Article Text

Abstract
Objective: To investigate if the core population hypothesis is applicable to patients with genital chlamydia infections.
Design: Retrospective cross sectional study.
Setting: Two genitourinary medicine (GUM) clinics in the city of Birmingham and eight adjacent clinics.
Subjects: All patients with chlamydia (n = 665) or gonorrhoea (n = 584) attending between 1 October 1995 and 30 September 1996 with a postcode within the Birmingham health district. Controls were 727 patients seen in the same period with no infection.
Methods: Postcodes were used to calculate population prevalence rates per 100 000 aged 15–65 in the 39 wards of the city and to estimate the socioeconomic status using the Super Profile (SP). Ethnic specific rates were also calculated. Data were obtained on gonorrhoea and chlamydia isolation from all the major laboratories of the city over the same time period.
Results: GUM clinic attenders accounted for 67.6% and 82.5% of all chlamydia and gonorrhoea isolates reported by the laboratories and that were available for our epidemiological analysis. Both infections were more common in men and in black ethnic groups. However, patients with gonorrhoea only infection were more likely to be of black ethnicity than those with chlamydia only infection (p = 0.0001) and to have different SP distribution (p = 0.0001). On logistic regression age <20 years, male sex, black ethnicity, and living in neighbourhoods with SP J (“have nots”) were predictive of both infections compared with controls. Overall chlamydia and gonorrhoea prevalence rates were 129 and 98.4 per 105 respectively. Corresponding rates for whites was 64.7 and 37.2 and for black ethnic groups 1105 and 1183 per 105 of each ethnic group. Eight adjacent wards accounted for 41% of the chlamydia and 66.5% of the gonorrhoea.
Conclusion: In a large urban setting patients attending GUM clinics with chlamydia belong to core population groups with similar, but not identical, sociodemographic characteristics to patients with gonorrhoea infection.
- gonorrhoea
- Chlamydia trachomatis
- geomapping
- ethnicity
Statistics from Altmetric.com
Introduction
Sexually transmitted infections (STI) are predominantly urban diseases. Both ethnicity and socioeconomic status appear to be important factors in the acquisition of many sexually transmitted infections. Gonorrhoea rates are higher in African-Americans in the United States1 and African-Caribbeans in the United Kingdom.2, 3 Moreover, in urban settings geographic clustering of diseases have been reported for gonorrhoea1–3 and syphilis,4 and for repeat infections with Chlamydia trachomatis.5
Explanations for the concentration of infection in certain ethnic groups include differences in sexual behaviour6–8 and deprivation. However, differences in incidence are not entirely accounted by behaviour9 or social deprivation.1, 2, 10 Moreover, in some of the reports, because of the availability of alternative healthcare venues the data obtained at testing sites may not represent the socioepidemiology of the infection in the community.
Accurate information on geographic clustering, ethnic concentration, and socioeconomic status of those at risk of infection may help target sexual health education and infection screening programmes.
We report here results of a study of geographical clustering and socioeconomic status of patients with C trachomatis and Neisseria gonorrhoeae genital infection presenting to genitourinary medicine (GUM) clinics in the city of Birmingham over a 12 month period. By collecting data from all the clinics surrounding the city we ensured that the majority of cases presenting to GUM clinics were included.
Subjects and methods
All patients with C trachomatis and N gonorrhoeae infection attending two GUM departments in Birmingham (Whittall Street clinic and Birmingham Heartlands) and eight clinics in the vicinity of Birmingham (Coventry, Burton upon Trent, Dudley, Nuneaton, Redditch, Sandwell, Tamworth, and Wolverhampton) with a postcode within the Birmingham Health Authority (BHA) were included in a retrospective cross sectional study. The study period was between 1 October 1995 and 30 September 1996. C trachomatis was tested from a cervical swab in women and a urethral swab in men. From April 1996 Birmingham Heartlands switched to ligase chain reaction (LCR) for chlamydia isolation in male urine (40 samples). In all other clinics tests were by ELISA with a confirmatory test. Gonorrhoea was diagnosed by culture. Controls were patients presenting for the first time at the two clinics for infection testing in whom no STI was found randomly selected by taking every third (Heartlands) or fourth (Whittall Street) patient.
