Article Text

Abstract
Objectives: To test whether more women are screened for sexually transmitted infections when offered home-based versus clinic-based testing and to evaluate the feasibility and acceptability of self-sampling and self-testing in home and clinic settings in a resource-poor community.
Methods: Women aged 14–25 were randomised to receive a home kit with a pre-paid addressed envelope for mailing specimens or a clinic appointment, in Gugulethu, South Africa. Self-collected vaginal swabs were tested for gonorrhoea, chlamydia and trichomoniasis using PCR and self-tested for trichomoniasis using a rapid dipstick test. All women were interviewed at enrolment on sociodemographic and sexual history, and at the 6-week follow-up on feasibility and acceptability.
Results: 626 women were enrolled in the study, with 313 in each group; 569 (91%) completed their 6-week follow-up visit. Forty-seven per cent of the women in the home group successfully mailed their packages, and 13% reported performing the rapid test and/or mailing the kit (partial responders), versus 42% of women in the clinic group who kept their appointment. Excluding partial responders, women in the home group were 1.3 (95% CI 1.1 to 1.5) times as likely to respond to the initiative as women in the clinic group. Among the 44% who were tested, 22% tested positive for chlamydia, 10% for trichomoniasis, and 8% for gonorrhoea.
Conclusions: Self-sampling and self-testing are feasible and acceptable options in low-income communities such as Gugulethu. As rapid diagnostic tests become available and laboratory infrastructure improves, these methodologies should be integrated into services, especially services aimed at young women.
- CT, Chlamydia trachomatis
- NG, Neisseria gonorrhoea
- OR, odds ratio
- RD, risk difference
- RR, risk rate
- STI, sexually transmitted infection
- TV, Trichomonas vaginalis
Statistics from Altmetric.com
- CT, Chlamydia trachomatis
- NG, Neisseria gonorrhoea
- OR, odds ratio
- RD, risk difference
- RR, risk rate
- STI, sexually transmitted infection
- TV, Trichomonas vaginalis
New strategies to increase coverage of sexually transmitted infection (STI) testing, diagnosis and treatment are vitally needed to combat the persistently high rates of curable STIs globally.1 This need is especially pronounced in resource-poor settings such as sub-Saharan Africa, with a high burden of disease, dependence on syndromic management for diagnosis, and low levels of health infrastructure.2
Two methodologies could help to improve women’s access to STI management by allowing testing to occur in non-clinical settings and improving diagnostic accuracy: self-sampling techniques3–7 and self-testing. As rapid diagnostics become easier to use, women can test their own self-collected specimens for infections (self-testing), similar to a home pregnancy test.8
Offering self-sampling at home may increase women’s likelihood to be screened for STIs.8,9 However, few studies have evaluated home sampling, and almost none have evaluated self-testing in resource-poor settings8 such as South Africa, where STI prevalence is high.10 We therefore conducted a study in Gugulethu, South Africa comparing response rate among young women randomised to home-based versus clinic-based screening, as well as feasibility and acceptability of self-sampling and self-testing. We implemented a similar study concurrently in São Paulo, Brazil with a wider age range of women.8 In both studies, we hypothesised that more women would respond to home-based than clinic-based screening. In this paper, we present results from South Africa.
METHODS
Women were enrolled from September 2003 to March 2004 and followed through August 2004 at the Empilisweni Wellness Center, a clinical trial research site in Gugulethu. Women received a home self-sampling and self-testing kit or a clinic appointment to be screened for Neisseria gonorrhoea (NG), Chlamydia trachomatis (CT) and Trichomonas vaginalis (TV).
Study procedures
General information sessions on STIs and a study description were held at four community-based youth groups and two public health clinics (Uluntu and Nyanga). Eligible women were 14–25 years old, had at least a grade 5 education to ensure literacy, and did not report genital ulcers or other symptoms in need of immediate gynaecological care. Participants provided informed consent and were interviewed about sociodemographic characteristics and sexual history using Xhosa and English structured questionnaires. Women were randomised to the home or clinic group using a random sequence prepared before study initiation. Staff opened a sealed randomisation envelope for the next sequential identification number containing group assignment. Blinding was impossible after assignment, as women either received a home kit or clinic appointment; participant materials were labelled by group to facilitate procedures. All women had a clinic appointment 6 weeks after enrolment for clinical follow-up and interview. Up to three attempts were made to contact women who missed this visit.
