Article Text

Abstract
Background: The association between herpes simplex virus type 2 (HSV-2) and human immunodeficiency virus (HIV) and the development of HSV vaccines have increased interest in the study of HSV epidemiology.
Objectives: To estimate the age and sex specific seroprevalence of HSV-1 and HSV-2 infections in selected populations in Brazil, Estonia, India, Morocco, and Sri Lanka.
Methods: Serum samples were collected from various populations including children, antenatal clinic attenders, blood donors, hospital inpatients, and HIV sentinel surveillance groups. STD clinic attenders were enrolled in Sri Lanka, male military personnel in Morocco. Sera were tested using a common algorithm by type specific HSV-1 and HSV-2 antibody assay.
Results: 13 986 samples were tested, 45.0% from adult females, 32.7% from adult males, and 22.3% from children. The prevalence of HSV-1 varied by site ranging from 78.5%–93.6% in adult males and from 75.5%–97.8% in adult females. In all countries HSV-1 seroprevalence increased significantly with age (p<0.001) in both men and women. The prevalence of HSV-2 infection varied between sites. Brazil had the highest age specific rates of infection for both men and women, followed by Sri Lanka for men and Estonia for women, the lowest rates being found in Estonia for men and India for women. In all countries, HSV-2 seroprevalence increased significantly with age (p<0.01) and adult females had higher rates of infection than adult males by age of infection.
Conclusions: HSV-1 and HSV-2 seroprevalence was consistently higher in women than men, particularly for HSV-2. Population based data on HSV-1 and HSV-2 will be useful for designing potential HSV-2 vaccination strategies and for focusing prevention efforts for HSV-1 and HSV-2 infection.
- seroepidemiological study
- herpes simplex virus
- age
- sex
- Brazil
- Estonia
- India
- Morocco
- Sri Lanka
Statistics from Altmetric.com
Infections with herpes simplex virus types 1 and 2 (HSV-1 and HSV-2) are among the commonest human viral infections. HSV-1 is the usual cause of oro-labial herpes and HSV-2 of genital herpes. Globally, HSV-1 is most commonly transmitted horizontally in childhood, although improvements in socioeconomic conditions in some western countries have resulted in declining rates of childhood infection.1 HSV-1 is increasingly recognised as a cause of first episode genital herpes in these countries.2,3
HSV-2 is one of the commonest causes of genital ulceration worldwide. HSV-2 is almost always sexually transmitted and as such has been shown to be a good marker of sexual behaviour in populations.1,4,5 Up to 70% of genital HSV infections are unrecognised,6 so seroepidemiological studies are critical to understanding the pattern and distribution of infection within populations. Even though the majority of HSV infections are unrecognised, most people who are infected shed virus at some time and are therefore potentially infectious.
There is increasing evidence that HSV-2 facilitates HIV transmission,7,8 making the development of HSV control methods a priority.6,9 Recent efforts to develop an HSV-2 vaccine have met with limited success,10,11 but these trials have underscored the importance of collecting population based HSV type specific data. In particular, two phase III trials of a prospective subunit vaccine for HSV-2 were found to prevent disease in women who were HSV-1 naive.10 If these results are confirmed, age specific data on HSV-1 seroprevalence will be critical to defining country specific vaccine strategies.
Recently, serological tests that can accurately distinguish between antibodies to HSV-1 and HSV-2 have become commercially available allowing more widespread study of the epidemiology of these infections. In this paper we present the results of a study designed to estimate the age and sex specific seroprevalence of HSV-1 and HSV-2 infections in selected populations in Brazil, Estonia, India, Morocco, and Sri Lanka, countries in which there is currently little information about the epidemiology of HSV and with low HIV rates in the general population.12
METHODS
Study populations
Sites were selected on the basis that there were few existing data on HSV seroepidemiology and they had the appropriate infrastructure to conduct this research. Each centre collected samples from antenatal clinic attenders and from either children attending hospital (Estonia, India, Morocco, Sri Lanka) or children involved in vaccine studies (Brazil). Additional samples were collected from other adult populations chosen for their low risk profile for HIV/STD in each country, including blood donors in Brazil, Estonia, India, and Sri Lanka; adult hospital inpatients in Sri Lanka; and selected surveillance groups for HIV monitoring in Morocco. Some centres enrolled populations supposed to be at high risk for HIV/STD, such as STD clinic attenders in Sri Lanka, and male military personnel in Morocco. Seventy per cent of specimens were prospectively collected during 2000, the remainder being stored samples collected before this (table 1⇓).