The information retrieved from case notes for each patient were: age, sex, date of birth, ethnic group, and full postcode. This information was volunteered by the patients in the two Birmingham clinics. All black groups (black Caribbean, black African, and black others) were combined for multivariate analysis as 84%, 88%, and 92% of black controls, chlamydia and gonorrhoea patients respectively belonged to the black Caribbean groups. Indian, Pakistani, and Bangladeshi were combined under Asian. All other ethnic groups were grouped together under “other”. They comprised 5.3%, 4%, and 3.9% of the control chlamydia and gonorrhoea groups respectively.
Patients presenting more than once during the study period with either gonorrhoea or chlamydia to the same clinic were entered only once. We could not identify patients who had attended another clinic with a second chlamydial or gonococcal infection. However, only four (0.3%) patients attended two clinics with identical postcode and only one of these had an identical date of birth. Patients with dual infection with gonorrhoea and chlamydia, whether concurrently or on two separate occasions, were included on both the chlamydia and gonorrhoea database only once. Information was obtained from all the main microbiology laboratories in Birmingham on the number of chlamydia and gonorrhoea isolates during the study period. It was not possible to determine the source of the samples except for those who attended GUM clinics. One laboratory used LCR throughout and another changed to LCR in April 1996 for the isolation of chlamydia. In another laboratory culture was used throughout.
Geomapping was performed with the arcview mapping program using the postcode. Patients were assigned to one of 39 wards in Birmingham. Infection rates were reported as rates per 100 000 residents aged 15–64 obtained from the 1991 census.
Super Profile (SP) classification was used as an indicator of socioeconomic status. Super Profile is a geodemographic system which categorises households according to the characteristics of the neighbourhood in which they are located, using the postcode to assign SP categories. It is based on the 1991 census data and enhanced by other data including the electoral roll and credit information. Households have been divided into 10 groups (from A to J) based on 120 separate characteristics, with A being the most affluent group and J the most deprived group.11 SP correlates well with other commonly used deprivation indices such as Jarman, Townsend, and Carstairs indices.11 The socioeconomic correlation is limited by the fact that SP has been derived from information from households while infection and clinic attendance data are from individuals.
STATISTICS
Prevalence rates for chlamydia, gonorrhoea, and controls for individual wards were correlated using the Pearson correlation. Demographic characteristics from chlamydia and gonorrhoea patients were compared with controls by univariate analysis. Ethnicity (white, black, Asian, and other), age (<20, 20–29, 30–39, >40), sex (male, female), and SP were entered as covariates into a multivariate forward stepwise logistic regression model using the spss 9 software package. Demographic characteristics of patients with gonorrhoea and chlamydia, excluding those with dual infection, were also compared by univariate analysis using the Pearson χ2 test and odds ratio.
Results
During the study period 1121 diagnoses of chlamydia (152 by LCR, 228 by culture, and the remainder by ELISA), and 789 cases of gonorrhoea were made by the main laboratories in Birmingham. Microbiological laboratories serving large gynaecology units accounted for 353 isolates of chlamydia and 69 isolates of gonorrhoea. No patients with a Birmingham postcode attended Coventry, Burton upon Trent, Nuneaton, Tamworth, and Wolverhampton clinics with either infection. The remaining five clinics reported 758 episodes of C trachomatis infections in 665 residents living within the geographic boundaries of Birmingham Health Authority (BHA); 97.2% were seen in the two Birmingham clinics.
