Article Text

Abstract
Objective: To describe a new disaggregate surveillance system covering key diagnosed sexually transmitted infections in a UK locality.
Methods: The Avon System for Surveillance of Sexually Transmitted Infections (ASSIST) collects computerised person- and episode-based information about laboratory-diagnosed sexually transmitted infections from genitourinary medicine (GUM) clinics, the Avon Brook Clinic, and the Health Protection Agency and trust laboratories in primary care trusts in Avon. The features of the system are illustrated here, by describing chlamydia-testing patterns according to the source of test, age and sex, and by mapping the distribution of chlamydia across Bristol, UK.
Results: Between 2000 and 2004, there were 821 685 records of tests for sexually transmitted infections, with 23 542 positive results. The proportion of tests and positive results for chlamydia and gonorrhoea sent from general practice increased over time. Most chlamydia tests in both GUM and non-specialist settings were performed on women aged >25 years, but positivity rates were highest in women aged <25 years. The positivity rate remained stable between 2000 and 2004. Including data from all diagnostic settings, chlamydia rates were about twice as high as those estimated only from genitourinary clinic cases.
Conclusions: The ASSIST model could be a promising new tool for planning and measuring sexual health services in England if it can become sustainable and provide more timely data using fewer resources. Collecting denominator data and including infections diagnosed in primary care are essential for meaningful surveillance.
- ASSIST, Avon Surveillance System for Sexually Transmitted Infections
- GP, general practitioner
- GUM, genitourinary medicine
- NHS, National Health Service
Statistics from Altmetric.com
- ASSIST, Avon Surveillance System for Sexually Transmitted Infections
- GP, general practitioner
- GUM, genitourinary medicine
- NHS, National Health Service
The attributes and usefulness of surveillance systems for sexually transmitted infections should be evaluated in terms of their ability to provide information about numbers of cases of infection in defined populations, rates of infection in groups at high risk of infection, diagnostic and screening activity in different health service settings, and the impact of interventions.1,2 Data about sexually transmitted infections in Britain have been collected since 1917.3 The evolution of this system has led to the collection of aggregated surveillance data from genitourinary medicine (GUM) clinics in the UK using the KC60 form.4 However, this system has a number of limitations. First, surveillance data are based on total numbers of cases, and are collected only from GUM clinics without defined catchment populations.1,5,6 As a result, geographical and ethnic inequalities in the rates of sexually transmitted infections went unrecognised for many years.6–8 Second, the lack of denominator data hinders the interpretation of time trends, particularly for chlamydia. Third, it is currently impossible to monitor the increasing amounts of testing for sexually transmitted infections in primary care,9 as required by the National Strategy for Sexual Health and HIV, and the National Chlamydia Screening Programme.10
The Avon System for the Surveillance of Sexually Transmitted Infections (ASSIST) was designed to overcome some of the limitations of existing surveillance systems. Using the framework for evaluating public health surveillance systems provided by the United States Centers for Disease Control and Prevention,2 we report the development and outcomes of ASSIST with respect to five areas: (1) engaging stakeholders; (2) description of the system; (3) evaluation design; (4) performance of the system; (5) conclusions and recommendations.
METHODS
Stakeholders engaged
ASSIST was developed as a multidisciplinary collaboration, with funding and coordination from the South West Public Health Observatory. The stakeholders who contributed in establishing the system included local sexual health service providers, microbiology laboratories, primary care trusts, the Avon Health Protection Unit and the Health Protection Agency (steering group members are listed in the Acknowledgements).
Description of the surveillance system
The aims of the ASSIST system are: (1) to establish data collection and dissemination systems for routine reporting of sexually transmitted infections that can be used for national surveillance, local surveillance, research, audit and commissioning purposes; (2) to collect person- and episode-based data about all laboratory tests for sexually transmitted infections carried out in any National Health Service (NHS) setting; (3) to use the data to examine inequalities in the geography and epidemiology of laboratory-diagnosed sexually transmitted infections; (4) to assess sexual health service provision by different providers, and (5) to plan and monitor local services and interventions. Fig 1 describes the data flows and integration of ASSIST with clinical and laboratory sources of data, and also with existing public health authorities.