Number of serum samples tested for antibodies to HSV-1 and HSV-2
Samples were anonymised. Age and sex were the only data available on each sample.
Laboratory methods
A “minimum” testing algorithm was developed to avoid unnecessary testing of samples; the level of childhood infection with HSV-1 infection was determined in sera from 1–11 year olds. If the HSV-1 antibody prevalence was greater than 80% in these children, only a random sample of 20% of the adult (that is, age >11 years) sera were tested from that country. All sera from adults aged 12 years and older were tested for HSV-2 antibody. In practice, however, four of five laboratories tested all sera for antibodies to both HSV-1 and HSV-2, as this was logistically simpler to do.
Validation and standardisation of laboratory methods
All primary testing of sera from the main serum banks and reference panels for HSV-1 and HSV-2 was undertaken using the indirect HSV-1 (gG1) and HSV-2 (gG2) antibody assays (HerpesSelect, Focus Technologies, CA, USA). These assays had previously been shown to be both sensitive and specific,13 and FDA approved. Assay kits obtained from one manufacturing batch were obtained in bulk and distributed to the sites by the Central Public Health Laboratory (CPHL), London, UK.
To validate the testing performed in each participating laboratory, CPHL distributed a panel of sera previously tested with the reference HSV type specific blocking assays.14 The panel consisted of 88 sera which included a range of HSV-1 and HSV-2 negative, equivocal and positive specimens, and was tested blind.
All participating centres tested the reference panel twice, before and after testing the study sera, with the Focus ELISA kits for HSV-1 and HSV-2. Qualitative and quantitative results of reference panel testing were returned to CPHL. All laboratories achieved greater than 90% sensitivity compared to consensus. For the HSV-1 reference panel, all laboratories except Morocco achieved specificity and positive predictive values of greater than 90% compared to the consensus of results. For Morocco, these values were 88% and 90% respectively. For the HSV-2 reference panel, all laboratories achieved specificity and positive predictive values of 97% or greater, compared to the consensus results.
A subset of sera was retested at CPHL, using the in-house type specific binding ELISA assay.14 Retested sera included all equivocal sera (for HSV-1 or HSV-2) and a random sample of double (HSV-1 and HSV-2) negative sera.
Statistical analysis
Data were double entered into Epi-Info at each site and then sent to the department of STD, University College London (UCL) for analysis. Data analysis was undertaken using SPSS version 10.0. For the purposes of analysis, a category of “low risk” group was devised. This comprised hospital inpatients (Sri Lanka), blood donors (Estonia, Brazil, India, Sri Lanka), and participants recruited during a national HIV sentinel surveillance sampling frame (Morocco). Analyses were stratified according to country, sex, and age (for the adult groups).
Differences in proportions were tested using the χ2 test. Logistic regression was used to examine differences in age and sex specific prevalence by country, using Morocco, as the reference. The odds of HSV-2 infection among individuals with and without HSV-1 was calculated in adults aged 20 years and over who had been tested for both HSV-1 and HSV-2. The analysis was restricted to those aged 20 and over (89.9% of sample) on the basis that the majority of these would be sexually active and hence have the potential to have been exposed to each virus.
Ethical issues
The ethics review boards of the respective institutions approved the study. The samples were tested in an anonymised fashion.
RESULTS
Overall, 13 986 samples were included in the study; 45% of samples (n=6269) were collected from women, 32.7% from men (n=4573), and 22.3% (n=3144) from children and adolescents (age 0–19 years). The majority (88%) were from people resident in urban areas. A detailed breakdown of the number of specimens tested from each country is given in table 1⇑.