The same five clinics reported 651 cases of N gonorrhoeae infections from 584 individuals living within the BHA. 97% of the patients were diagnosed at the two Birmingham clinics. Thirteen (1.8%) chlamydia and 24 (4%) gonorrhoea patients were self reported as being homosexual men. Table 1 shows demographic characteristics of the patients and controls. Both infections were more commonly isolated in men and in black ethnic groups. Control patients were more likely to be of Asian ethnicity than either chlamydia (p <0.001) or gonorrhoea (p <0.0001) patients.
Demographic data of patients with chlamydia and gonorrhoea resident within Birmingham Health Authority and attending GUM clinics in and around Birmingham. Controls were patients attending for infection testing at GUM clinics during the same period without an STI
When directly comparing patients who had only C trachomatis and only N gonorrhoeae infections there was a similar sex and age distribution but the proportion of black ethnic groups was lower in chlamydia patients (41.6% v 65.7%, χ2 68, p = 0.0001). There was also a significant difference in the Super Profiles between the two infections (χ2 43, p = 0.0001).
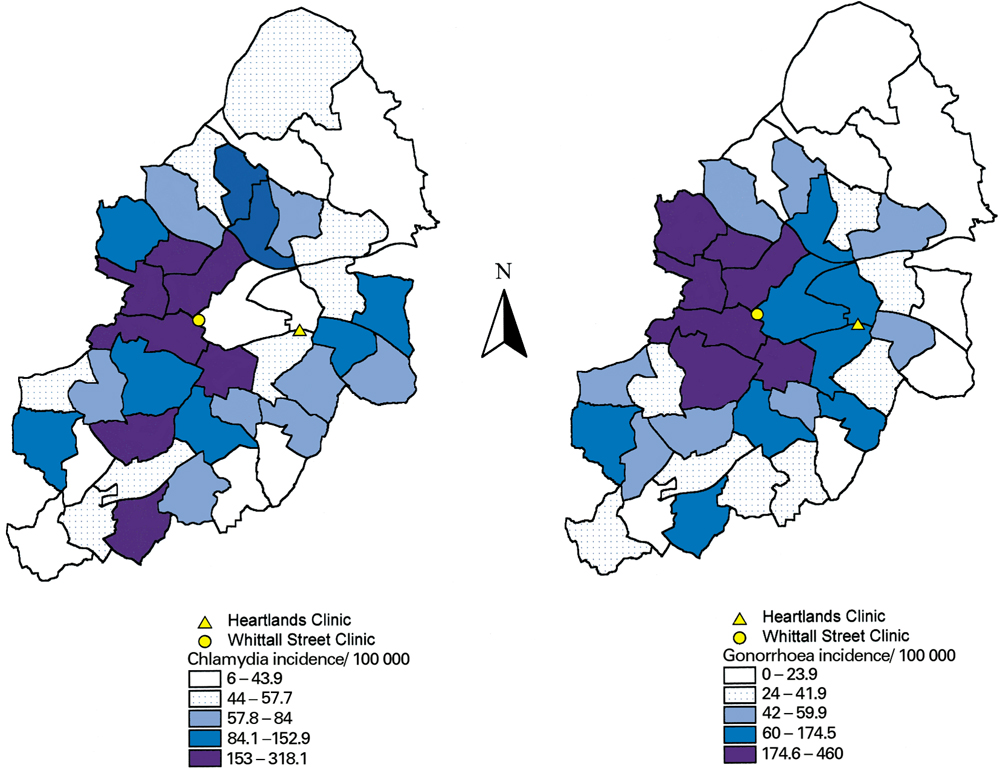
Overall chlamydia and gonorrhoea prevalence rates in the BHA area were 129/105 in the population aged 15–64 and 98.4/105 in the population aged 15–64, respectively. Respective rates for whites were 64.7/105 for chlamydia and 37.2/105 for gonorrhoea and for black ethnic groups were 1105/105 for chlamydia and 1183/105 for gonorrhoea. Eight adjacent wards accounted for 41% of cases presenting with chlamydia and 66.5% of cases attending with gonorrhoea (and 35.5% of controls) with a prevalence rate of 153–318/105 and 181–460/105 respectively (fig 1). Five of these wards were common to both conditions. The top eight wards from which control patients came accounted for 38% of the patients, five of which overlapped with the top chlamydia and six with the top gonorrhoea wards. Chlamydia and gonorrhoea rates per ward were significantly correlated for the 39 wards (r = 0.83 p<0.0001) for all ethnic groups and for whites (r = 0.41 p = 0.009) but not for black ethnic groups (r 0.29 p = 0.07). If attendance for infection testing at a GUM clinic can be taken as an index of sexual risk taking and heath seeking behaviour, there was a significant correlation between population prevalence rates in each ward for both infections and the population rates in the controls (no infection found) attending from the same wards (r = 0.66 for chlamydia and 0.72 for gonorrhoea, p <0.0001).