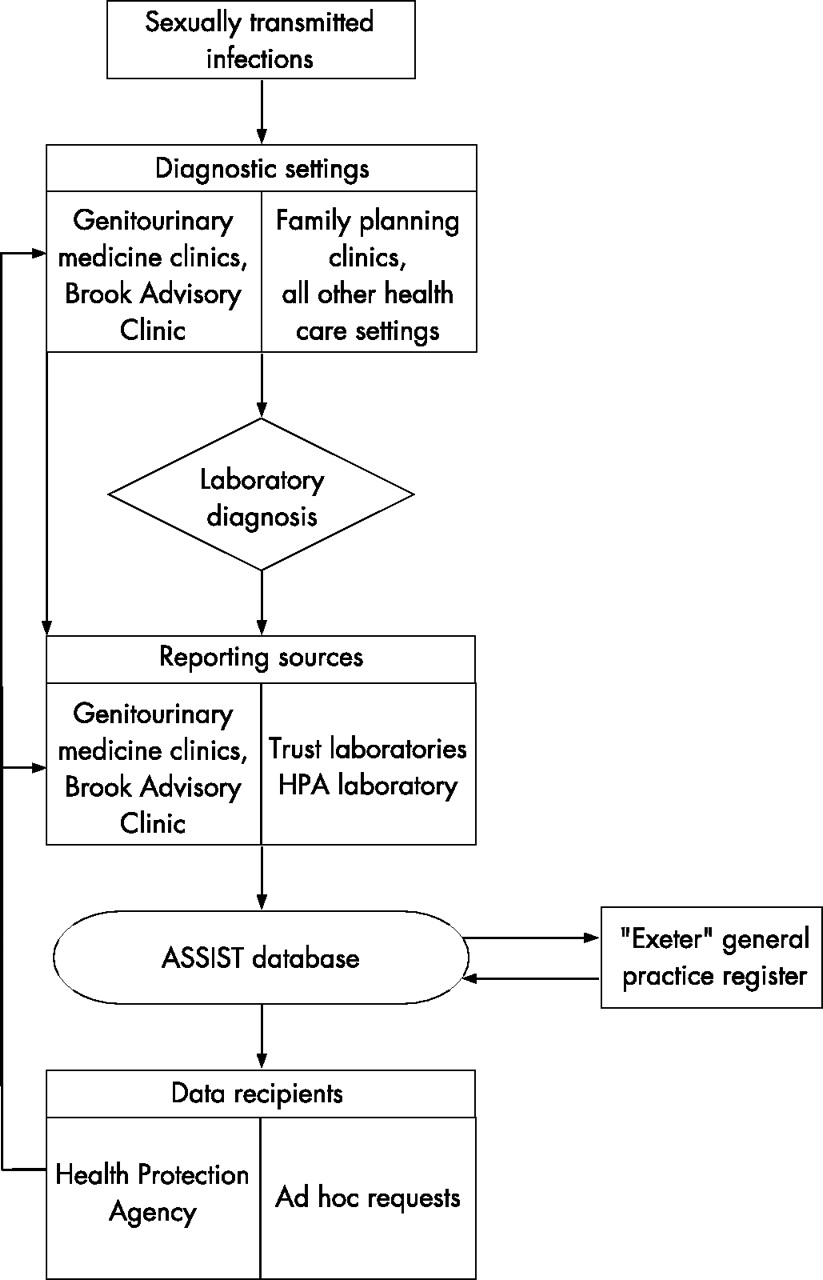
Flow chart showing information flows between reporting sources and the ASSIST database.
