIV and 2.0% for syphilis, population size of 158 465 women presenting for delivery or miscarriage services, and a design effect of 1.25 due to the multi-stage sampling design.
The study protocol was approved by the research ethics committee of the Central University of Ecuador (Ethics committee: Bioethics committee. Cobi-UCE. Federalwide Assurance FWA00002482 IEC IORG0001932 IRB00002438). Informed consent was required for women to participate. The consent form employed included the specific form of the Ministry of Health for HIV testing. Parental permission for minors to participate was waived by the ethics committee.
Data collection
Study teams comprised health professionals trained on study procedures, including a supervisor, interviewers, and laboratory personnel. Participants received pre-test counselling and provided blood specimens. HIV counselling and rapid testing were performed before birth whenever possible, due to the potential benefit of receiving intrapartum antiretroviral prophylaxis. Only when the participant was admitted during the expulsion period, with no time to be screened, was rapid testing performed after birth. Participants then completed a face-to-face survey questionnaire, which explored sociodemographic variables and characteristics of ANC. Information about ANC was also collected from medical records. Medical records in maternity units of the Ministry of Health are completed based on the information contained in ANC cards, which have been previously filled out by health staff of ANC centres and are carried by women to delivery services. Some facilities had computerised medical records which allowed access to information across the care continuum. The completeness of medical records was assessed as a measure of the quality of the registry.
Sociodemographic variables included age, nationality, place of birth, ethnic group, educational level, occupation, and household income. ANC characteristics included number and timing of visits, HIV and syphilis testing, timing of testing, and access to HIV and syphilis information. Indicators of access and utilisation of care during pregnancy and quality of care were those agreed in the regional initiative for the elimination of mother-to-child transmission of HIV and congenital syphilis,10 where at least four visits per pregnancy, early ANC consultation, and early syphilis screening before 20 weeks gestational age are recommended. Pregnancy in adolescence was classifed as 10–14 years of age and late adolescence (15–19 years of age).12
Study participants with confirmed HIV or syphilis infection, and their newborns, received free care and treatment following national guidelines, including referral to Ministry of Health specialised HIV care and treatment facilities as necessary. Pre- and post-test counselling, testing, and treatment were integrated into the routine process of medical care over the course of the study.
Stringent data collection, transfer and storage procedures were implemented, including security features for controlled access to project data; a tracking system for data forms, activities, and study samples; independent double data entry of data forms and laboratory results; date and time stamping of all data records with electronic signatures; and audit trails to track all changes made to data records. Database management was performed using OpenClinica software, V.3.0.4.
Laboratory procedures
Fourth generation HIV rapid tests (Determine) and rapid plasma reagin (RPR, Wama Diagnostica) or Venereal Disease Research Laboratory (VDRL, Wama Diagnostica) tests for syphilis infection were conducted at the participating health facilities. Reactive samples were sent to the National Institute of Hygiene and Tropical Medicine's (IHTM) regional reference laboratories in Quito, Guayaquil, or Cuenca for confirmatory testing by western blot and fluorescent treponemal antibody absorbed (FTA-ABS) for HIV and syphilis, respectively, following national diagnostic algorithms. Confirmed syphilis infection was defined as reactive RPR/VDRL and FTA-ABS test results. HIV rapid test and RPR/VDRL results were provided during the initial attendance. Participants were scheduled for a follow-up visit for confirmatory results. Ten per cent of samples non-reactive for HIV and syphilis were re-tested at IHTM for external quality control.
Statistical analysis
Univariate proportions of sociodemographic characteristics, infection prevalence, and antenatal services received were estimated along with 95% CIs. The sample was self-weighted within each of the primary sampling units (ie, healthcare facilities); however, the sample as a whole was not equiprobabilistic. Consequently, the individual-level records were weighted by the inverse of each woman's selection probability. Analysis was conducted in EPIDAT 4.1,13 a specialised software that takes into account both the weights and the complex nature of the sample design (two stage cluster sampling). κ values assessed the agreement between medical records and self-report interview data. κ levels below 0.40 indicate poor agreement, between 0.40 and 0.75 moderate agreement, and above 0.75 high agreement.
Women presenting for miscarriage services were excluded from the analysis of number of visits per pregnancy.
