Article Text

Abstract
Objectives: This intervention linked research aimed to reduce prevalence of Neisseria gonorrhoeae (Ng) and Chlamydia trachomatis (Ct) among female sex workers by means of one round of presumptive treatment (PT), and improved prevention and screening services.
Methods: A single round of PT (azithromycin 1 g) was given to all female sex workers reached during a 1 month period of enhanced outreach activity. Routine sexually transmitted infection (STI) screening services were successfully introduced for two groups of unregistered sex workers who work in brothels (BSWs) and on the street (SSWs). No changes were made to existing screening methods for registered sex workers (RSWs) or lower risk guest relations officers (GROs). Cross sectional prevalence of Ng and Ct was measured by PCR on three occasions, and stratified by type of sex work. Ng/Ct prevalence was assessed twice in clients of BSWs.
Results: Prevalence of Ng and/or Ct at baseline, 1 month post-PT, and 7 months post-PT was BSWs: 52%, 27%, 23%; SSWs: 41%, 25%, 28%; RSWs: 36%, 26%, 34%; GROs: 20%, 6%, 24%, respectively. Ng/Ct declines 1 month post-PT were significant for all groups. 6 months later prevalence remained low for BSWs (p<0.001), and SSWs (p = 0.05), but had returned to pre-intervention levels for the other groups. Prevalence of Ng/Ct among clients of BSWs declined from 28% early in the intervention to 15% (p = 0.03) 6 months later.
Conclusions: In this commercial sex setting, one round of PT had a short term impact on Ng/Ct prevalence. Longer term maintenance of STI control requires ongoing access to effective preventive and curative services.
- BSWs, brothel based sex workers
- Ct, Chlamydia trachomatis
- GROs, guest relations officers
- Ng, Neisseria gonorrhoeae
- PCR, polymerase chain reaction
- PT, presumptive treatment
- RSWs, registered sex workers
- SHCs, social hygiene clinics
- SSWs, street based sex workers
- STI, sexually transmitted infections
- HIV prevention
- STI
- Philippines
- presumptive treatment
- sex work
Statistics from Altmetric.com
- BSWs, brothel based sex workers
- Ct, Chlamydia trachomatis
- GROs, guest relations officers
- Ng, Neisseria gonorrhoeae
- PCR, polymerase chain reaction
- PT, presumptive treatment
- RSWs, registered sex workers
- SHCs, social hygiene clinics
- SSWs, street based sex workers
- STI, sexually transmitted infections
Sex work carries occupational risks, not least of which is frequent exposure to sexually transmitted infections (STI). STI prevalence among sex workers in low income countries often surpasses 50% and may reach 80–90% when chronic viral infections are included.1 Sex workers also face extremely high risk of sexually acquired HIV infection with incidence rates as high as 17 per 100 person months.2 Yet it is estimated that only 16% of sex workers in low and middle income countries have access to even basic HIV prevention services.3
Sex workers, once infected, can transmit STIs and HIV to a far larger number of susceptible clients, who serve as efficient “bridge” groups for even wider transmission.4 Because of this multiplier effect, effective interventions with sex workers and their clients can avert many more infections than would be prevented by general population strategies alone.4,5 Empirical data from Asia and Africa confirm that interrupting transmission in commercial sex networks can lead to large reductions in community HIV and STI prevalence, and reverse rapidly growing epidemics.6,7,8,9,10,11
Both condom promotion and STI case finding are important for decreasing STI and HIV transmission in sex work settings.12–16 Case finding is expensive, however, and commonly available methods for identifying STIs in women are neither sensitive nor specific. Presumptive treatment in high risk populations is an alternative that has been shown to contribute to community STI control in several settings.17–19
By definition, however, presumptive treatment strategies are temporary measures; as prevalence falls, the epidemiological justification for the intervention weakens.19 In order to maintain reduced prevalence, other control measures—condom promotion, effective screening, and treatment programmes—must be in place.
