Article Text

Abstract
Objectives: (i) To assess the psychosocial burden of testing for human papillomavirus (HPV) related genital disease or of a HPV-related diagnosis; (ii) to compare an instrument specifically designed to measure HPV-related psychosocial burden with other generic quality of life (QoL) instruments.
Methods: A cross-sectional design. Researchers recruited women from outpatient clinics at a major tertiary women’s hospital and a sexual health centre who completed surveys within 3 months of receiving results: 331 women, 18–45 years, who had experienced a normal cervical Papanicolaou (Pap) result, an abnormal Pap result, biopsy confirmed cervical intraepithelial neoplasia (CIN) or external genital warts (EGW). Main outcome measures: the HPV impact profile (HIP) designed to assess the psychosocial impact of HPV; two general health-related QoL surveys—the EuroQoL VAS and the Sheehan disability scale; and a HPV knowledge survey.
Results: Response rate was 78%. Significant psychosocial impacts were found for women screened for, or having a diagnosis of, HPV-related genital disease. The largest impact was in women with CIN 2/3 and EGW. This HPV-related psychosocial impact was most sensitively detected with the HIP. Relative to generic measures of QoL, the HIP provided insight into the full range of psychosocial impacts of HPV testing and diagnoses.
Conclusions: Clinicians need to be aware of the potential psychosocial impact of testing for or diagnosing HPV-related genital disease, in particular CIN 2/3 and EGW. The HIP survey is a more sensitive measure of the psychosocial impact of HPV-related genital disease than generic QoL surveys.
Statistics from Altmetric.com
A woman’s life time risk of acquiring genital human papillomavirus (HPV) infections is at least 75%.1 Approximately 40–60 HPV genotypes specifically infect the genital area.2 HPV types 16 and 18 cause 70% of cervical cancer, 55% of high-grade precancerous cervical intraepithelial neoplasia (CIN 2/3) and 35% of low grade cervical lesions (CIN 1),3 with types 6 and 11 causing approximately 85% of external genital warts (EGW)4 and 12% of CIN 1.3 5
Reduction of up to 70% for incidence and mortality from cervical cancer has been achieved in primary care due to well-organised, high-quality cervical cytology screening programmes (using Papanicolaou (Pap) smears) to detect dysplastic cellular changes, with effective recall systems, leading to appropriate treatment.6 7
Performing Pap smears and managing results is a common activity for general practice (GP) nurses and doctors.8 However, simply participating in screening programmes, when no abnormalities are detected, can cause women pain, embarrassment, fear and inconvenience.9 An abnormal Pap test can cause concerns about cancer and fertility10 in addition to general embarrassment, fear and anxiety.11 Additional procedures, such as colposcopy and cervical biopsy, also cause concern.12 Actual diagnoses of dysplasia or CIN can cause confusion, worry and depression13 and have negative effects on self-esteem, sexual dysfunction and body image.14 Recently described adverse pregnancy outcomes with some surgical treatments for CIN15 will no doubt increase concerns. EGWs can also have a negative impact on many aspects of quality of life (QoL).16
With licensure of prophylactic HPV vaccines in many countries, a quadrivalent formulation for HPV-16, 18, 6 and 11,17 18 and a bivalent one targeting HPV-16 and 18,19 it is timely to examine the psychosocial impact on women of the full spectrum of HPV-related screening activities and disease. Understanding the impact on QoL of screening programmes will be an important element in reviews of HPV vaccination and cervical cancer screening policies. To date, there has been little research in this area using specifically developed or validated tools and it is likely that existing instruments may not address the complexities of the possible psychological responses to HPV-related diagnoses.20 Therefore, we aimed to assess the psychosocial impact of HPV infection and related interventions on women, comparing HPV-specific with generic QoL instruments, prior to HPV vaccine programme implementation in young Australian women.
Methods
Subjects
The design was a cross-sectional, self-administered questionnaire study. Women were recruited in 2006 from Melbourne’s largest public teaching hospital for obstetrics and gynaecology, the Royal Women’s Hospital (RWH), and the nearby Melbourne Sexual Health Clinic (MSHC), the city’s only dedicated public sexual health service. Eligible women were aged 18–45 years with an HPV-related diagnosis, intervention or a normal Pap smear within the past 3 months. Exclusion criteria were history of HPV vaccination, concurrent enrolment in studies of HPV investigational agents, other sexually transmitted infections, history of ongoing alcohol or other drug abuse, or inability to provide informed consent.
