Article Text

Abstract
Objectives: Chlamydia is the most common bacterial sexually transmitted infection worldwide and a major cause of morbidity—particularly among women and neonates. We compared costs and health consequences of using point-of-care (POC) tests with current syndromic management among antenatal care attendees in sub-Saharan Africa. We also compared erythromycin with azithromycin treatment and universal with age-based chlamydia management.
Methods: A decision analytical model was developed to compare diagnostic and treatment strategies, using Botswana as a case. Model input was based upon (1) a study of pregnant women in Botswana, (2) literature reviews and (3) expert opinion. We expressed the study outcome in terms of costs (US$), cases cured, magnitude of overtreatment and successful partner treatment.
Results: Azithromycin was less costly and more effective than erythromycin. Compared with syndromic management, testing all attendees on their first visit with a 75% sensitive POC test increased the number of cases cured from 1500 to 3500 in a population of 100 000 women, at a cost of US$38 per additional case cured. This cost was lower in high-prevalence populations or if testing was restricted to teenagers. The specific POC tests provided the advantage of substantial reductions in overtreatment with antibiotics and improved partner management.
Conclusions: Using POC tests to diagnose chlamydia during antenatal care in sub-Saharan Africa entails greater health benefits than syndromic management does—and at acceptable costs—especially when restricted to younger women. Changes in diagnostic strategy and treatment regimens may improve people’s health and even reduce healthcare budgets.
- POC, point-of-care
- SA, syndromic approach
Statistics from Altmetric.com
Chlamydia trachomatis infection is the most common bacterial sexually transmitted infection (STI) worldwide, with highest prevalences in sub-Saharan Africa.1 In women, chlamydia can progress to pelvic inflammatory disease, and subsequently cause ectopic pregnancy and infertility. The risk of intrauterine growth retardation, preterm birth, perinatal conjunctivitis and pneumonia, and postpartum upper genital tract infections makes treatment in pregnancy desirable.2,3 Because STIs can enhance HIV transmission, UNAIDS and WHO recommend the improvement of STI control.4,5
In developing countries, the diagnosis of chlamydia has been limited to the syndromic approach, a strategy that is neither sensitive nor specific.3,6–8 The majority of infected women are asymptomatic and will not be diagnosed and treated, and high levels of overtreatment increase drug costs and the risk of drug resistance.8 Simple, affordable point-of-care (POC) tests are needed to improve chlamydia management in the developing world.9 Tests with moderate sensitivity and high specificity are commercially available, and more sensitive tests are under development.7,9,10
The aim of this economic evaluation was to estimate, from the healthcare perspective, incremental costs and health consequences in sub-Saharan Africa of testing all antenatal care attendees with a POC test on their first visit. Treating the women with azithromycin was compared with erythromycin treatment; and, as chlamydia is strongly correlated with youth,11,12 we also compared the management of teenagers or women under 30 years of age to universal management. Our case was Botswana, a country with 7.5% prevalence of chlamydia and 32% HIV prevalence among antenatal care attendees.13,14 Screening for syphilis and HIV in pregnancy is routine, and all clinics and health posts perform POC tests for HIV, suggesting that it would be feasible to use POC tests for chlamydia in this setting.