In the Philippines, a network of social hygiene clinics (SHCs) provides STI screening and treatment for registered female “entertainment workers” in over 140 cities, in some sites screening over 1000 women weekly. The effectiveness of these services is unclear, however. Cervical Gram stain, used in SHCs to screen for gonorrhoea and chlamydia, has low sensitivity to detect infection,20 and clinical examinations are not done systematically. Moreover, some categories of entertainment workers are exempt from regular checkups, and most freelance sex workers are either not eligible or avoid the system entirely. Despite these limitations, HIV prevalence remains low in the Philippines even among sex workers.21 Curable STI rates are high, however, with predominantly non-ulcerative patterns.21,22
Angeles City is a priority area for STI control and HIV prevention. Formerly the site of a large US military base, the city’s numerous “entertainment establishments” now attract foreign tourists and local men. At the time of the intervention, an estimated 2000–2500 women were working as sex workers in Angeles. Registered sex workers (RSWs) employed by licensed establishments receive weekly checkups at the local SHC. Unregistered sex workers who work in brothels (casas) or on the street typically have more clients, poorer access to services, and higher STI prevalence.23,24 In a recent study in Angeles, gonorrhoea prevalence was 38% among unregistered compared to 15% among RSWs, while chlamydial infection was similar in the two groups (37% v 35%); the majority of these infections were asymptomatic.25,26
To address gaps, preventive and curative interventions targeting all categories of sex workers in the “entertainment industry” in Angeles City were strengthened. The objective of this intervention research was to evaluate changes in STI prevalence following implementation of these interventions.
METHODS
This intervention was implemented between January and October 2001. The first intervention objective was to rapidly reduce the prevalence of Neisseria gonorrhoeae (Ng) and Chlamydia trachomatis (Ct) by providing a single round of presumptive treatment (PT) to female sex workers. The second was to maintain reduced Ng/Ct prevalence by strengthening preventive and curative services.
Evaluation of the interventions consisted of cross sectional assessments of behaviour, gonococcal, and chlamydial prevalence among female sex workers and clients. Ethics review committees of the Department of Health/Philippine Council for Health Research and Development, and Family Health International approved the study protocol.
Intervention phase 1—a single round of presumptive treatment
All female sex workers in Angeles City were offered PT during a 1 month period. In order to reach the widest population of sex workers, peer educators from the SHC and several non-governmental organisations (NGOs) extended outreach to both registered and unregistered sex workers. At recruitment staff explained the objectives of the intervention and the benefits and limitations of PT to potential participants. They explained that treatment was only effective for a few specific STIs, that participation in the programme was voluntary, and was not a substitute for other preventive measures. Participants who agreed were given a supervised 1 g dose of azithromycin as PT for gonococcal and chlamydial infections with a small snack to reduce gastrointestinal side effects. Any participant with signs or symptoms consistent with vaginitis or genital ulcer received additional treatment based on national guidelines. Condom use was promoted and condoms demonstrated and supplied at each outreach and clinic encounter.
