Article Text

Abstract
Objective: To measure the burden of infection with herpes simplex type 1 (HSV-1) and herpes simplex type 2 (HSV-2) in the general population of England and Wales and to assess temporal changes in the incidence of HSV-1 infection in childhood.
Methods: 4930 residual blood samples taken from people aged 0–69 years and submitted to 15 public health laboratories in England and Wales between January 1994 and June 1995, and 500 samples taken from people aged 10–14 years between November 1986 and December 1987, were screened for IgG antibody to HSV-1 and HSV-2 using type specific ELISA assays.
Results: The prevalence of antibody to HSV-1 in 10–14 year olds declined from 34% in samples collected in 1986–7 to 24% in samples collected in 1994–5 (p<0.001). HSV-1 antibody prevalence in adults increased with age and was higher in females than males, reaching 54% in females aged 25–30 years in 1994–5. In samples collected in 1994–5 from people aged 16–69 years HSV-2 antibody was detected in sera from 3.3% of men and 5.1% of women.
Conclusions: The incidence of HSV-1 infection in childhood is falling in England and Wales. The prevalence of HSV-2 infection in the general population is low, with the rate of infection significantly lower than that described for the general population in the United States and developing countries. The falling rate of HSV-1 infection in childhood may be one factor contributing to the increasing incidence of genital HSV-1 infection.
- herpes simplex virus
- genital herpes
- prevalence
Statistics from Altmetric.com
Introduction
The two herpes simplex viruses (HSV-1 and HSV-2) cause ulcerative infections of the oral and genital mucosa in humans. Primary infection is followed by seroconversion and the establishment of latent infection in nerve ganglia. Recurrent infections occur periodically due to virus reactivation. Classically, HSV-1 is responsible for oral infections and is acquired mainly in childhood. HSV-2 infects the genital tract through sexual contact.1 An important feature of HSV mucocutaneous infection is that it is often subclinical.2
Genital herpes has become more common in England and Wales in recent years—approximately 15 000 cases of first episode genital herpes have been seen at genitourinary medicine clinics each year since 1993. Within the past 20 years an increasing proportion of genital herpes cases in the United Kingdom has been caused by HSV-1.3 The reasons for this change remain unclear but two factors that may have contributed are “changes in behaviour” and a changing pattern of HSV-1 infection.
The recent development of reliable HSV type specific antibody assays has provided the means to identify past infection with a given HSV type, regardless of whether it was clinically apparent or not. To date these assays have been used largely in epidemiological studies, particularly within populations at high risk for genital herpes such as genitourinary medicine (GUM) clinic attenders.4, 5 Two studies in the United Kingdom have used validated HSV type specific serology to test cohorts that are more representative of the general population. These found an HSV-2 seroprevalence of 10.4% and 7.6% in London antenatal clinic attenders and blood donors respectively,6, 7 while 22.7% of GUM clinic attenders in the latter study were HSV-2 positive.
Methods
SAMPLES
This study used a total of 5430 serum samples, 4930 of which were from people aged 0–69 years collected between January 1994 and June 1995 and 500 from children aged 10–14 years collected between November 1986 and December 1987. All were anonymised residues of specimens submitted for microbiological or biochemical testing to 15 public health laboratories in England and Wales, collected as part of the PHLS serological surveillance programme.8, 9 Samples from immunocompromised people and those submitted for testing for antibody to HIV and hepatitis B were excluded. Ninety eight per cent of sera were collected outside London. Sera from children aged 0–16 years were collected in all participating laboratories, whereas sera from adults were collected predominantly in four laboratories (Ashford, Cambridge, Manchester, and Preston). In total, 2607 sera were from males and 2823 from females.