Results
Sample and sociodemographic characteristics
Between August 2011 and February 2012, 5988 women participated in the study, with an average recruitment period of 4 months at each health facility. Women admitted for miscarriage comprised 8.2% of the sample. Information from surveys and medical records were obtained for 97.4% and 96.6%, respectively, of enrolled women. The mean age of the participants was 24.9 years (95% CI 24.1 to 25.8). Approximately 25% of women were adolescents (under 20 years of age); 0.9% aged 10–14 and 23.7% aged 15–19. Half of the enrolled women were from the coastal region (51.0%), with 38.4% from the highlands and relatively few from the Amazon basin (9.0%). The most frequently self-reported ethnicity was mixed (mestizo) (79.5%). An estimated 54.9% reported completing secondary education and few (17.7%) post-secondary education. Household income was below the Ecuadorian minimum wage in 74.0%. The most common occupation was housework (70.8%) and few participants were employed (9.7%) (table 1).
Sociodemographic characteristics of women presenting for delivery or miscarriage, Ecuador, 2011–2012
HIV and syphilis prevalence
Samples for HIV and syphilis testing were obtained for 98.7% and 98.1%, respectively, of enrolled women. HIV infection was detected in 46 participants and confirmed syphilis infection in 21 participants. Estimated population prevalence was 0.60% for HIV and 0.25% for confirmed syphilis infection. All of the HIV cases and most syphilis cases identified were found in the coastal region (table 2). One out of 46 HIV seropositive women was determined to be co-infected with confirmed syphilis infection (weighted estimate 0.01%, 95% CI −0.01% to 0.03%). No cases of confirmed syphilis infection were found among women undergoing miscarriage.
Infection prevalence among women presenting for delivery or miscarriage, Ecuador, 2011–2012
ANC services
According to medical records, 5.9% of the recruited women did not use ANC services whereas 73.0% completed at least four healthcare consultations during their pregnancy. Early antenatal coverage, before 20 weeks gestational age, was 73.4%. The proportion of pregnant women tested for HIV (89.9%) was substantially higher than the proportion tested for syphilis (71.6%). Less than half of women (42.1%) were screened for HIV in the first trimester of pregnancy. Early syphilis testing was also low (42.9%).
The percentage of women who reported using ANC services in face-to-face survey was higher than that registered in medical records. Reported HIV and syphilis testing was lower, with the highest differences observed for syphilis. Only 36.2% of women reported having been tested for syphilis during pregnancy and 27.7% having been tested before 20 weeks.
Nearly three quarters of participants (74.3%) received HIV information during pregnancy, while those who received information about syphilis was lower (24.7%). Most women attended public health services for ANC (83.2%) while use of private services was pretty low (27.6%).
Agreement between medical records and interview data was moderate for most of the indicators of access and quality of ANC (table 3).
Characteristics of antenatal care (ANC), Ecuador, 2011–2012
Most (85.5%) of HIV seropositive women had evidence in their medical records of HIV testing during pregnancy; among those tested, 84.8% had a positive result recorded. In participants with confirmed syphilis infection, testing during pregnancy was lower (66.1%), and among those tested, 55.3% had a syphilis positive result. No treatment during pregnancy was recorded in 11.6% and 42.9%, respectively, of women with confirmed HIV and syphilis infection.