The home kit consisted of a paper bag containing: two vaginal swabs in sealed plastic tubes; a XenoStrip TV test (a rapid TV dipstick test; Xenotope Diagnostics, San Antonio, Texas, USA) with a small container of buffer solution; instructions on how to use the kit with diagrams and a toll-free phone number; two self-administered questionnaires; an addressed envelope with pre-paid postage for mailing used materials and questionnaires; condoms, a pen, and educational materials on STIs and other reproductive health services.
Women in the clinic group received an identical looking paper bag, containing condoms and educational materials, and a clinic appointment card. At their appointment, women were given two swabs for self-sampling and the rapid TV test for self-testing. In this group, nurses observed self-sampling and self-testing and recorded any difficulties the participant displayed.
Specimen collection and laboratory procedures
The first self-collected specimen (Dacron swab) was forwarded to the University of Cape Town Virology Laboratory for PCR testing using Roche COBAS AMPLICOR PCR tests (Roche Molecular Diagnostics, Pleasanton, California, USA) to detect NG and CT, and in-house PCR to detect TV.3 The woman used a second swab (cotton) to perform the rapid TV test.8
Home kits were collected from the post office daily; staff recorded the content before delivering swabs to the laboratory. Similarly, swabs collected at the clinic were stored dry at room temperature and delivered to the laboratory daily.
Treatment
Women who tested positive by rapid test at the clinic were treated that day. Women in the home group with a positive rapid TV test were asked to call the toll-free number and come to the clinic for treatment. All women were asked to call the toll-free number for their PCR results 2 weeks after specimen collection. Women with positive results who had not previously been treated were contacted or treated at their follow-up visit, if attempts to contact them were unsuccessful, and chose between different partner notification methods as described elsewhere.11 The study was approved by ethical committees at the University of Cape Town and the Population Council.
Measures and data analysis
The main study outcome was the proportion of women who responded to the initiative, defined as mailing their kit or attending their clinic appointment. Women in the home group whose packages were not received but called to report a positive rapid TV test or reported having done the rapid TV test and/or mailing the package at the 6-week visit were coded as “partial responders”. The sample size was powered at 80% to detect a 10% difference, assuming that 20% of the women would respond in the clinic group with an α of 0.05.
Feasibility of home and clinic self-sampling for all infections and self-testing for TV was measured in both groups by questions on difficulties performing these procedures and by clinician observation in the clinic group. Acceptability was measured immediately after study procedures with self-administered questionnaires and by interviewer at the follow-up visit using preferences for future STI screening.
To test for a difference in response rates, sociodemographic characteristics, sexual history, feasibility and acceptability responses between the groups, we used the Fisher exact test for categorical variables and the Mann-Whitney rank sum test for continuous variables. To explore additional predictors for responding to the screening initiative, we used multivariable logistic regression.