Recruitment
Eligible women were invited to complete questionnaires in the waiting rooms and to consent to having their Pap or biopsy results confirmed either from medical records or GPs. Participants tested on the day of recruitment were mailed questionnaires 2–3 weeks later after receiving their results in the usual manner. Non-responders were followed up by telephone.
The study had four main groups:
(i) Participants with normal Pap test results
Recruited from the RWH’s family planning clinic, which caters largely for postpartum women. Eligibility criteria were normal Pap smear result in last 3 months and no abnormal Pap result or history of treatment for cervical dysplasia in the past year. Participants who later received an abnormal Pap result were re-classified accordingly for analysis.
(ii) Participants with abnormal Pap smears
Recruited from the RWH Oncology/Dysplasia Clinic. Eligibility criteria were cytological prediction of low or high grade squamous intraepithelial lesion (LSIL or HSIL) within the past 3 months with no biopsy confirmation.
(iii) Participants with biopsy-confirmed cervical dysplasia
Recruited from the RWH Oncology/Dysplasia Clinic or, for a small number, from the operating theatre waiting room prior to treatment of their recently diagnosed lesion. Eligibility criteria were a histological diagnosis of CIN 1 or CIN 2/3 within the past 3 months.
(iv) Participants with external genital warts
Recruited by treating doctors at the MSHC. Eligible women had either a new diagnosis of EGW or received treatment for EGW diagnosed within the past 3 months.
Data collection
Basic demographic data, including self-reported medical history, medical record information concerning HPV and date of diagnosis, were collected at enrolment.
Survey instruments
All surveys were completed by the women unassisted. To measure psychosocial burden and health-related QoL impact of HPV, participants completed the HPV Impact Profile (HIP). To explore the sensitivity of generic QoL surveys to the impact of HPV, participants also completed the EuroQoL Visual Analogue Scale (VAS) and the Sheehan Disability Scale (SDS).
The HIP is a validated 29-item self-administered questionnaire designed to measure the psychosocial impact of HPV-related health conditions in women. It was developed using literature reviews and interviews with women with HPV. A psychometric evaluation of the HIP (n = 583 US women) found it had favourable reliability, construct validity and good ability to discriminate disease severity.21
HIP items are scored individually and then combined into a scale or total burden score, and can be grouped to examine seven specific psychosocial domains (see online supplementary material Appendix 1).21 The response for each item is marked on a 10-point discrete analogue scale, which uses visual-spatial, numeric and verbal descriptive anchors (from “not at all” to “extremely”) to assess participants’ responses. Higher scores indicate more negative impact. Eight Australian women, aged 23–44 years, with a Pap test in the preceding 12 months, were interviewed to ensure linguistic and cultural validity of the HIP for use in Australia. Minor modifications were made for the Australian context.
The EuroQol VAS is administered as a visual thermometer. Participants select their current health status on a scale from 0 (death) to 100 (perfect health).22 The SDS is a three-item questionnaire, which measures how diminished health status interferes with work/school, family life and social activities on a 0–10 Likert scale.23 For this study, the SDS was prefaced with: “All statements refer to your recent gynaecological examination or result”.
Finally, participants completed a nine question tick-box survey to assess knowledge regarding HPV (whether aware of HPV; self-report of knowledge; how contracted and by which gender; its long term effects), cervical screening (what is a Pap test; how often should women undergo one), their understanding of their recent gynaecological examination or test result and lifestyle factors that may increase their risk of cervical cancer.24
Data analysis
Statistical analyses were performed using Stata v9.1 (StataCorp, College Station, Texas, USA). Demographic characteristics, HPV knowledge survey responses and baseline data were summarised using descriptive statistics. Age was compared between participant groups using linear regression analyses. The Pearson χ2 test was used to compare differences in proportions for categorical variables (ethnicity, current partner, general health, education and HPV knowledge).
HIP item scores were linearly transformed to a 0–100 scale, with some items reverse scored to account for the intended meaning. The individual domain scale scores were computed as the sum of the items over the number of domain items answered (that is, accounts for missing data). If more than 50% of the items in the scale are missing, the scale is not computed; however, all women in our study answered over 50% of items. To create the overall HIP score, the mean was computed as the sum of all the items over the number of items answered on all domain scales.