Population and setting
The former Avon Health Authority area (population 984 000) encompasses the urban populations of Bristol, Bath and Weston-super-Mare, and rural populations in North Somerset and South Gloucestershire in the UK. The area is served by four primary care trusts, three GUM clinics, the Brook Advisory Centre for young people and four NHS trust microbiology laboratories. The United Bristol Healthcare Trust, which housed the local Public Health Laboratory and National Genitourinary Infections Reference Laboratory before the formation of the Health Protection Agency, performs all laboratory tests for HIV, syphilis, hepatitis B and herpes in Avon, the majority of tests for chlamydia and positive confirmation tests for gonorrhoea, on behalf of other NHS trusts. The age and sex distribution of the Avon population is similar to that of England as a whole, although the proportion of people from minority ethnic groups is lower (4% vs 9%). In 2004, 1260 cases of chlamydia and 388 cases of gonorrhoea were reported through the KC60 system from GUM clinics in Bristol, Bath and Weston in UK.
Data collection from GUM clinics and laboratories
We collected electronic data annually retrospectively from 2000 and prospectively from 2002. The reporting sources are: departments of GUM, the Avon Brook clinic, and the Health Protection Agency and trust laboratories. Information technology or administrative staff extracted computerised data from their own systems. In two GUM clinics, we adapted data extraction software developed by the system suppliers for the Health Protection Agency’s Programme for Enhanced STI Surveillance (ProgrESS) project. Two laboratories set up their own data extraction routines, and the ASSIST public health information analyst set up data extraction routines in the other sites. Information on date of birth, sex, soundex code of surname and clinical person’s identification number was obtained from both clinics and laboratories (supplementary table 1 available online at http://sti.bmjjournal.com/suppl). Clinic data also included the postcode of residence, ethnic group, KC60 diagnosis code (genitourinary medicine clinics only) and date of attendance. The laboratory data also included the general practice code or setting where the specimen was obtained, the date the specimen was received, the type of specimen to be tested and the test result.
Total numbers of tests for, and diagnoses of, chlamydia and gonorrhoea reported to the Avon System for Surveillance of Sexually Transmitted Infections, 2000–2004
Data management, processing and linkage
The ASSIST database was developed by one full time public health information analyst, under the supervision of a clinical epidemiologist. The system uses a Microsoft Access relational database linking person-based information to attendances at clinics and episodes of infection. Postcode data are required for geographical mapping. This is obtained from patient-based records provided by the GUM clinics and the Brook Clinic. To obtain this information from other settings, a postcode has to be linked to laboratory records. Using combinations of soundex code,11 date of birth, gender and referring general practitoners (GP) practice code, we used algorithms to obtain likely matches with the GP patient registration system (fig 1). We identified duplicate records resulting from repeat tests conducted on the same person in different settings for the same episode, using combinations of patient identifier code, soundex code, other patient identifiers and test dates. We also checked records to assign the source of tests performed outside GUM clinics, particularly to distinguish between tests sent from general practitioners and those from family planning clinics situated in general practices.
Data protection, confidentiality and approval for surveillance
Data transfer, storage, confidentiality and system security comply with the requirements of the Patient Information Advisory Group (PIAG 1-07(l)/2004) and the project has been approved by all local Caldocott guardians and the South West Multi-centre Ethics Committee. Data are transferred on password-protected compact or floppy disks. Data access is restricted using password permissions on a secure server at the Health Protection Agency.
RESULTS
Baseline evaluation
The aim of this evaluation was to describe the baseline attributes of the ASSIST system to guide future data collection and system development. We have particularly focused on chlamydia infections to assess the attributes of the system, because increasing numbers of cases are diagnosed outside GUM clinics.
Attributes of the surveillance system
Simplicity, acceptability and timeliness
Data were collated only at yearly intervals. After setting up the routines, data extraction for laboratory and clinic staff was simple. Data processing within the ASSIST database was more complicated, because of the need to assign postcode data to records originating from laboratories, to de-duplicate records, to identify the source of tests received by the laboratories and to check the accuracy of the data. Only laboratory data up to 2002 have been matched to postcodes; 12% of chlamydia specimens could not be unambiguously assigned to general practitioners, family planning clinics or midwives running antenatal clinics.