{kind=link}
Prevalence of infection by Chlamydia trachomatis (left) and Neisseria gonorrhoeae (right) presenting to sexually transmitted disease clinics from the 39 wards of Birmingham Health Authority. Wards have been categorised in quintiles according to prevalence of each infection per 105 people aged 15–64. (Prepared by the West Midlands Cancer Intelligence Unit, GIS Service, 1999.)
Super Profile distribution for the United Kingdom, Birmingham, and the three patient groups are shown in table 2; 57.5% of all chlamydia, 71.2% of all gonorrhoea, and 56.3% of controls lived in areas designated as SP E and J.
Superprofile distribution (% of households) in the United Kingdom and Birmingham Health Authority (Bh'am) and for STI clinic attenders (% of individuals attending)
Stepwise logistic regression showed that age <20, male sex, black ethnicity, and living in neighbourhoods designated as SP J were positively associated with both infections compared with the controls (table 3). There was no clear pattern in the distribution of cases of chlamydia and gonorrhoea infection across the 10 SPs. Individuals with chlamydia were more likely than controls to live in neighbourhoods designated as SP areas H and J and those with gonorrhoea in SP area J.
Stepwise forward logistic regression using ethnic groups, sex, age groups, and socioeconomic status based on the Super Profile of the place of residence. Controls were patients who attended the STD clinic with no infection. Gonorrhoea and chlamydia infected patients were compared with controls. Odds ratio with 95% confidence intervals
Discussion
We have compared the demographic features, the geographic clustering, and socioeconomic profile of patients attending GUM clinics infected with C trachomatis and N gonorrhoeae in a large urban setting and have shown a striking convergence between the two infections in this setting. Our conclusions must, however, be treated with caution. During the period of study 32.4% of the chlamydia and 17.5% of gonorrhoea diagnosed by the main microbiology laboratories in Birmingham were not seen in GUM clinics. The majority of the non-GUM diagnoses were reported from microbiological laboratories serving large gynaecology units. It is not possible to determine how many of these lived within the BHA boundaries, nor how many were referred to GUM clinics and therefore duplicated. Moreover, the use of ELISA tests for chlamydia will underestimate the prevalence of this infection12 and it is possible that more sensitive assays may reveal different patient characteristics. Finally as controls we used patients attending for the first time GUM clinics for infection testing in whom no infection was found as controls. We argued that this group may be representative of both sexual risk taking as well as sexual health seeking behaviour. Though, a non-GUM control population would avoid some of the biases introduced by the present controls, the use of such controls introduce other operational, ethical, and methodological problems.
Our study showed that in a large urban centre infection with chlamydia occurs in geographic core areas analogous to that reported for gonorrhoea,1–3, 13–15 with considerable overlap between the two infections. Both conditions are commonest in black men under 20 years of age. Moreover, nearly two thirds of both infections occurred in areas designated as SP groups E and J. However, the sociodemographic profiles of the two infections were not identical. Patients with chlamydia presenting to GUM clinics are more likely to be white or Asian and have broader socioeconomic spread as judged by the Super Profile of their local neighbourhood compared with those presenting with gonorrhoea.