Overall HIP scores, HIP domain scores and EuroQoL VAS scores were compared using linear regression modelling. Results of univariate and multivariate regression analyses, adjusting for age, ethnicity and whether the participant had a current partner, are presented. Interaction terms were included in the models to test for group effect modification. No significant interactions were demonstrated and interaction terms were, therefore, omitted from the final multivariate models. In addition, multivariate regression analysis was used to test for associations between HIP score and two broad aspects of the knowledge survey: self-report of HPV knowledge and whether aware of HPV. Group effect modification was tested by inclusion of interaction terms. Model assumptions were checked by standard diagnostic plots.25 For variables where model residuals were found to be non-normal, confidence intervals (CI) were estimated using bootstrap standard errors. The responses to the SDS were combined to produce either: (i) a dichotomous outcome—no disruption (SDS = 0)/some disruption (SDS>0); or (ii) four categories—no disruption (SDS = 0); mild disruption (0<SDS⩽3); moderate disruption (3<SDS⩽6) or marked disruption (SDS>6). The effect of women’s Pap cytology or HPV diagnosis on the presence or absence of disruption was analysed using multivariate logistic regression to compute odds ratios (OR). Goodness of fit of the model was checked using the Pearson χ2 statistic and the reported models fit the data adequately (p>0.3 for all models).
Results
The response rate was 73% (331): overall, 884 women were approached to participate of whom 453 (51%) met the eligibility criteria.
Demographic characteristics of participants are shown in table 1. Women with normal Pap smears were significantly older (p<0.001) than other participants and more likely to have a current partner, while significantly less likely to be in full time employment (data not shown). Overall, 86% of participants rated their general health as good or excellent.
Participant characteristics (n = 331)
Table 2 shows results from the HPV knowledge survey (only survey items relevant to study aims are reported). Women with a HPV-related condition were better informed about HPV. For example, these women were significantly more likely to have heard of HPV (at least 69%) and to know that it is sexually transmitted (at least 61%) than women with normal Pap results (37% and 32%, respectively). However, no significant differences in knowledge by HPV-related diagnosis were found regarding self-reported level of HPV knowledge: whether HPV can be contacted by touching, affects men and women equally, or can have an impact on fertility (data not shown).
HPV-related knowledge by participant group measured by the HPV knowledge survey
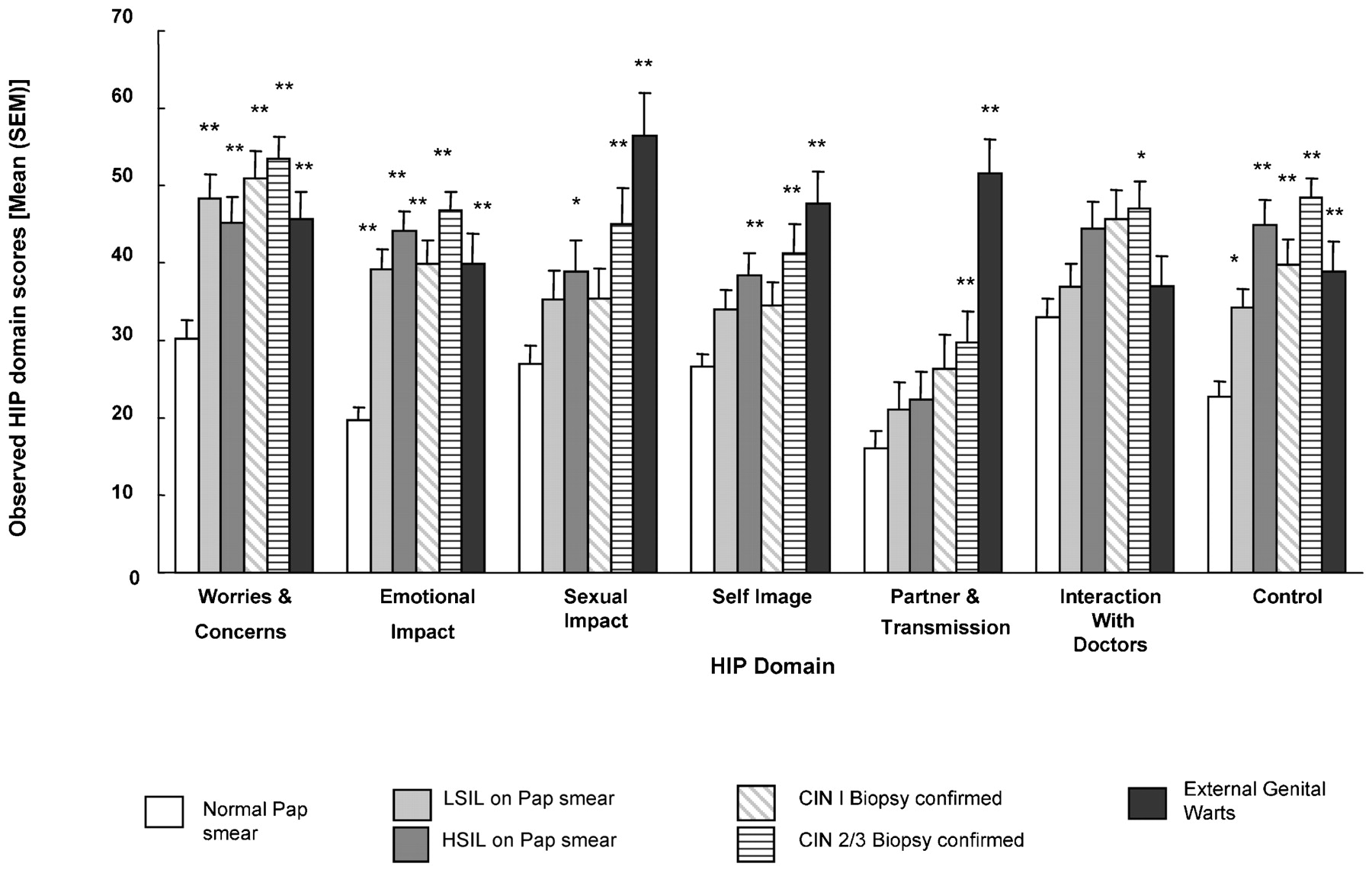
Table 3 shows the outcomes of the HIP and two QoL instruments, with significant differences in the impact of HPV-related screening interventions and disease on women after adjustment for demographic characteristics. The HIP survey was most sensitive in detecting psychosocial impact, with significantly worse impact in all women with HPV-related disease compared with those with normal Pap results (see fig 1). The HIP scores ranged from 1.4–90 (maximum possible 100). The lowest scores indicating least psychosocial impact were observed in women with normal Pap test results (25.8; 95% CI 22.6 to 29.1) and the highest by women diagnosed with CIN 2/3 (46.6; 95% CI 41.6 to 51.5). Scores for women with EGWs were similar to women with CIN 2/3 (45.7; 95% CI 40.6 to 50.9).