METHODS
Decision analytical model
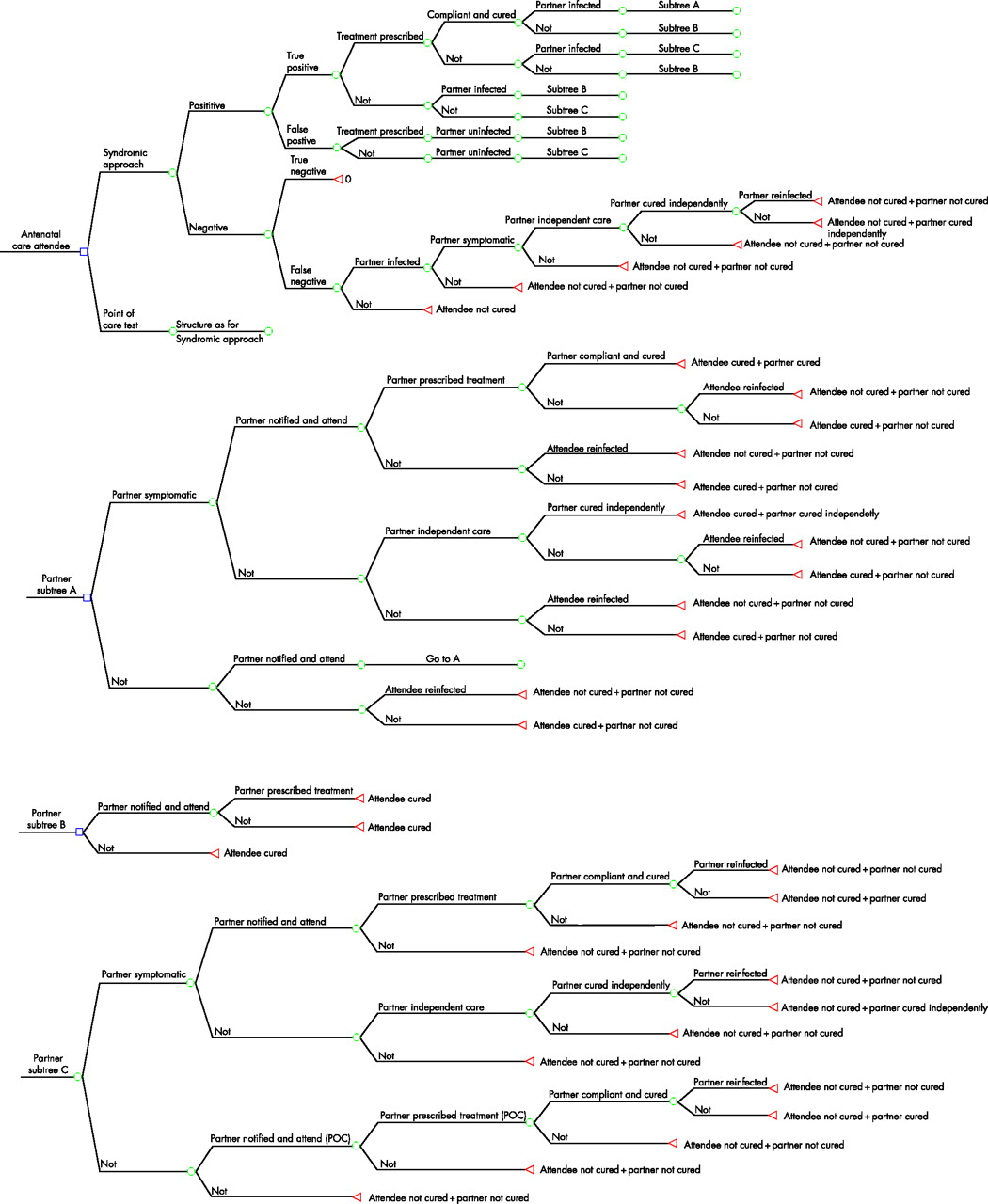
We used TreeAge Pro software to develop a decision analytical model, comparing the use of POC tests with syndromic management in a hypothetical cohort of 100 000 antenatal care attendees (fig 1). The structure of the decision tree branches is identical for the two diagnostic strategies, but the probabilities of events differ. We assigned costs to each branch, using the number of cured infections as the measure of benefit. The model captures programme costs, the number of cured infections and reinfections among attendees and their partners, and the number and cost of patients unnecessarily treated with antibiotics.