Epidemiology of HSV-1
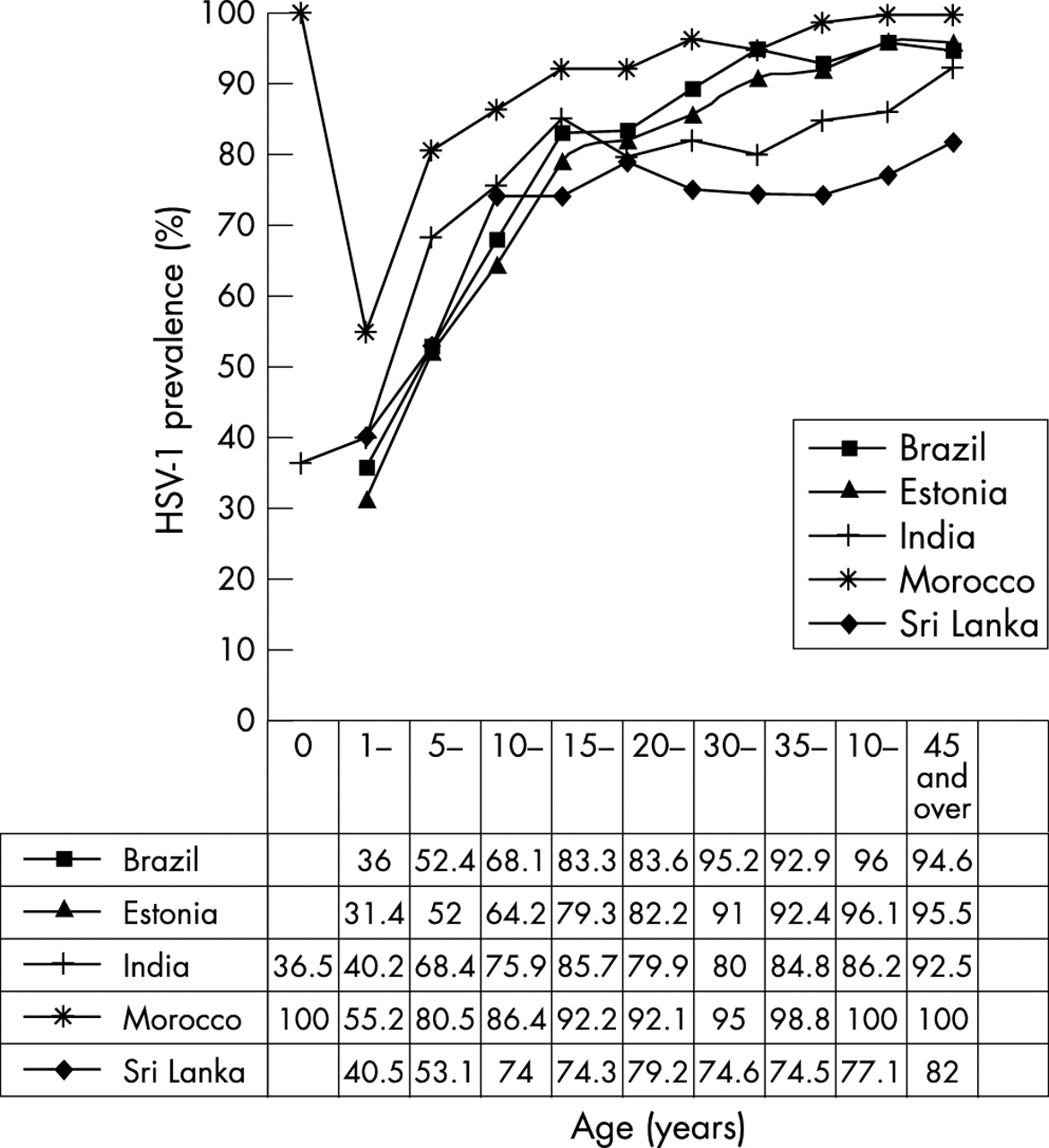
The HSV-1 seroprevalence among male adults at different sites ranged from 78.5%–93.6% and among female adults from 75.5% to 97.8%. The age specific HSV-1 seroprevalences are shown in figure 1⇓. At all sites HSV-1 seroprevalence increased significantly with age (t test for equality of mean ages among people who are HSV-1 positive and who are HSV-1 negative, p<0.001 for all countries) in both men and women. There were significant differences in the age specific prevalence between countries, with all countries having significantly lower risk of infection than Morocco (table 2⇓). The age at which 25%, 50%, and 75% of the population became HSV-1 seropositive also varied by country (table 2⇓).
Odds of infection with HSV-1 and HSV-2 by country after adjusting for age (excluding STD clinic attenders from Sri Lanka)

HSV-1 seroprevalence (%) by age group and country, males and females combined.
Epidemiology of HSV-2
The crude HSV-2 prevalences by country, sex, and population type are shown in table 3⇓ (see STI website for details).