{kind=link}
Scores for individual human papillomavirus Impact Profile (HIP) psychosocial domains. *p<0.05; **p<0.01 adjusted for age, ethnicity and current partner, as compared with normal Pap smear group.
Quality of life results by HIP, EuroQoL VAS and SDS*
Scores for individual HIP psychosocial domains are shown in the fig 1. There is a significant difference between normal Pap test participants and, collectively, all other women for the domains “worries and concerns”, “emotional impact” and “control”. Concerns regarding “sexual impact” and “self image” are observed for women with high-grade lesions or EGWs, but not for those with low-grade lesions. Women with EGWs report concerns regarding “partner and transmission”, but not for “interaction with doctors”, whereas women with CIN 2/3 have significant concerns in both of these domains.
No association was detected between HIP score and self-report of HPV knowledge or awareness of HPV.
The EuroQoL VAS (table 3) distinguished an impact only on women with EGWs relative to the normal Pap group (p = 0.042). However, the SDS (table 3) detected a significant impact on women’s work life for all women with HPV relative to the normal Pap group, except for those with LSIL, and on social life, except for those with LSIL and HSIL. For example, the SDS found that women with EGWs were 4.5 times more likely to have their social life disrupted than women with normal Pap results after adjustment for all other demographic characteristics. The SDS detected no significant differences between groups in impact on family life.
Discussion
We found significant psychosocial impacts on women of screening for, or having a diagnosis of, HPV-related genital disease, including normal Pap tests. HPV-related psychosocial impact was detected best with the HIP, which was more sensitive and comprehensive than either the EuroQol VAS or the SDS. Analysis of the HIP psychosocial domains provided insight in to how different HPV-related diagnoses affect various aspects of women’s lives.
Previous research has explored only discrete aspects of the range of HPV-related experience. For example, one qualitative study in women with an undefined HPV diagnosis explored the impact on relationships and sex,26 while a cross-sectional survey of men and women with HPV-related disease, of whom half had experienced visible EGWs, looked at the impact in the emotional and self-image domains.27 UK women under 30 years with EGWs had EuroQoL VAS scores on average 20 points lower than population controls indicating significant negative impact on quality of life,16 plus they had generally higher levels of anxiety.28
The contribution of our study is that we used a systematic approach and disease-specific questionnaire to assess women with a range of well-defined HPV-related diagnoses. We confirmed a lower (worse) score on the EuroQoL VAS for EGWs alone of all the participant groups. The HIP detected that the largest impact of EGWs on QoL was in the domains of sexual impact, self-image, and partner and transmission.