Intervention phase 2—strengthened clinical services
Recommendations were made for improving existing screening methods used with RSWs at SHC, and for establishing satellite clinics for unregistered sex workers who did not have access to services.
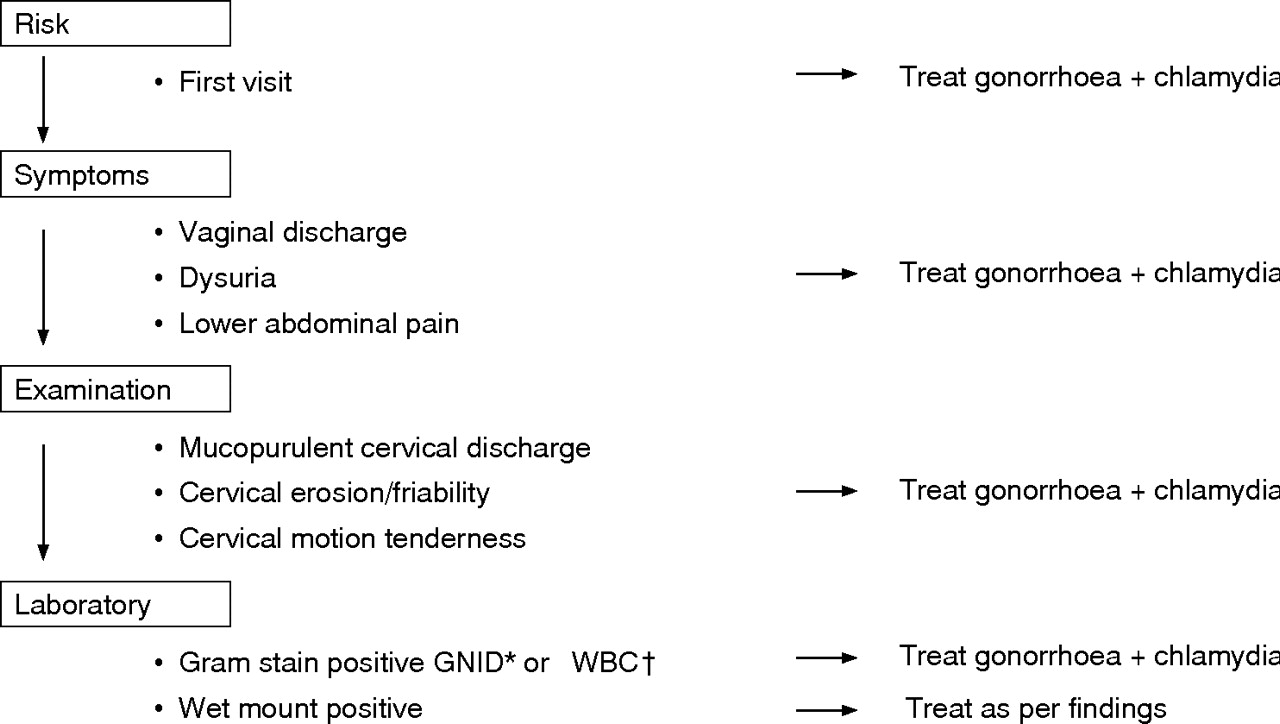
Figure 1 shows the recommended STI management algorithm for sex worker visits. In fact, changing existing SHC services proved difficult and screening continued using existing methods (based on Gram stained cervical smears) that permitted rapid processing of hundreds of women per day. The recommended algorithm was implemented only at the new satellite clinics serving unregistered sex workers.

{kind=link}
STI management algorithm. *Gram negative intracellular diplococci; †more than 20 white blood cells per high power field.
Intervention assessments
Three cross sectional behavioural and STI surveys of sex workers were conducted: round one (R1) at the time of PT, R2 1 month later, and R3 7 months after PT. Two cross sectional surveys of clients were carried out at the time of the second and third sex worker surveys.
Female entertainment workers who had sexual intercourse during the week before interview were systematically recruited as follows:
Among sex workers with health certificates (municipal registration):
-
Registered sex workers (RSWs) are establishment based, generally work in “go-go” bars catering to foreigners and possess health certificates issued by SHC. Every fifth RSW attending SHC for routine visits was eligible.
-
Guests relations officers (GROs) work in karaoke bars with a largely Filipino clientele, and possess health certificates. Every third GRO contacted by study staff at their workplace was eligible.
Among sex workers without health certificates (unregistered):
-
Street based sex workers (SSWs) serving mostly Filipino clients were approached in streets, parks, theatres, and cruising areas. SSWs were asked to refer their peers (snowballing technique).
-
Brothel based sex workers (BSWs) serving primarily Filipino clients were recruited in brothels and at a satellite clinic established in their community.
Sample size per survey round was 300 for RSW and 100 each for GRO, SSW, and BSW. All SSWs and BSWs contacted were eligible.
Clients were defined as men who had sex with a female sex worker in the last month, and were recruited by a researcher who approached men at brothels with the assistance of brothel staff. The sample size for clients was 100 per survey round.
Data collection
Study participants were given a standard questionnaire covering sociodemographic profile, duration of sex work, sexual behaviours, number of partners, history of previous STI and presence of STI symptoms. Treatment was provided to symptomatic individuals based on the Philippines’ national syndromic guidelines, and condoms were promoted, demonstrated, and provided.
Laboratory methods
Urine samples of 10–15 ml were collected using sterile polypropylene tubes, and stored at 4°C before being transported on ice to the central laboratory (SACCL) on a daily basis where they were frozen at −70°C until processed. Urine was tested for C trachomatis and N gonorrhoeae by polymerase chain reaction (PCR) using Amplicor CT/NG test (Roche Molecular Systems, Branchburg, NJ, USA) according to the manufacturer’s instructions.
Data analysis
Data from interviews, clinical, and laboratory examinations were entered, validated, and analysed using Epi-Info 6.0 and Stata 6 software. Pearson’s χ2 test was used to compare proportions.
RESULTS
Outreach and presumptive treatment
In all, 1938 female entertainment workers accepted PT, close to the estimated sex worker population of 2000–2500 in Angeles.