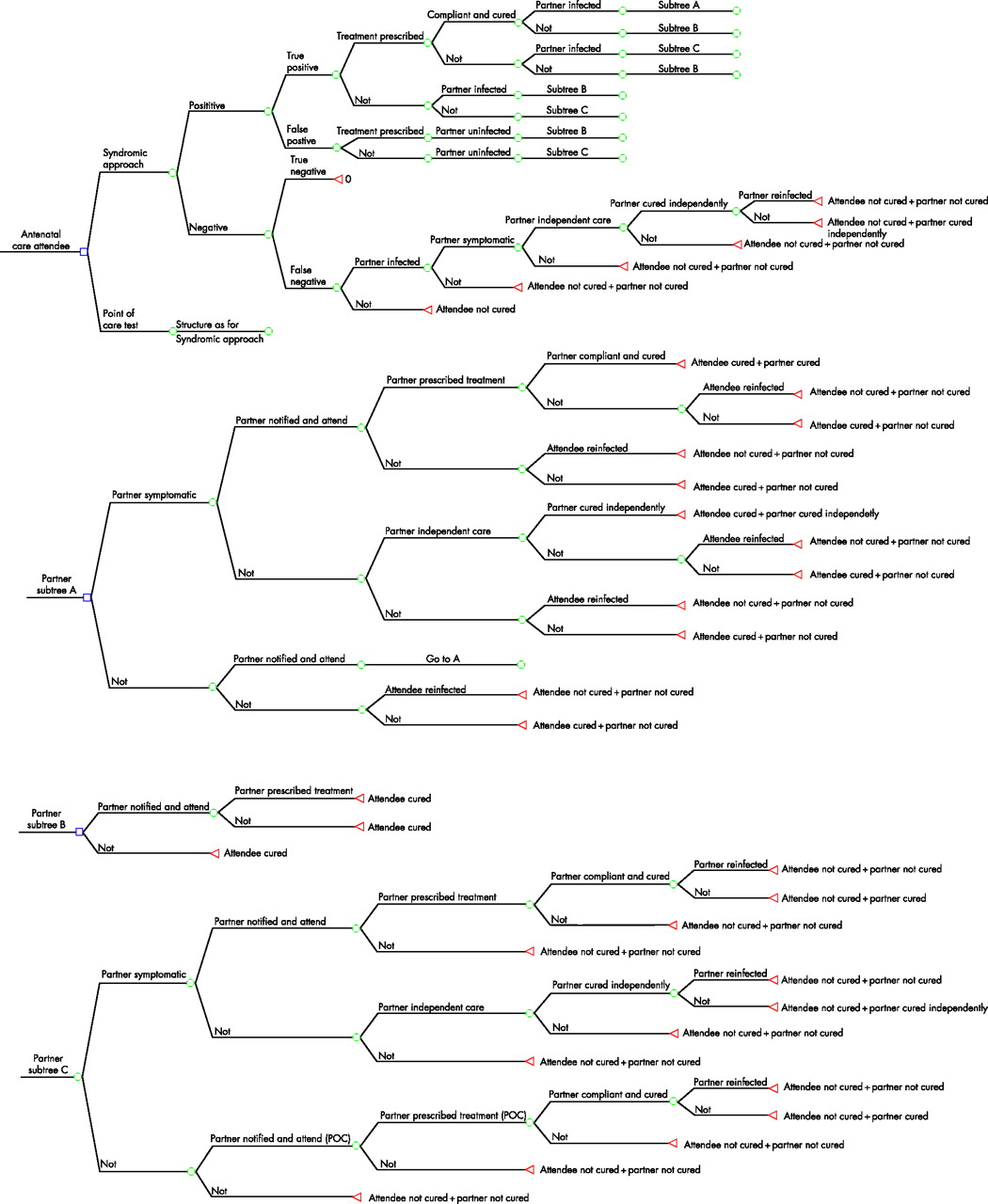
Key structure of the decision tree and its branches.
Information to feed the decision tree was based on literature reviews and Medline searches for data on all probabilities and costs, a cross-sectional study among 703 antenatal care attendees in Gaborone, the capital of Botswana,12,14 and advice from an expert panel. The model probabilities are presented in table 1. The model is described in full in a technical report, available online.15
Model probabilities
Probabilities
The general and age-specific prevalences of chlamydia were based on the Gaborone study.14,15 These prevalences correspond with those among pregnant women in other sub-Saharan countries, but prevalences from 3% to 31% have been found.3,8 Prevalences may differ in other settings or change over time, and to estimate the effect of prevalence on the results, this range was used in the one-way sensitivity analysis. The chlamydia transmission rate was based on co-infection studies among STI patients and on expert opinion.15, w1–w4 For the w-references, please see the additional web reference list.