LABORATORY METHODS
Type specific antibodies to HSV-1 and HSV-2 were determined using monoclonal antibody blocking ELISAs. These are a direct modification of the validated monoclonal antibody blocking radioimmunoassays described by Slomka et al10 and full details of the assays will be reported elsewhere (manuscript submitted).11 Briefly, wells of microtitre plates (Greiner) were coated overnight at 4°C with either HSV-1 or HSV-2 infected cell lysate10 as appropriate, diluted 1:25 in phosphate buffered saline (PBS). Wells of HSV-2 coated plates were further incubated with detergent (1.5% Triton X-100 and 0.5% Nonidet P40 in PBS) for 30 minutes at room temperature. After incubating for 2 hours at 37°C with PBS containing 10% fetal calf serum (FCS), wells of coated plates were incubated successively for 1 hour at 37°C with the following in PBS containing 10% FCS and 0.2% Tween 20 (T20): a 1:4 dilution of test serum; a 1:16 000 dilution of HSV-1 or HSV-2 specific Mab as appropriate; a 1:1000 dilution of horse radish peroxidase (HRPO) conjugated anti-mouse Mab. Wells were washed three times between each stage with PBS containing 0.05%T20. Plates were incubated with a tetramethyl benzidine substrate (TMB) at room temperature in the dark. The reaction was stopped after 20 minutes by the addition of 2M H2SO4. The optical density of each well was then measured immediately at 450 nm (620 nm reference) (OD450/620) and the percentage blocking of each serum calculated by comparison with diluent controls and the mean OD450/620 of four wells containing a positive control serum.
TESTING STRATEGY
Of the sera collected in 1994–5, 1583 samples from 0–15 year olds were tested for antibody to HSV-1 only; 1500 samples from 16–30 year olds were tested for antibody to HSV-1 and HSV-2; and 1847 samples from 31–69 year olds were tested for antibody to HSV-2 only. All 500 children's sera collected in 1986–7 were tested for antibody to HSV-1 only.
Sera were considered positive for HSV-1 antibody if blocking values were ≥20%; equivocal for blocking values of 0–19%; and negative if the blocking was <0%. The positive cut off was set at the mean plus three standard deviations of 127 children's sera (age range 5–14 years) negative for antibody to HSV. The cut-offs were supported by mixture model analysis12 of results for all 3583 sera tested for HSV-1 antibody. To confirm these cut offs a 587 sample subset (including all equivocal sera and representative samples of positive and negative sera) were screened for total antibody to HSV using a commercial ELISA kit (Behring Enzygnost, Behringwerke AG, Marburg, Germany).
Sera were considered positive for HSV-2 antibody if they gave a blocking value ≥50%, equivocal for blocking values of 30–49% and negative if the blocking was <30%. The positive cut off was set at the mean plus three standard deviations of 213 sera from children aged 5–14 years (considered negative for antibody to HSV-2).13 To confirm the sensitivity and specificity of the testing strategy a representative subset of 100 sera of the 3347 screened for HSV-2 antibody were tested by western blot14 for HSV-2 specific IgG antibody. No mixture model analysis was performed because of the small proportion of positive samples in the population screened.
STATISTICAL METHODS
Agreement between assays was assessed using Cohen's kappa statistic, with 95% confidence intervals. Prevalence by sex was compared using the χ2 test and age trends were assessed using the χ2 test for trend. Exact confidence intervals for prevalence were calculated using the binomial distribution.
Results
ASSAY EVALUATION
In the absence of a suitable gold standard assay for determining HSV-1 specific IgG levels in sera at the time of testing, the Behring ELISA which measures total HSV antibody was used to confirm the cut offs chosen using sera without HSV-2 antibody. There was good agreement between the HSV-1 antibody blocking ELISA and the Behring ELISA in samples from both children and adults, which is supported by kappa analysis of the results (table 1). In those sera tested by both assays, there was agreement on 375 (94%) of the 401 sera that gave unequivocal results in the blocking assay. The Behring ELISA (for total HSV IgG) gave a positive result for 21 of 160 (13%) sera from adults that were negative by the in house assay (table 1). Two of these 21 samples were positive for antibody to HSV-2. Equivocal results were obtained for 186 of 3583 sera (5%) tested using the HSV-1 antibody blocking ELISA. These sera were categorised as positive or negative for HSV-1 antibody according to their result in the Behring ELISA; 74% were positive.