Cross sectional surveys
The baseline survey (R1) was done at the time of PT in February/March 2001, R2 in March/April, and R3 in October. The total sample included 1651 sex worker contacts during three rounds. The proportion of women surveyed at rounds R2 and R3 who reported having received PT during round 1 was 50% and 17% (RSW), 75%, and 33% (GRO), 63% and 32% (SSW), and 79% and 70% (BSW), respectively.
Demographic and behavioural characteristics
Table 1 summarises demographic and behavioural characteristics of 1130 women sampled at least once during the three rounds. No significant differences were found among women attending for the first time during initial and subsequent survey rounds. Reported numbers of sex partners during the week before baseline interview varied with BSW having significantly higher numbers of partners—including more non-regular and paying regular clients—than other groups (p<0.001). Numbers of non-paying regular partners was similar across groups (range 0–3).
Demographic and behavioural characteristics of female sex workers (n = 1130*) at first contact, Angeles City, Feb–Oct 2001
At the PT contact (R1), 44% of women reported using a condom the last time they had sex. Condom use varied by category of sex worker and partner type.
STI prevalence
Table 2 shows gonococcal and chlamydial prevalence rates. One month post-PT (R2), prevalence of gonorrhoea and/or chlamydial infection (Ng/Ct) was reduced by 28% (36.3% to 25.8%, p = 0.02) for RSW, 70% (20.0% to 6.0%, p = 0.002) for GRO, 39% (41.0% to 25.0%, p = 0.02) for SSW, and 47% (51.6% to 26.6%, p<0.001) for BSW.
Prevalence of gonorrhoea (Ng) and chlamydia (Ct) by group and by survey round, Angeles City, Feb–Oct 2001
At the second assessment 6 months later (R3), Ng/Ct prevalence was maintained at the reduced level for BSW (23.0%, p<0.001) and SSW (28.0%, p = 0.05) but had returned to pre-intervention levels for RSW (33.7%) and GRO (24.0%).
Greater reductions in Ng/Ct prevalence at round 2 were seen among less mobile groups (a higher proportion of whom had received PT 1 month earlier). Table 3 presents Ng/Ct prevalence rates for sex workers who had received PT during the initial intervention phase compared to those who had not.
Prevalence of gonorrhoea (Ng) and/or chlamydia (Ct) stratified by exposure to PT at R1, by group and survey round, Angeles City, Feb–Oct 2001
Differences in prevalence compared to baseline were significant for all groups at R2 but only for BSW and SSW 6 months later (R3). Exposure to prevention interventions was comparable for all groups (based on outreach reports). Reported condom use at last sex increased slightly overall but differences were significant only for RSW (p = 0.01).
STI screening improved greatly for BSW and SSW (who previously had no access) while there were no changes in existing services for RSW and GRO. As a result, the former were more likely to receive treatment for STI during the post-PT period. Only 2–3% of RSW screened by Gram stain at SHC were treated for infection each month, similar to treatment rates before the intervention. In comparison, 21% of BSW screened at newly established clinics using the clinical/laboratory algorithm (fig 1) received treatment during the first month, gradually declining to 8% 6 months later.
Among clients of BSWs sampled 1 month after the PT (n = 100) and again 6 months later (n = 100), Ng/Ct prevalence declined 46%, from 27.6% to 15.0% (p = 0.03) (table 2).
DISCUSSION
This intervention linked research assessed several intervention components introduced to strengthen existing STI control efforts among sex workers in Angeles. Our findings suggest that (1) one time presumptive treatment can help reduce STI prevalence for rapid but short term control, that (2) ongoing STI screening using sensitive methods, together with outreach and condom promotion are important for sustaining STI reductions, and that (3) interventions that effectively reduce STI prevalence among sex workers can have broader public health effects, extending at least to their clients.