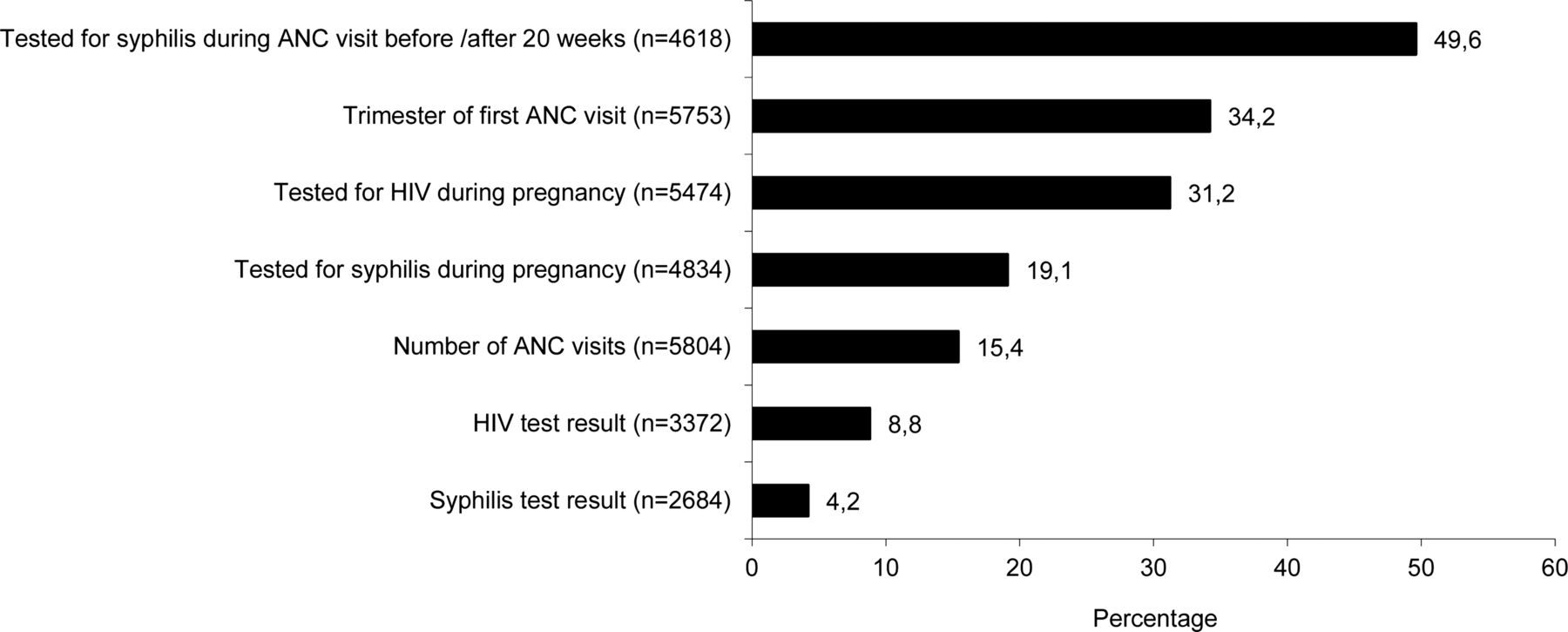
Medical records were found to be frequently incomplete for the selected indicators which are part of the essential dataset of the national perinatal clinical history. Half of the participants (49.6%) had no data entered regarding the gestational age when the syphilis test was performed. Around a third (34.2%) had no information concerning the trimester of first ANC visit and regarding HIV testing (31.2%) (figure 1).

{kind=link}
Percentage of medical records with incomplete data on antenatal care (ANC) indicators, Ecuador, 2011–2012.
Discussion
Prevalence studies and behavioural research in specific populations are recommended for a better understanding of the HIV and STI epidemics.14 This is the first study of HIV and syphilis infection prevalence in a nationally representative sample of pregnant women in Ecuador. The HIV and syphilis prevalence estimates found in this study are higher than those indicated by programmatic and case report data, pointing to possible limitations in the latter surveillance systems.
HIV prevalence estimates among pregnant women are often viewed as a proxy for the general population.14 Previously available information defined the Ecuadorian HIV epidemic as being concentrated in high risk groups, mainly in men who have sex with men.15–17 However, the estimated HIV prevalence in pregnant women from the coastal region is slightly over 1% in our study, a threshold defined by UNAIDS as indicative of a ‘generalised epidemic’,14 meaning that there is a substantial contribution from sexual behaviour in the general population to overall transmission. Because the contribution of high risk groups to the HIV epidemic in Ecuadorian coastal region appears considerable,16 this scenario would be characterised as a ‘mixed’ epidemic by some authors.18
We found syphilis to be less prevalent than HIV in women giving birth or suffering miscarriage, which concurs with data from national case reporting. This is an uncommon finding in the Americas, only observed previously in the Dominican Republic, Trinidad and Tobago, and Guyana.3 The estimated syphilis prevalence in pregnant women in Ecuador (0.25%) is below the estimated median for the region of the Americas (0.84%)19 and is one of the lowest within LAC, where around half of countries reported prevalences over 1% in 2010.3
Syphilis testing coverage was found to be below regional goals,4 with almost 30% of women not having access to a test during their pregnancy according to medical records. Interestingly, the results show a higher HIV testing coverage. Regrettably, this reflects a more limited focus on prevention of congenital syphilis relative to the greater resources and attention on prevention of mother-to-child transmission of HIV, as has been noted at the global level.18 Observed indicators of HIV and syphilis treatment in women who were already found to be seropositive during pregnancy, lower than 100%, indicate missed opportunities for prevention of mother-to-child transmission.