Data quality, flexibility and stability
We included person-based data covering all three GUM clinics and the Avon Brook clinic (supplementary table 1 available online at http://sti.bmjjournal.com/suppl). Laboratory test results were obtained from the main laboratory from 1 January 2000 to 31 December 2004 (table 1) and from Weston laboratory from 1 January 2002. Overall, there were approximately 32 000 GUM clinic attendances and 200 000 laboratory tests per year.
Data completion was good. Using data from 2002, 100% (31 063/31 063) of clinic records and 98.6% (187 335/190 016) of laboratory records had date of birth; 100% (31 063/31 063) of clinic records and 99.5% (189 134/190 016) of laboratory records had sex recorded; and 99.9% (31 042/31 063) of clinic records and 92.2% (126 047/136 632) of laboratory records relating to non-clinic tests had a soundex code. Ethnic group was recorded in 79% (24 517/31 063) of clinic records. After correcting postcodes for obvious transcription errors, 75% (142 509/190 016) of laboratory tests were linked to a recognised postcode. We have not yet assessed the system’s flexibility and stability.
Sensitivity and representativeness
ASSIST collected testing data from all diagnostic settings. Between 2000 and 2004, there were 821 685 records of tests for sexually transmitted infections and 23 542 positive results (supplementary table 2 available online at http://sti.bmjjournal.com/suppl). There were 394 539 tests for chlamydia or gonorrhoea, and 20 377 positive results. Chlamydia testing has increased over time (table 1). GP accounted for 38.8% (16 