In Angeles, as elsewhere, conditions of sex work influence vulnerability, risk, and STI prevalence. Differences between types of sex work proved important for orienting services. Five out of six women (RSW and GRO) reached during the month long PT intervention phase were already “in the system,” receiving some form of regular STI screening through social hygiene clinics. The remaining women worked in brothels or on the street and, being unregistered, did not have access to services. Importantly for STI control, these unregistered sex workers reported more clients, had the lowest condom use, and highest STI rates.23,26
It was not difficult to reach these sex workers. Outreach efforts by peers and NGOs were highly effective in mobilising large numbers of both registered and unregistered sex workers for PT and in promoting services. Peer involvement and community mobilisation are critical factors in uptake of interventions with sex workers.27,28 Organised sex workers are also better able to demand condom use and safer working conditions, and to resist abusive conditions such as harassment and trafficking.28
Presumptive treatment reduced STI prevalence in the short term. One round of presumptive treatment was followed by significant STI declines in all groups 1 month later, similar to experience reported elsewhere.29 In Angeles, however, rapid turnover among some groups of sex workers quickly diluted the effect of one time PT. Frequent arrival of new sex workers into an area argues for incorporating PT and/or screening into routine sex worker services along with outreach efforts to reach new sex workers.
Sustaining lower STI rates clearly requires more than one time presumptive treatment. By the final assessment round, 7 months post-PT, Ng/Ct prevalence remained low for BSW and SSW but had returned to baseline for RSW and GRO. It is not possible to say with certainty which intervention components were responsible for these differing outcomes. Exposure to condom promotion was similar for all groups and no significant changes in reported condom use (except RSW) or numbers of partners were measured for any group over the short intervention period. One apparent difference was the higher rate of treatment at the newly established screening services for unregistered sex workers compared to rates at SHC. Sensitive screening criteria (fig 1) were successfully introduced in newly established services for BSW and SSW. Established routines at SHC proved difficult to change, however, and treatment rates for RSW and GRO remained low.
Notably, unregistered BSWs, who initially had the highest rates of risk behaviours and infection, had the lowest STI prevalence at the end of the evaluation period, and STI prevalence had fallen an equivalent amount among their clients as well. Since only 5% of these clients reported condom use at last sex with their regular non-commercial partners, lower STI prevalence in this bridge population should also benefit women with lower risk behaviour.
Holmes et al drew similar conclusions in Olongapo City, Philippines, in 1967, although the sequence of interventions was different.30 Weekly screening of registered sex workers by gonococcal culture, and treatment of contacts named by US Navy servicemen reduced gonorrhoea prevalence among registered sex workers from 11.9% to 4.0% within 4 months, and gonorrhoea incidence in servicemen at nearby Subic Bay fell by half. A single round of “selective mass treatment” (comparable to presumptive treatment) had a temporary additional benefit that was not sustainable without other interventions.
In Angeles, as in Olongapo more than 30 years earlier, presumptive treatment facilitated STI control by bringing down STI rates rapidly, but benefits were short lived without additional intervention. Regular STI screening using sensitive methods appears to contribute to longer term control. Regular contact with health services also allows for a relationship that can encourage safer behaviours including condom use.1,6 In both places, important public health benefits—lower STI burden for sex workers and halving of rates among male bridging groups—were evident.
Key messages
-
One time presumptive treatment may help to quickly reduce Ng/Ct prevalence in commercial sex networks but is not sufficient for long term STI control
-
Ongoing services including outreach, condom promotion, and STI screening appear to be important for sustaining STI control
-
Effective interventions with sex workers can have a broader public health impact
Acknowledgments
This study was supported by the US Agency for International Development (USAID) through Family Health International’s (FHI) AIDS Prevention and Care (IMPACT) projects, Cooperative Agreement HRN-A-00-97-00017-00. The views expressed here do not necessarily reflect those of USAID or FHI.
CONTRIBUTORS TW was the principal investigator who initiated and oversaw all aspects of the study design, implementation, analysis and write up; ERR was the principal field investigator with responsibility for implementation of the study protocol and initial data analysis; RS provided technical assistance in the design, implementation, analysis and write up; TAE contributed to the study design and implementation and oversaw clinical teams involved in interventions and data collection; MCR provided review of study protocol and technical backup to the field researchers; MCL-Q provided review of study protocol and technical backup to the field researchers; GN provided technical input in design, analysis, and manuscript review; GD provided technical input in design, analysis, and manuscript review.
REFERENCES
Footnotes
-
The authors are grateful to the following for their support of the study: the Philippine National AIDS Council (PNAC), for providing azithromycin and other STI drugs for treatment of study participants, Angeles City Health Office Angeles Social Hygiene Clinic; Program for Appropriate Technology in Health (PATH) Foundation, Pearl S Buck Foundation and Reach Out for their assistance in data collection, and JICA-STD/AIDS Cooperative Central Laboratory.
-
The authors declare no competing interests.