The sensitivity and specificity of the syndromic approach in the diagnosis of chlamydia in pregnancy were based on the Gaborone study—figures similar to those of other studies from sub-Saharan Africa.3,15,16 A pregnant woman diagnosed as having vaginal discharge syndrome may have normal pregnancy-related discharge or symptoms caused by candida, bacterial vaginosis or trichomoniasis—or, less likely, chlamydia or gonorrhoea. This uncertainty, coupled with the fact that the syndrome requires up to four drug regimens, reduces nurses’ adherence to treatment guidelines, patient compliance, and incentives to ensure partner notification.8 With syndromic management, these variables were based on expert knowledge of the situation in developing countries, indirect study data and available evidence (table 1).
The sensitivity of available POC tests have shown considerable variability (25–85%).w5 A recent evaluation of a widely used test found 50% sensitivity,11 and more sensitive tests are under development.17 We evaluated 50–85% sensitive tests, and exemplify with 50% and 75% sensitive tests in the text. All POC tests for chlamydia have high specificity.9,10 A positive test requires prescription of and compliance with one drug regimen. Data on the management with POC tests are lacking. The expert panel inflated the values used for the probabilities in the syndromic strategy, assuming that the additional confidence in the POC test result would improve management (table 1). The possibility that this is not the case is covered by using large uncertainty bounds, including in the lower bound a value that represents syndromic management. The upper bound represents much better performance, as found in developed countries where specific chlamydia tests are in use.
Costs
The costs were modelled from the providers’ perspective and presented in 2006 US$ (table 2). For syndromic management, we included direct drug costs and the cost of a pharmacy technician dispensing and informing patients. In the base-case analysis, we used government wage rates from Botswana;w6, w7 a range of ±50% was evaluated in the sensitivity analyses to ensure relevance to countries with different personnel costs and to cover uncertainty over testing and dispensing time. Drug costs were collected from the Technical Support Services, Botswana Ministry of Health and the International Drug Price Indicator Guide.w8, w9
Model costs (2006 US$)
For the POC-test strategy, we added test costs and the cost of time required to conduct each test. Currently available POC tests cost between $0.85 and $7.00.7,18 We modelled test costs at between $0.50 and $4.00, as less expensive tests are likely to be available in the near future. Costs of staff training were not included: Syndromic management requires frequent training and supervision of health personnel, and introducing POC tests for chlamydia should fit well into the ongoing activities of the national STI programmes. Discounting was not performed, as the time perspective was less than one year.
Sensitivity analyses
To test the robustness of model results, we undertook a range of sensitivity analyses. We first explored the consequences of parameter uncertainties in one-way sensitivity analyses, where one parameter at a time was varied up and down within the prespecified uncertainty bounds, while maintaining the others at their base-case values (tables 1 and 2). In these analyses, testing all new antenatal care attendees with a 50–85% POC test was compared with syndromic management in the same population using azithromycin as treatment.
We also performed probabilistic sensitivity analyses in which the model was run 10 000 times, allowing the effects of joint uncertainty across all the parameters of the model to be considered. Universal testing, first with a 50% sensitive and then with a 75% sensitive POC test, was compared with syndromic management in a population with 7.5% chlamydia prevalence, using azithromycin as the drug of choice. We adopted beta distributions for the probabilities to constrain the values between 0 and 1, and gamma distributions for the costs because of their skewness. The probabilities in the two strategies were linked to account for interdependencies.