Comparison of results that were unequivocal by HSV-1 antibody blocking ELISA with Behring ELISA
The HSV-2 antibody blocking ELISA compared well with western blot. Of a total of 100 sera tested by both methods, 98 gave concordant results: the two discrepant sera were positive by the antibody blocking ELISA and negative by western blot.
HSV-1 ANTIBODY PREVALENCE
Prevalence in 1994–5
The prevalence of antibody by age and sex in sera collected in 1994–5 is shown in figure 1. Of infants aged less than 1 year 47% had detectable antibody to HSV-1, most probably attributable to maternally acquired antibody. Prevalence in children aged 1–15 years was 24.5% (363/1484) with no significant difference between sexes (p=0.45), or age trend (p=0.091). In adults prevalence increased with age and was higher in females than males (p<0.001), reaching 54% in females aged 25–30 years.

Age specific prevalence of antibody to HSV-1 (95% CI) in serum samples from males and females collected in 1994–5.
Comparison with 1986–7
The prevalence in samples from children aged 10–14 years was significantly lower in 1994–5 than in 1986–7 (p<0.001). Prevalence decreased from 32% (80/250) to 23% (55/243) in males and from 37% (92/250) to 26% (65/252) in females.
Comparison of cohorts born in 1972–6 (that is, 10–14 year olds in 1986–7 with 18–22 year olds in 1994–5) shows an increase in prevalence from 34% (172/500) to 41% (203/498), which was marginally significant (p=0.044). The average annual risk of infection in susceptible individuals in these cohorts was 1.3% (95% CI 0.1% to 2.5%).
HSV-2 ANTIBODY PREVALENCE
Prevalence in 1994–5
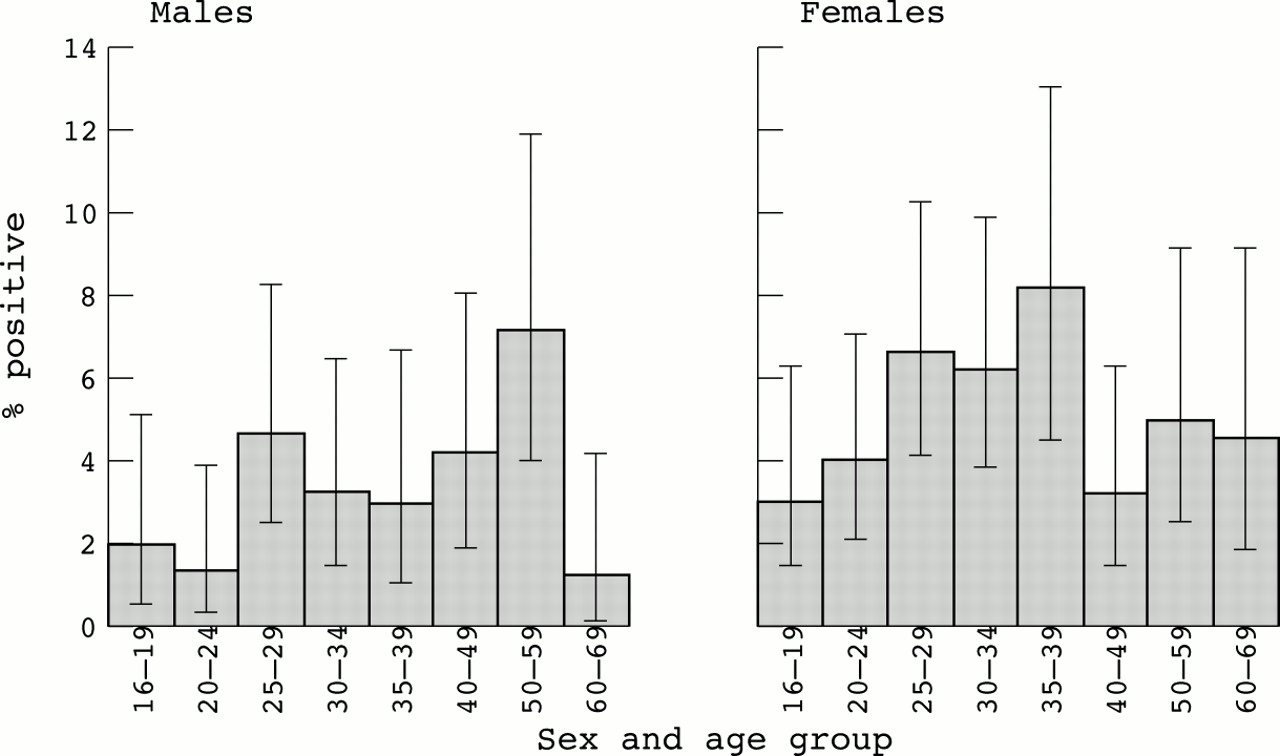
The prevalence of HSV-2 antibody by age and sex in sera collected in 1994–5 is shown in figure 2. In people aged over 16 years a significant difference was seen between sexes, HSV-2 antibody being detected in sera from a total of 3.3% men and 5.1% women (p=0.009). Prevalence of antibody and increasing age was associated in males aged 16–60 years (p=0.006) and in females aged 16–40 years (p=0.011).
{kind=link}
{kind=link}
Age specific prevalence of antibody to HSV-2 (95% CI) in serum samples from males and females collected in 1994–5.
Discussion
