Article Text

Abstract
Background: Neonatal herpes is a condition with high morbidity and mortality. The greatest risk occurs when the mother acquires herpes simplex virus (HSV) towards the end of pregnancy. A study from Seattle has suggested that the risk of acquisition of HSV during pregnancy was 3.7%. In Australia, HSV-2 infection is less common in pregnant women than in the United States. Consequently we conducted a study to establish HSV seroprevalence and the rate of HSV seroconversion in this population.
Methods: The study was conducted at Westmead Hospital, Sydney, between June 1995 and April 1998. Women completed a questionnaire covering risk factors for the acquisition of genital herpes. A serum sample during pregnancy and a specimen of cord blood were obtained and tested for antibodies to HSV-2 using a type specific indirect enzyme linked immunosorbent assay (ELISA). Equivocal results were resolved by western blot. A subset of the paired sera was tested for antibodies to HSV-1. The data were analysed using spss.
Results: 326 of the 2616 (12.5%) women were HSV-2 seropositive. Three women (0.15%) acquired HSV-2 infection during pregnancy. None of the three babies of these mothers developed neonatal herpes. 416 maternal cord pairs were tested for HSV-1 antibodies and 330 (79.3%) were positive. No HSV-1 seroconversions occurred.
Conclusions: In this population, HSV acquisition was uncommon (0.34% per year) and neonatal herpes was rare. A cost effective analysis suggested that type specific serology to screen pregnant women and their partners in low prevalence communities was not cost effective.
- type specific serology
- herpes simplex virus
- neonatal herpes
Statistics from Altmetric.com
Introduction
Neonatal herpes is a devastating condition. Even with treatment the majority of infants will die or be left with severe neurological sequelae.1 Fortunately the condition is uncommon with an estimated incidence of up to 50/100 000 live births in some parts of the United States,2 6/100 000 in Sweden,3 8/100 000 in Australia,4 and 3/100 000 in the United Kingdom.5
The greatest risk to the neonate of contracting herpes occurs when the mother acquires genital herpes during pregnancy, particularly if this occurs towards or at the end of the third trimester.6 A recent study from Seattle suggested that the maternal risk of herpes simplex virus (HSV) type 1 or 2 acquisition during pregnancy was 3.7% for women who were HSV seronegative and 1.7% for HSV-2 in those who were initially HSV-1 seropositive.7 The results of this study and the observation that the prevalence of HSV-2 infection has increased by 30% in American adults over the past two decades8 have prompted some authors to recommend the use of serological testing in couples considering pregnancy to detect those at risk. This would enable women who are HSV-2 seronegative with an HSV-2 seropositive partner to use condoms or abstain from intercourse during pregnancy.7 The feasibility of this approach and its cost effectiveness has not been tested and the impact of this approach on the incidence of neonatal herpes is likely to be minimal.9
The prevalence of HSV-2 infections varies enormously in different geographic locations, and in different populations.10 The risk of HSV acquisition during pregnancy may be dependent on several factors including HSV-2 and possibly HSV-1 prevalence in the community, the proportion of women considering pregnancy or who become pregnant who are HSV-2 negative, and sexual behaviour during pregnancy. Limited information from pregnant women in Australia11 has suggested that HSV-2 infection is less common than in some parts of the United States6, 12–15 and this may explain the differences in the incidence of neonatal herpes.
Consequently, we conducted a study to establish HSV-1 and HSV-2 seroprevalence, the factors associated with HSV acquisition and the HSV seroconversion rate in a large hospital in Sydney, Australia, where HSV-2 seroprevalence was lower than Seattle.
Subjects and methods
STUDY SETTING
The study was conducted in the obstetric department at Westmead Hospital. This is a large teaching hospital situated in the western suburbs of Sydney, which services a multicultural population. The women were recruited from antenatal clinics between June 1995 and April 1998. Antenatal clinics were run every weekday. However, owing to limited staff availability, recruitment occurred on 2 and sometimes 3 days per week. Whenever possible, we tried to recruit during the busiest clinics.