RESULTS
Health outcome and costs
Choice of antibiotics
In an antenatal care population of 100 000 attendees with a 7.5% chlamydia prevalence, syndromic management and treatment with erythromycin would entail a total cost of $54 400 and result in 800 cases of chlamydia cured ($66 per cured case) (table 3). Replacing erythromycin with azithromycin would entail a total cost of $31 400 and result in 1500 cases cured ($21 per cured case). In all scenarios, single-dose treatment with azithromycin implied a lower cost and greater effectiveness than did treatment with erythromycin (table 3). Therefore, in the next sections, we compare POC testing with the syndromic approach and universal versus age-based selective management using only the azithromycin treatment.
Testing all women with point-of-care (POC) tests compared with syndromic approach (SA)—according to treatment regimen, universal- or age-based management and test sensitivity: expected and incremental costs and effects per 1000 attendees included in the programme, and total programme costs and effects in a population of 100 000 antenatal care attendees*
POC tests versus the syndromic approach
Testing all attendees with a 50% sensitive POC test priced at $0.85 would cost $106 800 and result in 2400 C trachomatis infections cured per 100 000 women ($87 per additional case cured) (table 3). With increasing test sensitivity, the number of cases cured would increase further, while the cost of the programme would remain virtually unchanged, reducing the incremental cost per cured case.
Universal or selective management
Restricting syndromic management or testing for chlamydia to teenage attendees would entail the lowest cost per case cured: $10 with the syndromic approach, $22 with a 50% sensitive POC test, and $15 with a 75% sensitive POC test (table 3). Selective compared with universal syndromic management implies lower programme costs but results in fewer infections cured—as fewer women are included—and the same applies to the use of POC tests (table 3). Reserving chlamydia treatment to teenagers would reduce the programme costs of syndromic management by 80%, but also reduce the number of cases cured by about 60%. Using a 75% sensitive POC test among teenagers, however, would be as effective as the syndromic management of chlamydia among all attendees, and the programme cost would be reduced from $31 400 to $22 400 (table 3).
Overtreatment and partner management
In a population of 100 000 pregnant women, syndromic management and azithromycin treatment would result in 1500 cured cases, although 29 900 individuals would be treated unnecessarily (table 4). The treatment costs would be $31 400, 90% of which represents treatment of uninfected individuals. Introducing the testing of all attendees with a 50% or 75% sensitive POC test would result in 2400 or 3500 cured infections and 1800 or 1900 individuals unnecessarily treated. Furthermore, drug costs wasted on uninfected individuals would be reduced by 95%. Selectively testing attendees less than 20 years of age with a 50% or 75% sensitive test would imply 1000 or 1500 cases of chlamydia cured and 300 individuals unnecessarily treated, reducing drug wastage to 1% of the current level.
Number of female and male cases cured, number of patients overtreated, total costs, drug costs* and costs of drug wastage†: testing all women with a 50% or 75% sensitive point-of-care (POC) test compared with syndromic approach in a population of 100 000 antenatal care attendees‡
With syndromic management, 140 of the estimated 6000 infected partners would be successfully treated (table 5). Using a 50% or 75% POC test would increase this number to 600 or 900, which also would reduce reinfection rates. The majority of attendees diagnosed as having syndromic approach are uninfected, and increasing partner attendance from the current 8.5% to 50% would result in 1200 more cases cured per 100 000 attendees—while 11 700 additional uninfected partners would be unnecessarily treated. Increasing partner attendance to 50% when using 50% or 75% sensitive POC tests would result in 1300 or 2100 more cases cured, while 700 or 900 additional partners would be treated unnecessarily.
Expected number of antenatal care attendees and their partners diagnosed, treated* and cured: testing all women with a 50% or 75% sensitive point-of-care test compared with syndromic approach in a population of 100 000 antenatal care attendees†
Model uncertainty
In the one-way sensitivity analyses, the cost of the POC test had its greatest impact on the incremental cost per case cured of introducing POC tests (fig 2). High chlamydia prevalences result in the lowest incremental cost per additional case cured; decreasing from $91.80 in populations with 3% prevalence to $11.00 in populations with 31% prevalence (table 6). The probability of a partner being notified and attending healthcare with the POC-test strategy was also an importanat factor; the incremental cost per additional case cured ranged from $69.90 with poor attendance to $18.10 with optimal performance. For the remaining model parameters, realistic changes in values made little difference to the results.