385/42 231) of all tests in 2000, and for 54.7% (27 511/50 429) of tests in 2004. Among other service providers, the Brook Advisory clinic accounted for 2.2% (5040/225 412) of all chlamydia tests performed between 2000 and 2004 and for 5.4% (4810/86 419) in under 25-year-olds. Only 6.6% (14 905/225 412) of chlamydia tests were confirmed as originating from named family planning clinics, but this excluded some family planning clinic activity at general practice locations. The 21.0% (47 405/225 412) of other activity included inpatients, outpatients (including a small amount of confirmed antenatal clinic activity), accident and emergency and referrals from laboratories outside Avon.
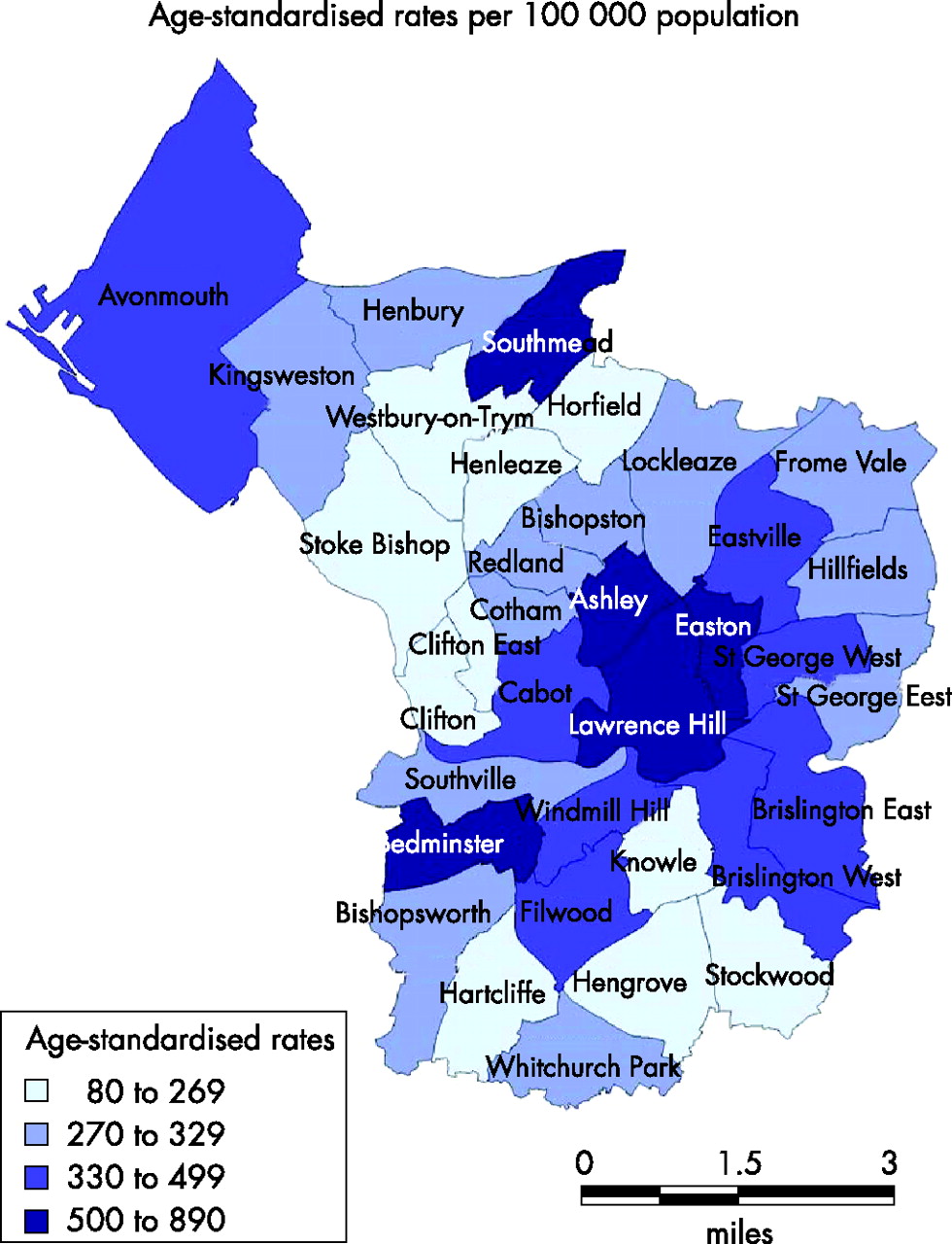
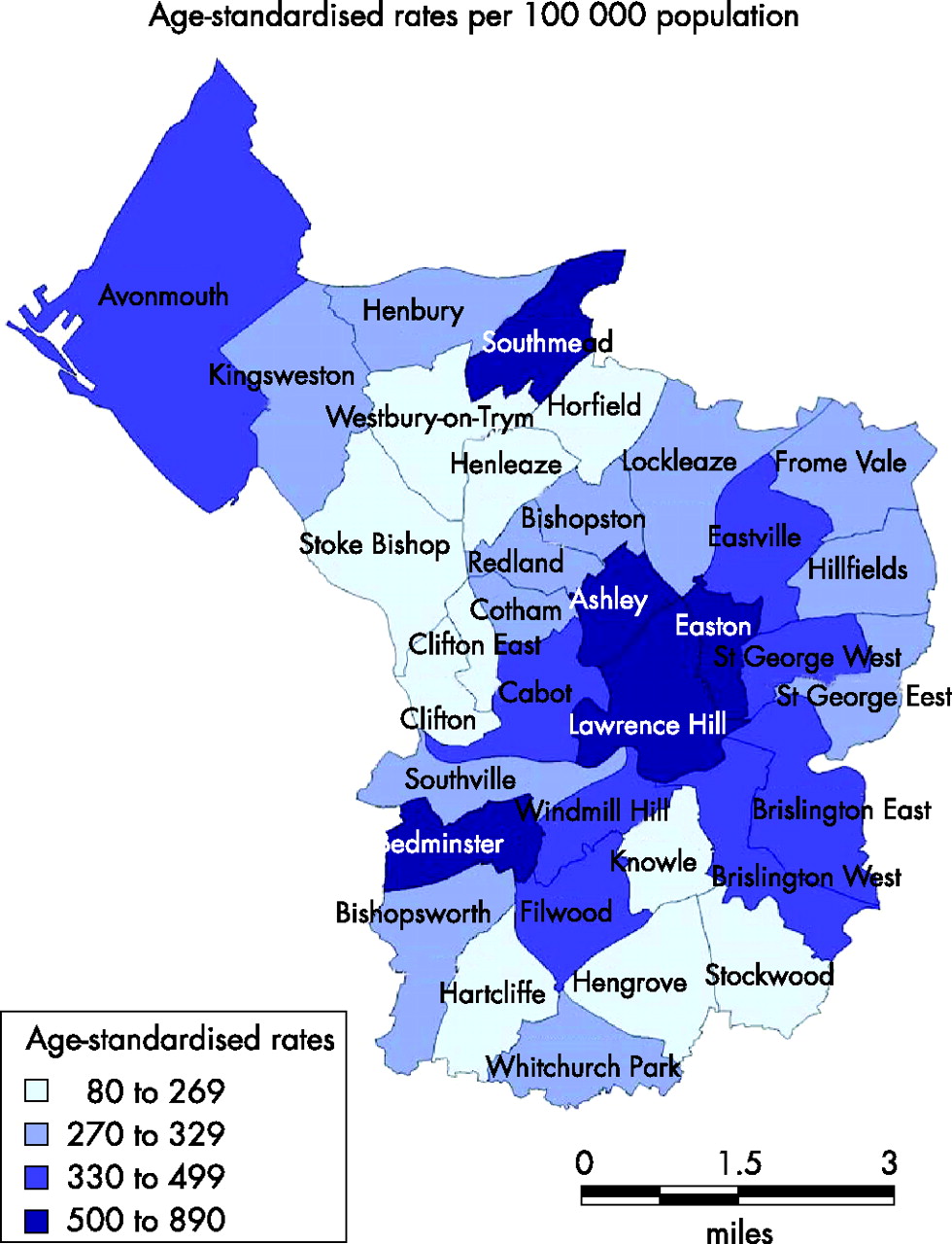
Figure 2 shows that, in both GUM clinics and general practice, most chlamydia tests were performed in people aged ⩾25 years, but that the highest proportions of positive test results were in under 20-year-olds: 15.1% (245/1624) and 12.2% (346/2826) in GUM clinics and primary care respectively. The population rate of chlamydia, on the basis of GUM clinic data, ranged from 200 to 300 episodes per 100 000, with a decrease over time (fig 3). When positive tests from all settings were included, the rate increased to around 600 episodes per 100 000. The chlamydia positivity rate remained stable. Figure 4 shows the geographical distribution of chlamydia in Bristol, UK, in 2002. The overall prevalence was 326 episodes per 100 000 population, with ward rates varying from 87 per 100 000 population in Stoke Bishop to 882 in Lawrence Hill.

Age distribution of chlamydia tests and positive results from genitourinary medicine clinics and general practice, 2004.

Rates of diagnosed chlamydial infection (per 100 000 population aged 15–59 years) in those attending genitourinary medicine clinics and all clinical settings, 2000–4.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Geographical distribution of chlamydia cases, Bristol primary care trusts: age-standardised rates per 10 000 population, 2002.
DISCUSSION
The ASSIST project demonstrates the feasibility of collecting both numerator and denominator data about sexually transmitted infections diagnosed in all settings. Rates of diagnosed chlamydia were about twice as high as those obtained from routine GUM clinic surveillance alone. The percentage of positive chlamydia tests remained stable between 2000 and 2004. The majority of chlamydia tests in both general practice and GUM clinics were performed over 25-year-olds.
Methodological issues
The main strength of ASSIST is its multidisciplinary infrastructure. This enabled us to collect data about laboratory-diagnosed sexually transmitted infections and testing in all clinical settings, to link records to geographical data, and to examine trends in data from 2000. The weaknesses of ASSIST relate to the complexity of linking geographical data and de-duplicating data about tests taken in different clinical settings. The project has not been integrated into routine service, and research funding provides limited support. The data have therefore been collected only once a year, and the most recent data are from 2004.