STUDY PROCEDURES
A research assistant approached women in the waiting room. The nature of the study was explained, written informed consent obtained, and the women were asked to complete a questionnaire covering risk factors for the acquisition of genital herpes (including age, age at coitarche, lifetime number of sexual partners, and history of genital herpes). The questionnaire was available in several languages (English, Arabic, Chinese, and Vietnamese) to cater for the diverse ethnic population attending Westmead Hospital. In some cases non-English speaking patients completed the questionnaire with the assistance of a professional interpreter allocated by the hospital. In other cases non-English patients were assisted by an accompanying friend or relative.
Serum samples were obtained from the serology laboratory from excess serum previously or concurrently taken for syphilis and rubella serology usually during the first trimester. To determine HSV seroconversion during pregnancy a specimen of cord blood was obtained from routine samples taken at the time of delivery. Paired samples were used to test for HSV antibodies and to establish HSV seroconversion.
HSV TESTING
Sera (maternal and cord blood) were stored at −20°C and tested for antibodies to HSV-2 using an indirect enzyme linked immunosorbent assay (ELISA) specific to glycoprotein G2 (gG2).16 The assay has levels of sensitivity and specificity of greater than 98%.16 Equivocal ELISA results were resolved by western blot.17 Seroconversion during pregnancy was defined as an HSV-2 negative maternal serum sample and an HSV-2 positive cord blood sample. All seroconversions were confirmed by western blot testing.
A subset of the paired sera (maternal and cord) were selected and tested for antibodies to HSV-1. We selected every fifth cord specimen with an available matching maternal specimen. Depending on the HSV-2 serostatus of these sera they were tested by the Behring ELISA for the detection of total antibody to HSV (if HSV-2 negative) or by western blot (if HSV-2 positive).17 This strategy was used because of the current lack of a low cost, low labour intensive, accurate ELISA for antibody to HSV-1.
DATA ENTRY AND ANALYSIS
The data from the questionnaires, and the serological results were entered onto a database and analysed using spss.18 Statistical analysis used included descriptive and comparative tests including Pearson's χ2 and Student's t test.
Results
During the period of the study 13 372 women delivered babies at the hospital; 7560 women attended on days when recruiting occurred, of which 3706 (49%) agreed to participate. Serum was available for HSV testing on 2616/3706 (70.6%) women who completed the questionnaire; 2040 cord blood samples were available from the group of 2616 participants. It was these 2040 mother cord pairs that were included in the seroconversion analysis. There were several reasons for lack of availability of maternal serum including no specimen taken, specimen processed at another laboratory, and insufficient serum remaining after routine syphilis serology and loss or mislabelling of specimen. Some of the women who were being managed privately had serum processed at other laboratories. All of the local laboratories were approached on several occasions to obtain serum samples. However, this approach only yielded a handful of specimens over an 18 month period. Consequently this approach was dropped and only women attending Westmead Hospital for their antenatal care and serology were included. Reasons for lack of cord blood included specimen not taken, insufficient serum, loss of specimen, and the woman delivering at another hospital.
In order to determine how representative our sample was, we compared the demographic, sexual, and obstetric characteristics of all the women who attended antenatal clinics on the days when recruitment occurred but did not participate (3861) with those who were recruited (3706). Participants were significantly younger than the unrecruited women (28.0 (SD 5.3) years and 31.2 (5.4) years respectively, p<0.001). There was a significant difference in country of birth for recruited and unrecruited women (p=<0.001). Sixty five per cent of the recruited women were born in Australia compared with only 48% of the unrecruited group and fewer recruited women were born in North or South East Asia (10.5% compared with 24.4%) and the Middle East (6.1% compared with 9.7%). The mean gravidity of recruited women was 2.0 (SD 1.5) compared with 3.0 (1.6) for unrecruited women. However, most of this difference occurred as a consequence of a small number of high gravidity women in the unrecruited group. Similar differences were seen with regard to parity. The mean parity for both groups was 1.0, but a small number of highly parous women in the unrecruited group resulted in a significant difference between them (p<0.001). The final difference related to whether participants were public or private patients. Eighty four per cent of recruited women were seen in the public sector compared with 67% of the unrecruited women (p<0.001).