Sensitivity analysis: cost per additional case cured with a POC test compared with syndromic approach under different assumptions about model parameters*
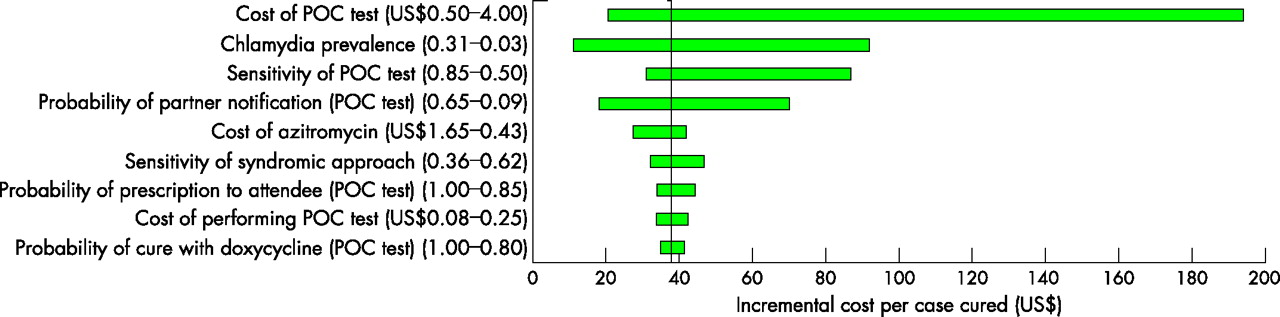
Tornado diagram summarising one-way sensitivity analyses in which testing all women with a POC test is compared with syndromic management of chlamydia among 100 000 antenatal care attendees.
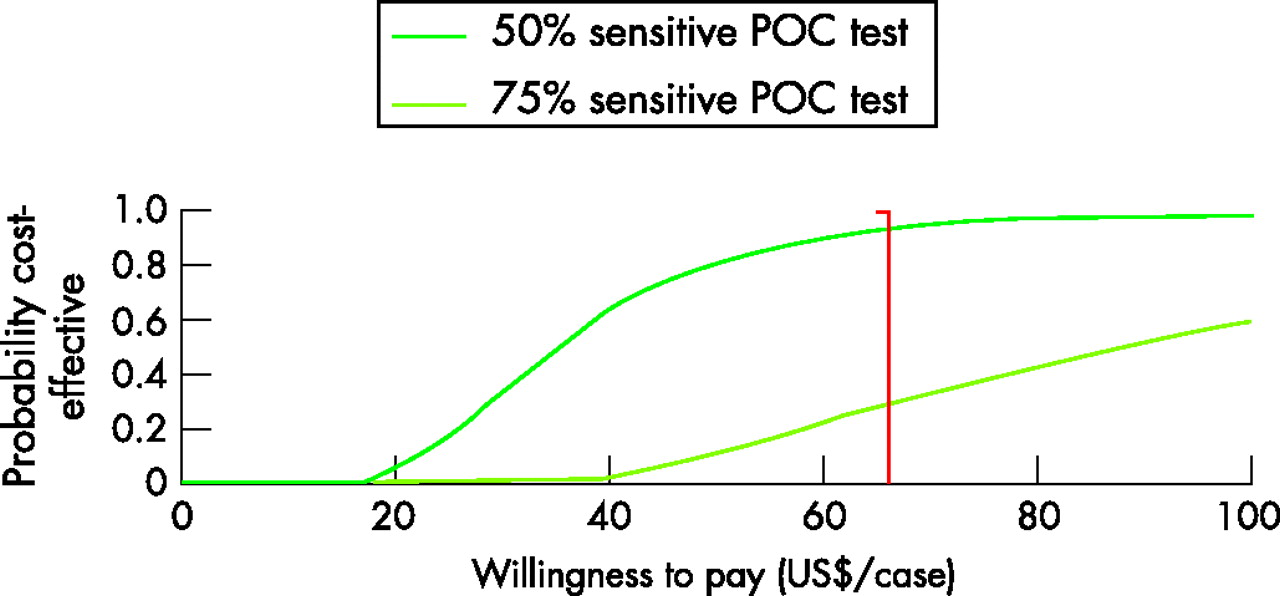
As for the probabilistic sensitivity analyses, using POC tests was more effective and more costly than was the syndromic approach in practically all model iterations. The incremental number of infections cured with a 50% or 75% sensitive POC tests varied from −250 to 4100 or from 500 to 7200 per 100 000 women screened. The additional cost ranged from $58 700 to $94 700 or from $60 800 to $96 200. In Botswana, health authorities currently pay about $66 per cured infection with C trachomatis. Adopting this willingness-to-pay threshold, replacing syndromic management with POC tests of all attendees had a 29% probability of being cost-effective with a 50% sensitive test and 94% with a 75% sensitive test (fig 3).