RESULTS
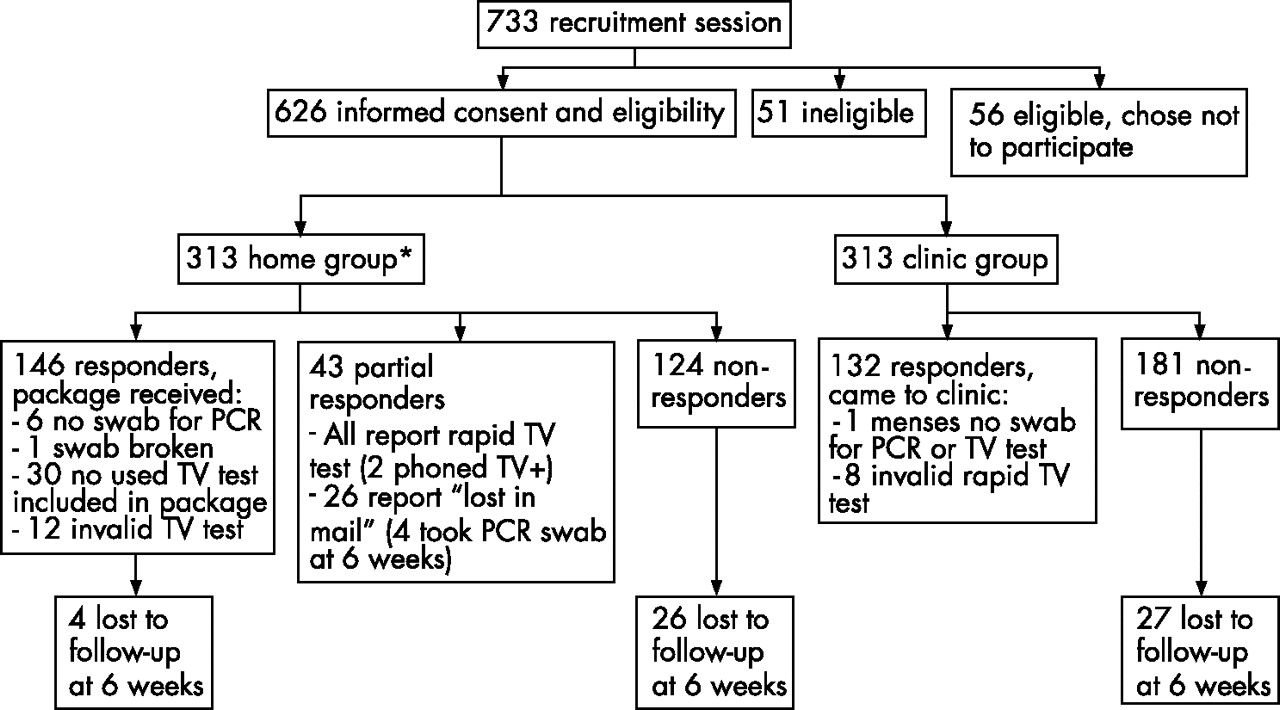
Of 733 women recruited, 626 (85%) were eligible and chose to participate (fig 1). Most participants were recruited from the nearby Uluntu clinic (49%), followed by the Nyanga clinic (36%), and non-clinic youth groups (14%). Ninety-one per cent completed their 6-week follow-up visit, with 9% lost to follow-up. Loss to follow-up was highest among women recruited at the Nyanga clinic (16%), followed by the Uluntu clinic (6%), and the non-clinic youth groups (2%, p<0.001). No differences were found between the home and clinic groups in baseline sociodemographic characteristics and sexual history (table 1).
Recruitment site, demographics and sexual history at enrolment

{kind=link}
Participant flow and response by randomisation group, Gugulethu, South Africa. *One woman (non-responder) was accidentally told that she was in the clinic group; counted as home group per randomisation scheme.
Screening initiative response
Forty-two per cent of women in the clinic group came for their appointment compared with 47% of the home group’s mailed packages received, with an additional 14% of the home group reporting partial responses (fig 1). Excluding partial responders, women in the home group were 30% more likely to respond than women in the clinic group (risk rate (RR) = 1.3, 95% CI 1.1 to 1.5; risk difference (RD) = 11.9% 95% CI 3.8% to 20.0%). There was no difference between the response rates of the two groups (RR = 1.1, 95% CI 0.9 to 1.3; RD = 4.5%, 95% CI −3.3% to 12.2%), counting partial responders as non-responders. However, assuming that they were responders, the response rate was significantly higher in the home group (60%) than the clinic group (42%; RR = 1.4, 95% CI 1.2 to 1.7; RD = 18.2%, 95% CI 10.5% to 25.9%).
Among women who responded to the initiative, almost all were tested for NG, CT and TV by PCR in both groups (fig 1). Six women in the home group did not include their self-collected swab in the kit; one sent a broken swab which was not forwarded to the laboratory; four reported that the kit was lost in the mail and self-collected the swab during the 6-week visit; and two did not mail their kit but called with a positive rapid TV test. One woman in the clinic group had her menses so was unable to self-collect a swab. A total of 274 (44%) were tested by PCR: 143 (46%) in the home group and 131 (41%) in the clinic group. Overall, 22% tested positive for CT, 10% for TV, and 8% for NG. Women in the clinic group were more likely to test positive for CT than those in the home group (27% vs 15%, p = 0.02). However, there were no differences in prevalence for NG (8% in both) and TV (11% clinic; 9% home, p = 0.69). All women who tested positive were treated in both groups.