A total of 326 (12.5%) women were HSV-2 seropositive at the time of their enrolment to the study. On univariate analysis HSV-2 seropositivity was correlated with age, country of birth, age of first sexual intercourse, lifetime number of sexual partners, previous sexually transmitted diseases, having a partner with herpes, educational status, parity, and gravidity.
Although age, ethnic, and other factors were significantly different between recruited and unrecruited patients the actual differences in HSV-2 seropositivity associated with the factors were small with the exception of public versus private status. For example, 11.5% of women from Australia and New Zealand were HSV-2 positive compared with 12.2% of those from North and South East Asia and 9.2% of those from the Middle East. However, 12% of public patients were HSV-2 positive compared with 6.3% of the private patients. An anonymous unlinked study of HSV-2 seroprevalence in 300 consecutive antenatal admissions during the study showed 12.6% were HSV-2 positive, similar to that of the recruited women.
Three of the 1746 (0.17%) HSV-2 susceptible women (that is, those who were initially HSV-2 negative) had an HSV-2 seroconversion during the pregnancy (fig 1). The average duration between antenatal and cord blood was 182.8 days giving a risk of HSV-2 acquisition of 1.72 (95% CI 0.35–5.02) per 1000 women or 3.43 (95% CI 0.71–10.0) per 1000 woman years.

Example of western blot results for one maternal/cord pair. Arrows indicate the presence of bands at 140 kD and 92 kD specific to HSV-2.16 (a) gG2 specific monoclonal antibody, (b) serum from patient with clinically proved HSV-2 infection. Samples (c) and (d) show a mother/cord pair. (c) Maternal serum sample negative for HSV-2 (no type specific bands). (d) Cord serum sample from baby born to mother c. The appearance of type specific bands in (d) demonstrates a seroconversion to HSV-2.
The first baby born to a woman who had an HSV-2 seroconversion during pregnancy was a healthy female baby born vaginally at 41.5 weeks and discharged from hospital 5 days later. The 30 year old gravida 4 para 2 mother had chronic active hepatitis due to hepatitis C. The second baby was born to a 23 year old G2 P0 mother. Again a healthy baby girl was delivered vaginally at 42.2 weeks and discharged 4 days later. The final baby was born to a 24 year old G2P1 mother. The vaginal delivery at 41.2 weeks was uncomplicated and the healthy baby boy was discharged 3 days later.
In all, 408 maternal cord pairs were tested for HSV-1 antibodies and 323 women (79.2 %) were seropositive. Although only a small number of maternal cord pairs were tested no seroconversions were detected.
Discussion
Previous studies have suggested that HSV infection in pregnancy is an important public health problem.2, 3, 6, 7, 19, 20 However, this study shows that in communities with low HSV-2 seroprevalence, HSV acquisition in pregnancy is uncommon (0.34% per year) and neonatal herpes is extremely rare. Indeed during the period of the study there was only one case of neonatal herpes out of 13 372 deliveries at Westmead hospital (7.5/100 000). This compares with 28.2/100 000 in Seattle19 and 40/100 000 in Atlanta.21 The baby with neonatal herpes was born prematurely to a mother who did not participate in the study. The baby was admitted to neonatal intensive care shortly after delivery with respiratory distress and sepsis. HSV-1 was isolated from the urine on day 19.