Our results confirm studies from the United States and the United Kingdom that in urban settings both gonorrhoea1–3, 16, 17 and chlamydia18–20 are commoner in black ethnic groups even when corrected for socioeconomic factors.2, 3, 10 Not all studies, however, have shown such a concentration21–25 or a relation with deprivation indices.20, 21 The reasons for the ethnic differences in infection rates is unknown. The national survey of sexual lifestyles showed that black men (but not women) were significantly more likely than white or Asian men to report sex before age 16.8 In people attending a GUM clinic black men were more likely to be younger, unemployed, had earlier coitarche, had sex with an African woman, and be infected with gonorrhoea or chlamydia than white men.6 Black women were younger, had earlier coitarche, more pregnancies, and births, were more likely to be infected with gonorrhoea, chlamydia, and trichomoniasis, and less likely to use condoms than their white counterparts.7 Black women did, however, report fewer non-regular sexual partners in preceding year than white women. African-Caribbean patients attending one of the participating clinics (Whittall Street) were more likely to present with an STI than whites, to have multiple infections, to have more than two partners (73% v 61%), and more non-regular sex. Condom use was similar between ethnic groups (Pareek M, Arichi T, Satgunum S, personal communication).
Social and, consequently, sexual relationships to a large extent occur among people with similar age, ethnicity, religious, and educational background26 facilitated by residential segregation (clustering) of ethnic groups. Greater assortative mixing has been demonstrated in the United States in core geographic locations27 particularly among African-Americans.26 Moreover, spatial distance between partners in core gonorrhoea areas is shorter than those in non-core zones.13 Barlow et al showed a similar high level of assortative mixing in heterosexual patients attending a large London GUM clinic when the country of birth of the parents of the index patients is taken into account.28
The geoclustering of chlamydia in our study, though somewhat less than that observed for gonorrhoea was remarkable. Moreover, there was a similar age, ethnicity, and Super Profile distribution between patients presenting with gonorrhoea to GUM clinics in Birmingham and Leeds.2 In both cities Super Profile groups (E and J) accounted for the majority of cases of gonorrhoea and, in Birmingham, of infection with chlamydia (table 2). Wasserheit and Aral4 have postulated that sociogeographic concentrations of STIs are to some extent a function of the stage of the epidemic for any particular infection. The concurrence of the core geographic areas for the two diseases, and the high prevalence of infection in these core areas, would suggest that, at least for the population accessing GUM clinics in Birmingham, the epidemics for gonorrhoea and chlamydia are at similar stage of evolution. However, a similar study carried out in the city of Coventry, 22 miles west of Birmingham, did not show a similar degree of confluence between the infections (Winter et al29 and Winter AJ, personal communications).
Overlapping of the areas with high infection rates of both infections could facilitate locally targeted sex education which has been suggested to be more useful.4, 30 If attendance for infection testing at a GUM clinic can be taken as a sign of both sexual risk taking as well as sexual health seeking behaviour, the overlap of geographic location and SP of patients found to have gonorrhoea or chlamydia with that of the control patients who had attended GUM clinics with negative tests, with may also be useful for targeted sex education. The present study suggests that in some large urban centres young African-Caribbeans living in neighbourhoods with similar sociodemographic characteristics are at greatest risk of infection with gonorrhoea or chlamydia. Young people with excess income which they spend on leisure (SP E), and those at the lowest end of the socioeconomic scale (SP J) might be considered for targeted sex education.
Acknowledgments
We wish to thank Carol Cummings for her help in cleaning up the database and for statistical advice.
Contributors: MS designed the study, collated data, and wrote manuscript; SG, RR, and MA designed the database, entered data, liaised with clinics and laboratories, commented on manuscript; RS performed geomapping and commented on manuscript; JD and JR performed statistics and commented on manuscript.