Participants who experienced an HPV-related diagnosis were generally better informed about HPV than women with normal Pap test results probably because of information provided by the clinicians caring for them. However, we confirmed other research that found that being informed did not equate to less concern. One study investigating the impact of testing for HPV found that good knowledge of HPV had variable impact on women: some were more anxious if aware that HPV was sexually transmitted, whereas others were less anxious, viewing acquisition of HPV as a common, almost inevitable, consequence of being sexual active.29
Our study method has some limitations, which may lead to an underestimate of the impact. Our control group of women with normal Pap test results may not represent women in the general community. Our controls reported worse general health than both the other participants and population norms: age-related EuroQoL norms for women equivalent to our control group were 86.8 in the UK30 and 89.3 in the USA.31 Our control group, older than our other participants and caring for very young children, scored 77.5, which is equivalent to QoL scores for UK women over 65 years of age. The likely effect of comparing our HPV disease groups with a control group reporting relatively poor QoL is an underestimate of the impact of HPV.
Another limitation is that we cannot gauge whether the psychosocial impact of HPV on the participants in our study, drawn from two large public medical centres, are generalisable to the entire population of women.
Our results have implications for both primary care practitioners and countries considering the introduction of HPV vaccination programmes. Health practitioners performing Pap tests and managing the results need to remain cognisant that the burden of HPV is broader than just the disease it causes; even screening that eventuates in a normal result may have negative psychosocial repercussions. Consequently, prevention by vaccination of HPV-related disease that also allows less frequent cervical cytology screening of women with Pap tests will not only reduce health costs but also the psychosocial burden on women.
Key messages
Health professionals undertaking human papillomavirus-related testing and diagnoses should be aware that these activities may have adverse impacts on women’s psychosocial wellbeing.
Even normal cervical screening tests may have a negative impact on women.
External genital warts and cervical intraepithelial neoplasia 2/3 had the largest impact on women in our study
Acknowledgments
This study was supported by CSL Limited. We gratefully acknowledge the assistance of the following people who kindly gave assistance in recruitment of participants: Rosslyn Bell, Julie Silvers and the doctors at Melbourne Sexual Health Centre; Drs J Tan, M Quinn and D Palmer of the Royal Women’s Hospital and to Professor Rob Carter for his advice. We also sincerely thank the study participants for their time.
Contributors: All authors approved the final version of the manuscript. MP contributed to the conception and design of the study, drafting of the paper and revising it critically for important intellectual content. LU contributed to design and acquisition of data and drafting of the paper. AS contributed to data management, statistical analysis, interpretation of the data, drafting of the paper and revising it for important intellectual content. ELC contributed to the conception and design of the study, interpretation of the data and revising the manuscript for important intellectual content. TCM is the developer of the HIP and provided input on study design, interpretation of HIP data and assisted in revising drafts for important intellectual content. CKF contributed to conception and design, and revising the paper critically for important intellectual content. SG contributed to conception, design, acquisition, analysis, interpretation of data, drafting of the paper and overall was responsible for the coordination and management of the study.
REFERENCES
Footnotes
▸ An appendix is published online only at http://sti.bmj.com/content/vol85/issue7
Funding The name of the guarantor and funding agency is CSL Limited. The collection of data, analysis and interpretation of data, and writing of this paper were independent from its funding source.
Competing interests AS and ELC are employed by CSL Limited and own stock in CSL Limited. TCM is employed by Merck & Co, Inc. CKF owns shares in CSL Biotherapies, has received honoraria from CSL Biotherapies and Glaxo SmithKline and a research grant from CSL Biotherapies. SG has received advisory board fees and grant support from CSL Limited and GlaxoSmithKline, and lecture and consultancy fees from Merck & Co, Inc. SG reports having previously owned stock in CSL Limited. SG has received grant support through her institution from Merck and GlaxoSmithKline to do clinical trials for HPV/cervical cancer vaccines.
Ethics approval Obtained from the relevant committees of the Royal Women’s and Alfred Hospitals.
Provenance and Peer review Not commissioned; externally peer reviewed.
Linked Articles
- Whistlestop tour