There were a number of statistically significant differences between women who agreed to participate in the study and those who were not recruited including age, gravidity, country of birth, and whether they were private or public. It is difficult to know whether any of these differences were important. However, as mentioned above the differences in parity and gravidity were as a consequence of a small number of women with multiple previous pregnancies. Age has been shown to be an important factor for the acquisition of HSV-2, with older individuals having a higher HSV-2 prevalence.22 However, the actual differences between the groups were small. Indeed, if anything, the differences in country of birth and public or private status probably contributed to a slight overestimation in HSV-2 seroprevalence in this population. Furthermore, an unlinked anonymous study of 300 women who attended consecutively during the period of the study showed a seroprevalence of 12.6% and this was not significantly different from the main study. We have shown that although the women who participated in the present study were not a completely representative sample of women attending the antenatal clinic at Westmead Hospital, they originated from a variety of ethnic and social backgrounds and included patients from the public and the private sector. In addition, the biological significance of these differences probably is negligible.
There are numerous studies of HSV-2 seroprevalence in pregnancy and these are summarised in table 1. Many of these studies have been small and conducted in selected groups of women. HSV-2 infections have increased in some communities20, 23 but appear relatively static in western Sydney. A study in 1986 with 229 consecutive specimens from antenatal patients using identical laboratory methods showed a prevalence of 14.5%,11 while the current study showed a prevalence of 12.5%.
HSV type 2 seroprevalence in antenatal clinic attendees
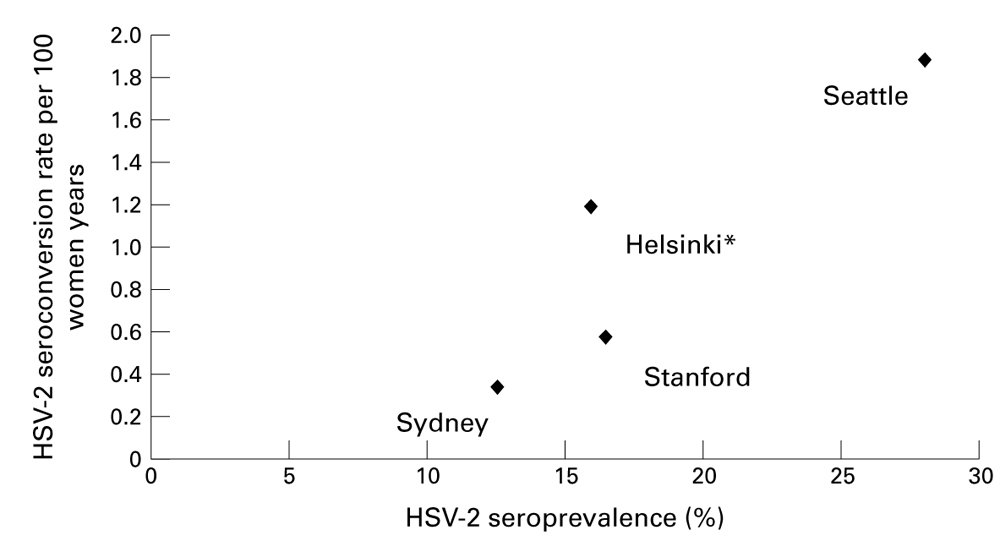
In Seattle the annualised HSV-2 seroconversion rate was 1.89%,7 in Helsinki it was 1.19%,24 in Stanford 0.58%13 and in our study it was 0.34%. The relation between HSV-2 seroprevalence and the rate of HSV-2 seroconversion in these four studies suggests a positive association (see fig 2; r = 0.912, p = 0.09). Future studies will determine whether this association is maintained and whether it holds over a range of seroprevalence.

{kind=link}
{kind=link}
Relation between HSV-2 seroprevalence and seroconversion during pregnancy in Sydney, Stanford, Seattle, and Helsinki. *The annualised HSV-2 seroconversion rate calculated from five of 840 women who seroconverted over an average of 6 months' follow up.