Crude HSV-2 rates by target group and country
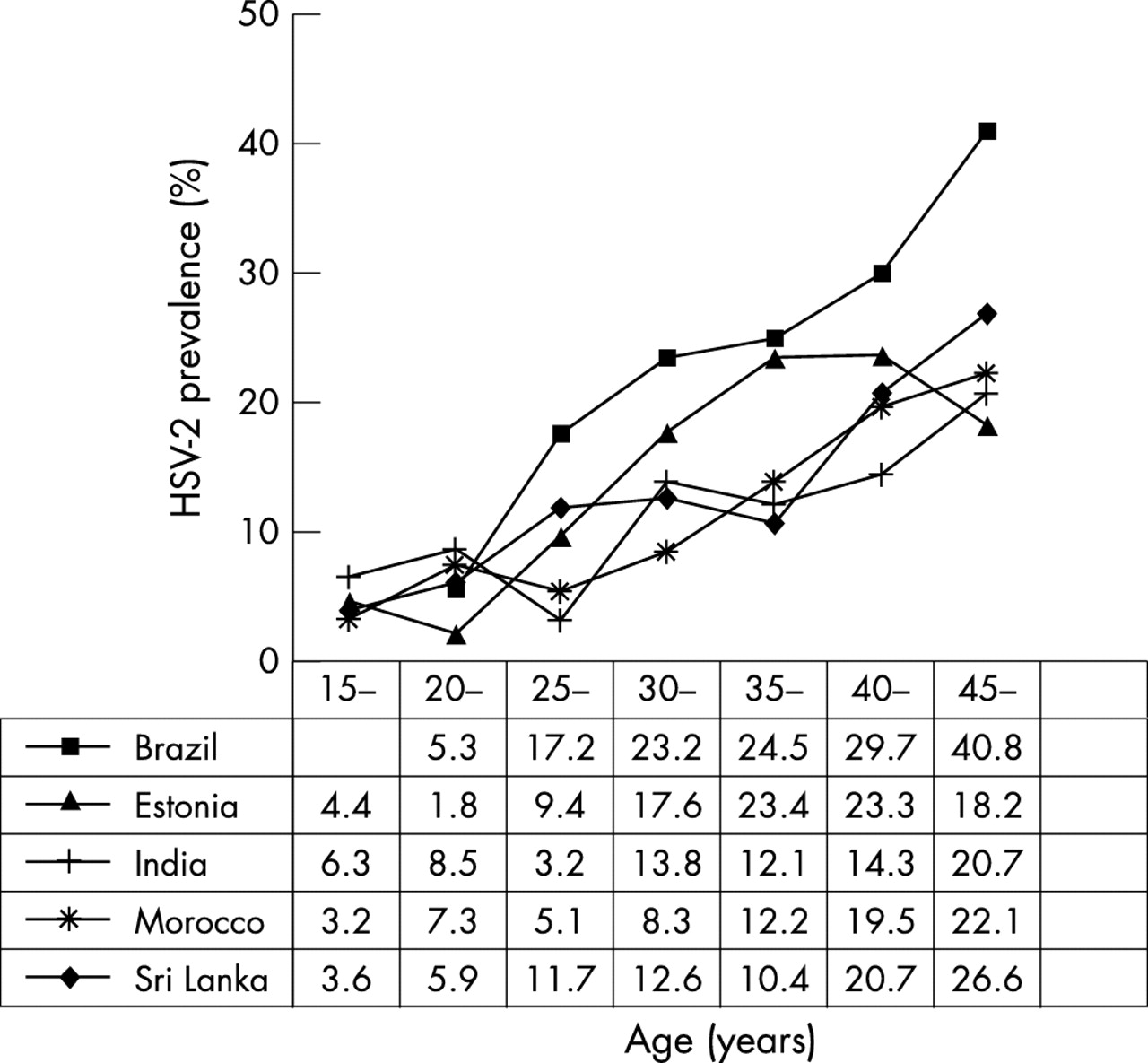
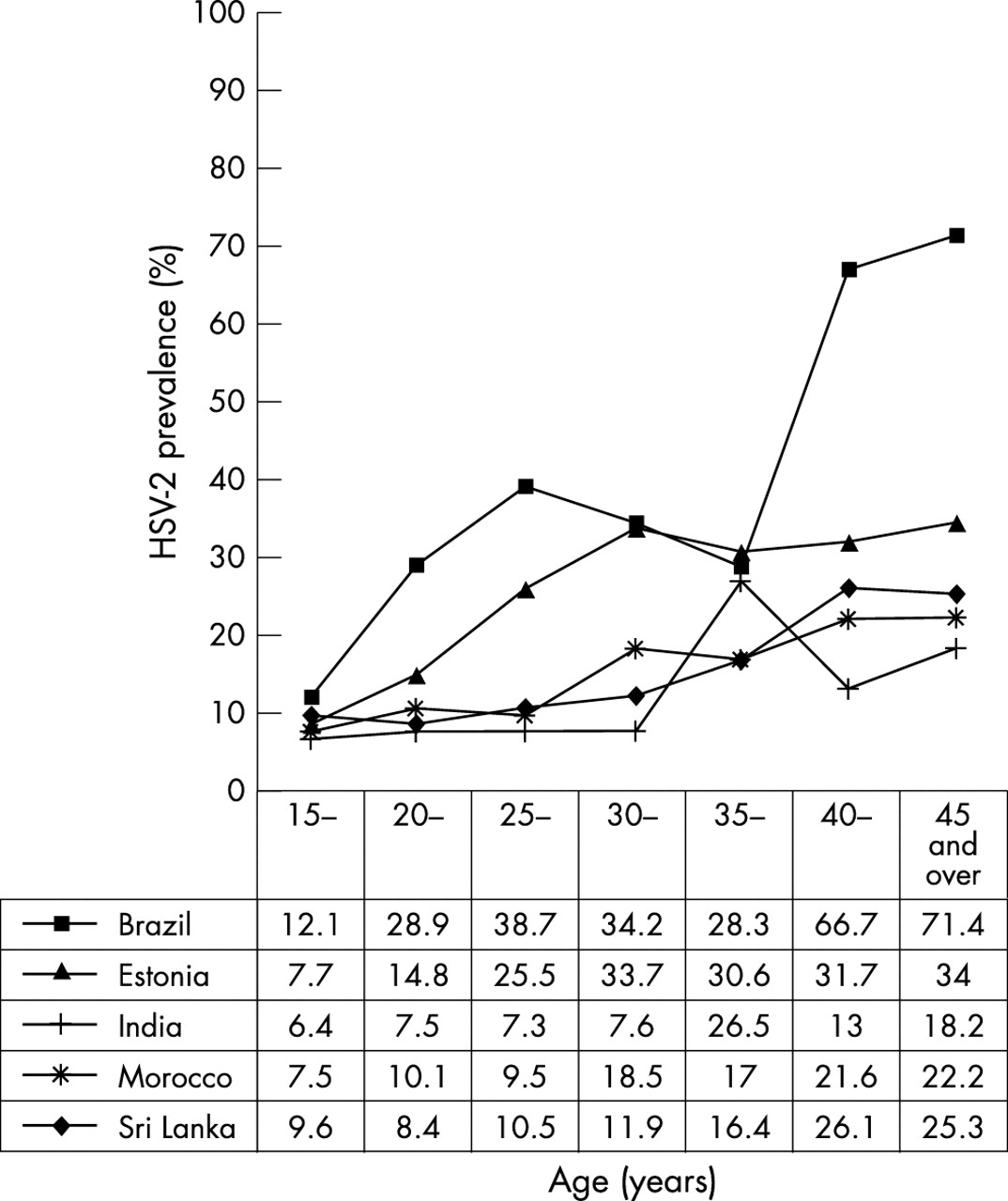
The age specific seroprevalences are shown in figure 2⇓ (for women) and figure 3⇓ (for men). In all countries HSV-2 seroprevalence increased significantly with age (t test for equality of mean ages among people who HSV-2 positive and HSV-2 negative, p<0.01 for all countries).

HSV-2 seroprevalence (%) among adult females by age and country (excluding STD clinic attendees).
{kind=link}
{kind=link}
{kind=link}
HSV-2 seroprevalence (%) among adult males by age and country (excluding STD clinic attendees).
The age and sex adjusted odds ratios of HSV-2 relative to Morocco for low risk men and women are shown by country in table 2⇑.
Overall, the odds of HSV-2 infection among adults (aged 20 years and over) with HSV-1 infection compared to those without was 1.32 (95% CI 1.12 to 1.55).
In Brazil, Estonia, India, and Sri Lanka all the samples collected from children were tested for antibodies to HSV-2 (n=2510). The HSV-2 seroprevalence was 0.5% (95% CI: 0.1 to 0.9) in Estonia, 2.2% (95% CI: 0.7 to 3.7) in India, 2.4% (95% CI: 1.0 to 3.8) in Brazil, and 4.8% (95% CI: 2.8 to 6.8) in Sri Lanka. Fifteen of the 21 seropositive sera taken from 433 children in Sri Lanka were retested using the reference assay.14 Only 3/10 gave positive results in both assays.