Comparison with other studies
The value of using disaggregated data from GUM to describe ethnic and geographical inequalities in sexual health has been widely demonstrated.7,8,12–14 Repeated prevalence surveys of people attending general practices have been suggested as a way of supplementing these surveillance data in the UK.15 Such surveys would be expensive, cover a limited number of infections and would still miss infections diagnosed in other settings.16 Surveillance systems that include laboratory reports of diagnosed infections have greater population coverage.17,18 Although they cannot be a substitute for well-conducted prevalence studies, they provide a complete picture of diagnosed sexually transmitted infections in a timely manner that allows trends to be monitored over time.
Meaning of the study
We have shown how the data collected about genital chlamydia infections increase our knowledge about time trends and diagnostic practices. The availability of denominator data is particularly useful, because it allows the number of positive chlamydia tests to be interpreted in the light of testing patterns. Chlamydia positivity rates in the area served by Avon primary care trusts do not seem to be increasing. This is different from the message portrayed in the national surveillance data, where the increasing number of positive tests is interpreted as being due to increased transmission.4 With the data available in ASSIST, we could examine testing and diagnostic practices by different providers. Previous studies have shown that most chlamydia tests in primary care are taken from women over 25 years of age, who have the lowest prevalence.9 What is more striking is that this was also the pattern in GUM clinics, which are assumed to serve young adult populations.
Implications for service delivery and research
Sexual health networks are now responsible for planning and commissioning sexual health services. Our project demonstrates the feasibility of collecting population level testing and diagnostic data across different service provider organisations. ASSIST also provides a mechanism for monitoring the effective screening rate of the chlamydia screening programme in England over time,19 because tests in the same person in different settings can be identified and de-duplicated, and the system can record the demographic data, and potentially the behavioural data, required by the Common Dataset for Sexual Health (Department of Health. http://www.cdssexualhealth.org.uk). The planned introduction of a new web-based system to automate data downloads and cleaning will improve timeliness and accessibility. We will explore the generalisability of ASSIST by implementing it through a further research project in Brent, London in 2006–7. The ASSIST model could be a promising new tool for planning and measuring sexual health services in England if it can become sustainable and provide more timely data using fewer resources.
Key messages
-
Exclusion of information from primary care and other clinical settings, and denominator data about the number of tests taken, limit the utility of existing UK surveillance for sexually transmitted infections.
-
The Avon System for Surveillance of Sexually Transmitted Infections (ASSIST) provides individual-based data about all tests and results for sexually transmitted infections according to infection, diagnostic setting, age, sex and area of residence.
-
The system shows that general practice accounts for an increasing proportion of tests and positive results for chlamydia and gonorrhoea, and that most tests for chlamydia testing in both genitourinary medicine clinics and general practice are performed in over 25-year-olds.
-
The ASSIST system could be a useful model for surveillance if it can become more timely and sustainable.
Acknowledgments
We thank the staff in clinics and microbiology laboratories who took the time and effort to provide information and aid data extraction. Members of the ASSIST steering committee are: Dr Charles Irish (Health Protection Agency), Dr Paddy Horner (Genitourinary Medicine, Bristol, UK), Dr Tracey Masters (community gynaecology), Dr James Stuart (Health Protection Agency) and Dr Kate Horn (Genitourinary Medicine, Bath, UK). We also thank Professor Selena Gray for providing the initial funding from the South West Public Health Observatory.
REFERENCES
Supplementary materials
Files in this Data Supplement:
Footnotes
-
Competing interests: None declared.
-
WS established the data collection systems and database for ASSIST, conducted the first analyses and wrote the first draft. KS updated the analyses and contributed to revising the text. JC provided advice about national surveillance systems and contributed to revising the text. PH provided access to genitourinary clinic data, contributed to the development and establishment of ASSIST and contributed to revising the final draft. NL conceived the idea for ASSIST, contributed to its establishment, and revised the draft manuscript. All authors approved the final draft.