Our analysis revealed weaknesses in maternal antenatal medical record keeping. Timing of syphilis testing was frequently missing in medical records, despite the importance of gestational age for screening and treatment, as mother-to-child transmission most commonly takes place after 4 months of gestation.20
We found moderate to low agreement when comparing the information from medical records and interviews. Self-reported HIV and syphilis screening coverage were lower than as indicated by medical records and the proportions of women who reported having received information about HIV and syphilis were lower than testing coverage rates. These findings may suggest non-compliance with national regulations that require STI counselling and informed consent before HIV testing, which has already been reported in several countries.21 ,22
Our study is subject to some limitations. The sampling design did not allow exploration of geographical differences in our main outcomes, as the sample was only large enough to obtain sub-estimates of HIV and syphilis infection for the coastal region. However, the concentration of HIV and syphilis cases in the coastal region suggests lower prevalences in the rest of the country. More information is needed to clarify the factors associated with within-country regional differences, which have been observed in other countries such as in neighbouring Peru.23 There are some limitations concerning representativeness. This study is not representative of women who do not seek skilled healthcare for delivery or miscarriage, a proportion estimated at 15% in Ecuador.9 Health facilities with a patient volume of fewer than 400 deliveries and miscarriages per year, which are more frequently found in rural areas, were excluded from the sample frame. The study is therefore less representative of rural areas, where access to services may be more limited.24 HIV infected pregnant women who know their status are usually referred to higher level facilities for delivery, which frequently have a higher number of deliveries per year. Excluding the smallest facilities could have resulted overestimation or underestimation of HIV prevalence. However, since they represented only 25% of deliveries and miscarriages nationally, the potential impact on HIV prevalence estimate would be low. Moreover, when calculating separate estimates for the subsample comprising the three facilities with the smallest volume (up to 800) of deliveries and miscarriages per year (subsample 1, S1) versus the rest with higher volumes (subsample 2, S2), we found no important differences in HIV prevalence estimates (S1: 0.61, 95% CI −0.58 to 1.80; S2: 0.58, 95% CI 0.09 to 1.08). Information about eligible women who refused to participate was not systematically collected, although due to the inclusion of the study procedures on routine care and based on reports from study sites coordinators we estimate a low refusal rate.
Despite these limitations, this report represents a relevant contribution to the characterisation of HIV and syphilis epidemics in Ecuador. Our findings highlight the concentration of both infections in the coastal region, suggesting the appropriateness of implementing differential approaches in the response to the epidemics targeting prioritised areas. ANC plays an important role as a platform for HIV and syphilis testing and provision of preventive services. There is an urgent need for improving interventions for preventing mother-to-child transmission of HIV and syphilis. Major challenges include reaching universal coverage of ANC, promoting early access to health services, and ensuring HIV and syphilis testing for all those who access such services. Improving medical record keeping is also a key component as it supports progress monitoring.
Key messages
-
HIV and syphilis prevalence in pregnant women in Ecuador is highest in the coastal region.
-
A response tailored to local epidemic conditions is needed.
-
Promoting early access to antenatal care services and improving coverage of HIV and syphilis testing during pregnancy should be a priority.
Acknowledgments
We would like to express our sincere gratitude to all health professionals in study sites and laboratory staff who participated on data collection and analysis.
References
Footnotes
-
Handling editor Jackie A Cassell
-
Contributors AS, JJ, ST and MC contributed to development of the study design, instruments and study procedures. MG, CY and JC developed the data management plan. WC trained the study team. WC, AS, MC, EC, ML, CM, CY and JC coordinated data collection. JJ and LS designed the sample and LS conducted data analysis. AS conceived and drafted the manuscript. All authors helped to conceptualise ideas, interpret findings, and review drafts of the manuscript.
-
Funding This work was supported by funds from the Pan American Health Organization/Latin American Center for Perinatology and Human Development (PAHO/CLAP), the United Nations Children's Fund (UNICEF), and the Ecuadorian Ministry of Health.
-
Disclaimer The findings and conclusions in this paper are those of the authors and do not necessarily represent those of the Pan American Health Organization.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Research Ethics Committee of the Central University of Ecuador (Ethics committee: Bioethics committee. Cobi-UCE. Federalwide Assurance FWA00002482 IEC IORG0001932 IRB00002438).
-
Provenance and peer review Not commissioned; externally peer reviewed.