One of the important questions raised by this study is why HSV acquisition during pregnancy differs in different communities. There are several possible explanations. Firstly, as discussed above the prevalence of HSV-2 infection in the community may be important. Where HSV-2 infections are more common the likelihood of exposure to the infection is greater. Secondly, sexual behaviour of women and their partners during pregnancy may be an important factor. Women who have multiple partners or whose male partners have sexual intercourse with other women may be at particular risk. Some couples may change their sexual behaviour during pregnancy, perhaps favouring orogenital sex. This may place HSV-1 seronegative women at risk of HSV-1 acquisition. Little is known about sexual behaviour during pregnancy and more detailed information may help determine risk behaviour and establish reasonable control strategies. Finally, HSV-1 seroprevalence may be important. Women who are HSV-1 negative may be susceptible both to HSV-1 and HSV-2 during pregnancy. It is of interest that HSV-1 seroprevalence in this community was 79% in this study and 80% in 198611 compared with 65% in Seattle.
What control strategies are available and applicable to prevent neonatal herpes? A strategy that has been suggested is use of HSV type specific serology to screen couples considering pregnancy or at the time of the first antenatal visit.7, 19 Women with antibodies to HSV-1 and 2 could be reassured about the minimal risk to the baby and advised to tell their obstetrician or midwife about the infection. Where partners are seroconcordant (the same HSV serostatus) the couple could be reassured that the risk to the baby is minimal. However, serodiscordant couples could be counselled about the risk of HSV acquisition and advised to use condoms and avoid cunnilingus (if the man is HSV-1 positive and his partner is not). In addition, the man could consider using antiviral suppression therapy, which has been shown to decrease the frequency of recurrences25–27 and viral shedding,28 and may reduce the likelihood of transmission. This approach may be welcomed by some couples29 but is unlikely to have much public health impact9 and in HSV-2 low prevalence populations the costs will probably outweigh the benefits.
In 1993 Randolph and co-workers34 developed a model to determine the efficacy, risks, and costs associated with caesarean section for the management of genital herpes in pregnancy. Using the assumptions in this model, we have calculated the cost of serological screening to prevent neonatal herpes in two antenatal settings. The first was a high HSV-2 seroprevalence (28%) and high HSV-2 seroconversion in pregnancy setting (1.89% per annum) the second a lower HSV-2 seroprevalence (12%) and lower seroconversion (0.34%) population (table 2). Presuming the cost of HSV-2 screening to be $10, in the low seroprevalence population, the cost of screening per case of neonatal herpes prevented was $1 240 000 and in the high seroprevalence community it was $254 000.
Estimated costs of serological screening for HSV-2 in pregnant women and their partners as strategy for preventing neonatal herpes
Given the association between HSV-2 seroprevalence and the rate of HSV-2 seroconversion in pregnancy, an alternative and cheaper approach would be to conduct regular HSV seroprevalence surveys in women attending antenatal clinics. If seroprevalence to HSV-2 remains low then it is likely that HSV acquisition during pregnancy will not be a major problem. However, if HSV-2 seroprevalence is high or increasing (particularly where HSV-1 serprevalence is relatively low) consideration of the public health measures discussed above may be warranted.
Acknowledgments
This study was funded by grants from the Ramaciotti Foundation and the Australian National Health and Medical Research Council (954001).
We would like to thank Dr Catherine O'Connor for her assistance at the beginning of the study, Jane Griffith, the nursing and midwifery staff in the antenatal clinics, Jocelyn Ling and Stuart Gilmore for their help in recruiting patients, Mr Con Tsiavos from the Information Services Division at Westmead Hospital for assistance in data retrieval, and Stig Jeanson for the gG2 antigen.
Contributors: AM, study idea, protocol design, data analysis and interpretation, report writing; JT, specimen collection and storage, serum assays, report writing, and manuscript review; RT, study coordination, data analysis and interpretation, and report writing; CS, recruitment, specimen collection and storage, serum assays, and data entry; GB, statistical advice and assistance with study design, data analysis and interpretation. Manuscript review; KW, recruitment, data entry; JP, recruitment, data entry; CM, database management and statistical analysis; BT, protocol design, manuscript review; AC, study idea, protocol design, supervision of laboratory tests, interpretation of data, and report writing.