Excluding partial responders, women in the home group had 1.7 (95% CI 1.2 to 2.5) times the odds of responding to the initiative as clinic women, when age, education, recruitment site, number of sex partners in last 6 months, and reported STI history were controlled for (table 2). Older women were slightly more likely to respond than younger women, as were women who had ever attended university. Within the clinic group, other variables associated with responding were reporting ever having had sex (odds ratio (OR) = 2.9, 95%CI 1.1 to 7.4), reporting unusual vaginal discharge at enrolment (OR = 2.3, 95% CI 1.1 to 4.8), and ever having had an STI symptom but not seeking care (OR = 2.7, 95% CI 1.3 to 5.3). Within the home group, number of lifetime sex partners was also significantly associated with responding (OR = 1.2, 95% CI 1.0 to 1.4). Ever having used a tampon or home pregnancy test and symptoms at enrolment were not associated with responding in the home group.
Factors associated with responding to the screening initiative, excluding partial responders
Feasibility
Of the 168 women who reported mailing their kits at the 6-week visit, 146 (87%) were received at the clinic. Almost all (96%) contained the self-collected swab for PCR testing, 79% contained the used TV test strip, and 77% the self-administered questionnaire. Although most women reported that self-sampling was easy or very easy, more women in the clinic group reported this than women in the home group (table 3).
Feasibility and acceptability of self-sampling and self-testing by group
At the 6-week interview, 65% of women in the home group reported having used the rapid TV test on their own. Ninety-five per cent of these women reported being able to read the results, and 92% of the recorded results matched the reading by clinic staff (table 3). Almost all clinic women (98%) who came for their appointment were rated as finding it easy or very easy to perform the rapid test on their own. Twenty-six per cent of women in the home group reported using the toll-free phone number, compared with 14% in the clinic group (p = 0.001). The main reason why women in the home group called was to obtain their PCR results (49%).
Acceptability
Almost all (97%) women at the 6-week interview who successfully self-sampled reported that they would self-sample in the future (table 3). In choosing between self-sampling at home and the clinic, women in the home group reported preferring the home (58%), whereas women in the clinic group reported preferring the clinic (66%). The main reasons for preferring home were privacy (42%) and ease (39%); the main reasons for preferring the clinic were being worried about making mistakes (46%), wanting supervision (25%), and not having privacy at home (21%). When choosing a location for self-testing, the majority (60%) in the home group would prefer to self-test at home, whereas most (71%) women in the clinic group would prefer the clinic. The main advantages for self-testing at home were privacy (60%) and confidentiality (36%), whereas the main advantages for self-testing at the clinic were availability of nurses to help (53%), and receiving immediate treatment (45%). Eighty-five per cent of women in both groups would purchase self-sampling and self-testing kits at the pharmacy were they available. Participants would be willing to pay a median of 16 Rand (approximately US$2.30).
DISCUSSION
Introducing home-based STI screening in this low-income setting in Gugulethu, South Africa resulted in a moderately higher proportion of women screened compared with clinic-based screening (unadjusted RR 1.3). A similar study conducted in São Paulo, Brazil also found a slightly higher response rate for home-based than clinic-based STI screening within 2 weeks of enrolment (80% vs 76%).8 Both studies showed a modest effect, suggesting that home-based screening is, at a minimum, as acceptable as clinic-based screening for women in resource-poor settings, and may result in more women being screened. The moderate difference found in both studies may be due to the high proportion of respondents recruited from clinics, who are probably women predisposed to clinic attendance.
The response rate was higher than expected in both groups, with 42% of the clinic group responding compared with our hypothesised response rate of 20%. Although this finding is encouraging, still less than half (44%) of the women overall were screened for STIs in this high-prevalence setting. The response rate was much higher in the Brazil study.8 In addition to potential sociocultural differences, the studies targeted different age groups: the Brazil study included women aged 18–40, whereas this study focused on young women 14–25 years old. Young women may have greater barriers to receiving STI screening than older women, as is seen in the present study, with women aged 23–25 nearly three times as likely to respond as women aged 14–17, after adjustment for randomisation group.