This study represents the first investigation of age related prevalence of type specific antibody to HSV-1 and HSV-2 using samples that represent the closest available approximation of the general population of England and Wales.
PREVALENCE OF HSV-1
Our study demonstrates that HSV-1 infection in childhood is becoming less common in England and Wales; the prevalence of antibody to HSV-1 in 10–14 year olds decreased from 34% in 1986–7 to 24% in 1994–5. Over this 8 year period the prevalence in cohorts born in 1972–6 increased from 34% to 41%, suggesting that the average annual risk of infection for susceptible adolescents and young adults is 1.3% (95% CI 0.1% to 2.5%). Above age 15 years the prevalence continues to increase with age, providing further evidence of transmission among adolescents and adults. The relative contributions of oral and genital infections to the antibody prevalence cannot be distinguished, but the pattern of an earlier increase in prevalence in females than males is suggestive of sexual transmission.
Although specific tests for HSV-1 antibody have only recently become available, some comparison with previous studies that measured the prevalence of total HSV antibody is possible. In children, this prevalence can be assumed to be entirely due to HSV-1 infection, since HSV-2 infection is only exceptionally acquired in childhood in the United Kingdom.13, 15 The prevalence of neutralising antibodies to HSV observed in Edinburgh in 1965 was found to be 33% (25/75) in 1–4 year olds and 43% (46/107) in 5–14 year olds.16 This is higher than the prevalence observed in this study, consistent with our observation of a decline in the incidence of infection in childhood. A study of pregnant women from different ethnic groups in west London in 1980–16 estimated the prevalence of HSV-1 antibody by measuring total antibody to HSV in sera negative for specific antibody to HSV-2. Prevalence was associated with age, ethnic group, and social class and was 77% (1955/2554) in women aged less than 30 years, considerably higher than that found in this study. However, this antenatal population of mixed ethnic groups is not typical of the general population of England and Wales and should be compared with caution with the results of this study, which included less than 2% of sera from London.