{kind=link}
{kind=link}
{kind=link}
Cost-effectiveness acceptability curves for testing all women with a POC test compared with syndromic management. The vertical line represents the current willingness to pay in Botswana (US$66).
DISCUSSION
The results of this study indicate that there may be substantial benefits in changing current diagnostic and treatment strategies for chlamydia in antenatal care in sub-Saharan Africa. The prevailing syndromic management of all attendees appears to be the least effective; it incurs high costs per case cured and entails considerable overtreatment.
The study is limited by uncertainties in several of the model parameters. There is a paucity of high-quality studies providing data relevant for sub-Saharan Africa, and many probabilities are based partly on expert advice. For the POC-test strategy, the level of correct prescription, patient compliance and partner notification have a high degree of uncertainty, and were provided with broad uncertainty ranges. The sensitivity analyses show that partner notification with POC tests is important for the effectiveness of the strategy, also indicating the potential impact of strategies to improve partner notification. The cost of the POC test, which was the largest source of variation in the results, will be known by authorities who consider implementating a POC-test strategy.
Large evidence gaps and conflicting evidence exist regarding chlamydia-related complications and their economic consequences.19,20 Because of this lack of knowledge, especially for developing countries, cured infections was used as the effect measure; thus important health benefits of case detection and treatment are not captured in this analysis. Short-term outcomes are not ideal for making policy recommendations, but as the existing management requires substantial resources, information about possibilities for more advantageous resource allocation should be highly relevant to health policy makers. If successful chlamydia treatment reduces complications such as neonatal infections and postpartum infections, or reduces HIV transmission,4,5 it would strengthen the conclusions of this study.21
To our knowledge, no studies in resource-poor settings have explored the costs and health consequences of chlamydia management strategies in pregnancy. One study has estimated the incremental cost-effectiveness of using POC tests for chlamydia and gonorrhoea among sex workers in Benin. Compared with syndromic management, such tests were cost-effective, averting HIV infections and decreasing inappropriate treatment.18 Reviews of economic evaluations, mainly from developed countries, indicate that chlamydia screening is cost-effective, depending on prevalence; azithromycin is cost-effective; and partner notification is essential.21,22 The studies showed considerable variability with regard to probabilities used, complications and costing considered, and were hampered by methodological problems. The reviews point out the need for more data, particularly on the risk of complications.
We used a static model to evaluate the chlamydia management of antenatal care attendees, a relatively small, non-core group within the total population. Static models assume constant infection prevalence, even when strategies result in fewer or more infections being cured. In contrast, dynamic models incorporate the impact of changes in strategy on infection prevalence. In recent years, the use of dynamic models has been advocated.22,23 However, chlamydia programmes targeting pregnant women are less likely to lower prevalence, and have been specifically mentioned as an example in which static models may be the preferred option.23
Botswana was used as the case for this analysis, but the model should be applicable to other sub-Saharan countries. In the majority of countries in the region, 70% or more of pregnant women attend antenatal care at least once,24 providing a convenient framework for diagnosis, treatment and follow-up. Botswana is classified as “upper-middle income”, but the cost estimates will nevertheless be applicable to less wealthy settings with lower labour costs. The cost drivers in the model are POC tests and drugs purchased in international markets, and these prices will be relatively similar across countries. The sensitivity analysis indicates how higher or lower parameter values would change the results. To the extent that model data differ from those of other countries, the analysis can be revised on the basis of local data.