DISCUSSION
This study describes the age and sex specific seroprevalence of HSV-1 and HSV-2 in selected populations in Brazil, Estonia, India, Morocco, and Sri Lanka. These data confirm that the majority of infections with HSV-1 occur during childhood, although the age of acquisition varies between countries. By contrast, very few children were found to be infected with HSV-2. The low rate of confirmation of children’s HSV-2 positive sera from Sri Lanka suggests that a proportion of these sera represent false positive results, as might be anticipated in a very low prevalence population with the test characteristics described. The proportion of adults infected with HSV-2 increased with age in all communities and, overall, women had higher rates of infection than men, although this was not the case in India. Again the rate of HSV-2 infection varied between countries with Brazil having the highest age specific rates of infection for both men and women.
While the pattern and distribution of HSV-2 infection is becoming increasingly understood, relatively few studies to date have examined the seroprevalence of HSV-1. These data confirm that universal infection with HSV-1 early in childhood is not the norm. Infection during adolescence appears to be common in both Brazil and Estonia. Later acquisition of HSV-1 may be altering the epidemiology and presentation of genital herpes in these countries. A recent serological survey of over 5000 samples collected as part of the UK PHLS serosurveillance programme showed that the rate of infection among 10–14 year olds had dropped from 34% in 1986–7 to 24% in 1994–5,15 which has been accompanied by an increase in the proportion of first episode genital herpes cases due to HSV-1.2,3 Understanding the seroepidemiology of HSV-1 in children is critical to defining HSV vaccine strategies, if a vaccine that only worked in people who are HSV naive is to be further investigated. Such a vaccine would have no practical use in countries with high rates of HSV-1 in early childhood as we have shown occurs in India, Morocco, and Sri Lanka and, possibly, Brazil and Estonia as well.
Previous studies have shown conflicting evidence concerning the protective effect of HSV-1 for HSV-2, with some studies suggesting it has a protective effect4,16 and others finding no evidence of this.17,18 In this study, we did not find that having HSV-1 infection reduced the likelihood of HSV-2. Individuals aged 20 years and over with HSV-1 antibody were significantly more likely to be infected with HSV-2 than those without.
In developing countries, the major public health importance of HSV-2 relates to its potential role in facilitating HIV transmission. However, limited data on HSV-2 prevalence are available from many parts of the world, especially eastern Europe, Asia, and South America. A recent workshop conducted under the auspices of UNAIDS and WHO9 reviewed existing knowledge concerning the epidemiology and control of HSV-2, and its interaction with HIV. Experts concluded that estimates of HSV and HIV infections were needed by sex and age group in order to explore possible differences in the effect of HSV-2 on HIV acquisition between males and females, and to determine target groups for interventions. Although data on sexual behaviour were not collected in this study, the high HSV-2 seroprevalence found in Brazilian and Estonian women may indicate a high risk for STD and HIV exposure in those populations. Rates of bacterial STDs are also high in eastern Europe.19 These data suggest that STD/HIV prevention should be a priority in order to prevent the emergence of an HIV epidemic in Estonia.
These data were generated from various hospital populations and convenience samples within the five countries studied. Although not strictly representative of the general population of those countries they do provide useful insight into the extent of infection and how it varies with age and sex and as such would provide a useful benchmark for sample size estimates for more definitive epidemiological or intervention studies.
STI eLetters
Letters on the following papers have been published recently as rapid responses on the STI website. To read these letters visit www.stijournal.com and click on “Read eLetters”:
Diagnosis and treatment of presumed STIs at Mexican pharmacies: survey results from a random sample of Mexico City pharmacy attendants OpenUrlAbstract/FREE Full Text
Male circumcision: an acceptable strategy for HIV prevention in Botswana OpenUrlAbstract/FREE Full Text
Sexual health–health of the nation OpenUrlFREE Full Text
If you would like to post an electronic response to these or any other articles published in the journal, please go to the web site, access the article in which you are interested, and click on “eLetters: Submit a response to this article” in the box in the top right hand corner.
Acknowledgments
The authors wish to thank all those who contributed to the collection of samples in the sites.
The study was supported by a grant from GlaxoSmithKline (GSK).
CONTRIBUTORS
FC, PM, NJR, and DB designed the study and contributed to analysis; RF was the overall study coordinator and carried the statistical analysis with FC; DB and RG coordinated the laboratory aspects; SA, AU, SR, REA, MR, NPSC were the centres’ coordinators; FC and PM wrote the first draft of the paper to which all authors contributed.
Conflict of interest: NJR is an employee of GSK. FC has acted as a consultant for GSK. FC, RF, and DB have all accepted funding from GSK to attend meetings