PREVALENCE OF HSV-2
The two previous studies that used validated type specific antibody assays to measure the prevalence of HSV-2 infection in low risk populations in the United Kingdom were both conducted in London. These found a prevalence in women at least twice the 5.1% detected in this study: 10.4% in an antenatal population in west London6 and 12.4% in blood donors in central London.7 The prevalence of 3.2% in male blood donors7 is similar to the 3.3% prevalence in males observed in our study. When making such comparisons it is important to consider other factors that may contribute to the prevalence seen, in particular the degree to which the samples screened reflect the general population. Both previous studies used selected subgroups of the London population whereas our study did not include any samples collected from adults in London. As is observed for other sexually transmitted infections, the prevalence of HSV-2 infection may be higher in London than in the rest of England and Wales. Further studies are therefore required to determine the burden of HSV-2 infection in the general population of London.
The only other similar study investigating the prevalence of antibody to HSV-2 in the general population of a developed country using a validated type specific assay is described by Fleming et al.17 A random cross sectional sample of the general US population was screened using samples collected between 1976 and 1994 and showed the prevalence of antibody to HSV-2 in the United States to have risen by approximately 30% since the late 1970s, reaching 22% for the period 1988 to 1994. This trend of increasing prevalence is not confined to the United States and has been observed in both developed and developing countries.18, 19 Our study suggests that the rate of infection with HSV-2 is much lower in England and Wales than in the United States.
IMPLICATIONS FOR INCIDENCE OF GENITAL HERPES
Previous oral infection with HSV-1 provides a high level of protection against genital HSV-1 infection.19 Furthermore, although a previous HSV-1 infection offers little protection against acquiring genital HSV-2 infection, it usually prevents the severe clinical manifestations observed with many primary HSV-2 infections.15, 19 A fall in the prevalence of HSV-1 antibodies in adolescents therefore leads to an increase in the pool of adults at risk of disease.
Many local studies in the United Kingdom have shown a high or increasing proportion of cases of genital herpes are due to HSV-1 infection, especially in young women.3, 20–26 One possible explanation for the rise in the incidence of genital infection with HSV-1 seen in the United Kingdom may be a result of changes in sexual behaviour towards an increase in orogenital contact between partners.27, 28 If cases of genital HSV-1 result from orogenital contact, the incidence of genital infection is proportional to the contact rate, the prevalence of oral HSV-1 infection (y), and the proportion susceptible to genital HSV-1 infection (1 − y). For any given contact rate, the highest incidence would occur if the prevalence of oral infection was 50%. At prevalences below 50%, a fall in the prevalence of oral infection would tend to reduce the incidence of genital infection. For example, a fall in the prevalence of oral infection from 34% to 24% (as observed in adolescents in our study) would lead to a 19% reduction in the incidence of genital HSV-1 infection. The increase in orogenital contact would have to outweigh this effect before an increase in genital HSV-1 infections was observed. Alternatively, if genital HSV-1 infections result predominantly from genital contact, a fall in the incidence of infection in childhood would increase the proportion of adults who are susceptible to genital HSV-1 infection and cause incidence of genital infection to rise.
IMPLICATIONS FOR DISEASE CONTROL
The burden of HSV-1 and HSV-2 infection in the general population of England and Wales described in this report has important implications for public health policies. Recently there has been a call to introduce screening using suitable type specific HSV serology assays in an attempt to control the increase in genital herpes infections.29 The health benefits of this are not yet established and the proposal does not satisfy any of the criteria of Wilson and Jungner30 for a successful screening programme. The cost effectiveness of such a screening policy is dependent on the population prevalence, which is considerably lower in England and Wales than in the United States. Vaccines currently in development provide the prospect of more effective disease control.31
Acknowledgments
We thank the staff in the following public health laboratories who collected the sera used in this study: Ashford, Birmingham, Bristol, Cambridge, Cardiff, Carlisle, Exeter, Gloucester, Leeds, Manchester, Norwich, Preston, Reading, Rhyl, and Tooting.
Contributors: The study was designed by NG, PM-C, and DB; AV and MS performed the laboratory tests; confirmatory laboratory tests were carried out by RG and TG; the data were analysed by NG and the PHLS Statistics Unit. The manuscript was prepared by AV, NG, and DB and reviewed by all authors; DB supervised the study.