Improving maternal and perinatal conditions and combatting HIV/AIDS received substantial attention in the Millennium Declaration.25 It has been said that if countries are to have any chance of achieving their development goals, they need to re-evaluate existing strategies and replace less effective strategies with more effective ones.26 Treatment of STIs is a strategy area that has already been prioritised in sub-Saharan Africa.27 Chlamydia management in pregnancy is well within the scope of the development goals, and this study points to changes in diagnosis and treatment which may contribute to achieving these goals.
First, single-dose treatment with azithromycin should be preferred, providing lower costs and higher efficacy than does the week-long erythromycin regimen. Azithromycin is safe in pregnancy, with fewer side effects and less interaction with other drugs.28 Second, POC tests are necessary to improve effectiveness and reduce excessive overtreatment with the current management. In Botswana, the direct cost of introducing POC tests in antenatal care would increase the total health expenditure by 0.006%, an investment which may be more than offset by the reduced cost of the medical consequences of infection. Third, targeted partner notification is a good argument for introducing specific POC tests. Managing sexual partners of STI patients is essential to prevent reinfection, cure partners, break the chain of transmission and prevent complications;8 in studies from Africa, partner notification has been associated with potential harm, including domestic violence, and using an unspecific syndrome diagnosis as a basis for notifying partners is questionable.8,29 If POC tests are introduced, however, patient-delivered medication or information for partners should be considered.30 Finally, the use of POC tests entails lowest incremental cost per case cured in populations with high prevalence. Adoption of age-restricted chlamydia treatment will entail lower programme costs and be more cost-effective than would the management of all pregnant women. Testing pregnant teenagers may be a feasible and reasonable way of introducing POC tests for chlamydia to antenatal care programmes in sub-Saharan Africa.
Key messages
-
The use of single-dose azithromycin for the treatment of chlamydia in pregnancy was more effective and less costly than is the use of erythromycin.
-
Moderately sensitive but highly specific POC tests may substantially improve case detection and treatment, and dramatically reduce the massive overtreatment that exists with syndromic approach.
-
The use of POC tests will entail lowest incremental cost per case cured in high-prevalence settings, and their effectiveness will increase with optimal partner notification.
-
Testing all teenagers with a 75% sensitive POC test was equally effective and less costly than the current syndromic management strategy was.
CONCLUSION
The results of this study indicate that sub-Saharan countries can substantially improve the management of chlamydia in antenatal care. Changes in diagnostic and treatment strategies may improve maternal and infant health as well as resource use.
Acknowledgments
The authors thank the Health Research Unit, Ministry of Health, for their valuable contributions to the formal and organisational aspects of the study. We also want to thank the staff at the government Clinics and at The National Health Laboratory for their cooperation, Mafizur Rahman for his contributions during the fieldwork, Elise Klouman for thoughtful input and Torbjørn Fosen Wisløff for technical assistance.
CONTRIBUTIONS
MR and ISK designed the decision analytical model. Data collection was undertaken by MR, FH and TWS; the epidemiological study in Gaborone was planned and conducted by MR, MV, JS and PH. Data were analysed by MR, and interpreted by MR and ISK. The manuscript was written by M Romoren, and all authors have proved the final version.
REFERENCES
Footnotes
-
Funding: The study in Botswana was funded by The Health Sector Agreement between Norway and Botswana. M R was funded by a grant from the Norwegian Research Council. The funding sources were not involved in the study.
-
Competing interests: None.
Linked Articles
- Brief Encounters