Self-testing and self-sampling were feasible in both clinic and home settings. However, women at home had more difficulties than women in the clinic in terms of performing the rapid test, especially reading the test results. As rapid diagnostics continue to be developed, instructions should be carefully pre-tested and designs refined for ease of interpretation of results. Women did not report difficulties using the mail and the toll-free number, suggesting that this type of screening initiative is possible in resource-poor settings.
This study had limitations. Women preferred the setting in which they had experience; having women try both environments and discuss preferences may be more informative. The choice of interpretation of “partial responders” alters study findings. Nevertheless, the proportion of women who were successfully tested for CT, NG and TV by PCR was equivalent in the two groups, and all women who tested positive were treated in both groups. Data on the number of attempts needed to track positive cases, however, were not systematically recorded; nor were data on the number of women who called with positive rapid TV tests.
Key messages
-
Self-sampling and self-testing for diagnosis of sexually transmitted infections (STIs) are feasible and acceptable options for many women in low-income communities.
-
Home-based STI screening is as acceptable as, if not slightly more acceptable than, clinic-based screening to young women. However, self-sampling and self-testing at home may be more prone to user error than at the clinic.
-
Many resource-limited settings do not currently have STI screening programmes, relying on syndromic management of people with symptoms who seek care at clinics, while asymptomatic infections go undiagnosed and untreated. As in-house PCR capability increases and rapid diagnostics improve, self-sampling and self-testing should be used to provide STI screening services in a wide range of clinical and non-clinical venues to maximise programme coverage for management of symptomatic and asymptomatic cases.
Finally, the findings have limited policy implications at present in that the cost of commercial PCR diagnostics for CT and NG remains prohibitively high. However, in countries such as South Africa and Brazil, where infrastructure for laboratory technology is growing, the potential for using cheaper in-house PCR techniques with self-acquired samples is becoming a viable reality. In addition, women themselves report being willing to pay a nominal fee (US$2.30), suggesting potential for introducing subsidised home kits into services.
Creative screening programmes for STIs are needed in resource-poor settings with a heavy disease burden. South Africa does not currently have screening programmes, relying on syndromic management for people with symptoms who seek care at clinics, while asymptomatic infections go undiagnosed and untreated. We have shown that self-sampling and self-testing are feasible and acceptable options in low-income communities such as Gugulethu. As rapid diagnostic tests and laboratory infrastructure improve, these technologies should be used to introduce STI screening services into a wide range of clinical and non-clinical venues to maximise programme coverage.
Acknowledgments
We thank the following: the study participants and staff at the Empilisweni Centre for Wellness Studies in Gugulethu; Willi McFarland and staff at the University of San Francisco Center for AIDS Prevention Studies (CAPS) and Nicol Coetzee for input in the protocol and study design; Susie Hoffman, Luisa Borrell, Katherine Keyes, Bianca Malcolm, Nina Banerjee and Sheri Lippman for their review of previous versions of the manuscript; Taja Ferguson, Barbara Friedland, Sarah Braunstein, Beverly Winikoff and Elof Johansson from the Population Council for their input in administration and general support; and Xenotope Diagnostics for provision of rapid diagnostics at reduced cost.
REFERENCES
Footnotes
-
Contributors
HEJ implemented data analysis, wrote the manuscript, and assisted with protocol and questionnaire design; LA wrote the initial protocol, assisted with questionnaire development, and provided editorial comments; AdeK and TY developed initial questionnaires, oversaw study implementation, and provided editorial comments; JHHMvandeW assisted with study and questionnaire development, data analysis, and provided editorial comments.
-
This study was funded by the Office of Population and Reproductive Health, Bureau for Global Health, US Agency for International Development, under the terms of Award No HRN-A-00-99-00010. The opinions expressed herein are those of the authors and do not necessarily reflect the views of the US Agency for International Development. Additional funding was received from the Parthenon Trust and the William and Flora Hewlett Foundation.
-
Competing interests: None.
Linked Articles
- Brief Encounters