Article Text

Abstract
Objectives To estimate for the first time the incidence and healthcare resource utilisation associated with genital warts (GW) in Australia prior to the human papillomavirus vaccination programme.
Method The authors analysed data from the nationally representative Bettering the Evaluation of Care and Health general practice cross-sectional programme and from the National Hospital Morbidity Database to estimate age-related incidence and community (non-hospital) and hospital-related costs (in 2009 Australian dollars) associated with medical treatment of GW.
Results The authors estimated an annual incidence of 2.19 cases of GW per 1000 Australians (95% CI 1.88 to 2.49), with peak incidence in women aged 20–24 years at 8.61 cases per 1000 and in men aged 25–29 years at 7.40 cases per 1000. The estimated number of consultations per GW case was 2.9 (95% CI 2.5 to 3.3) for women and 2.8 (95% CI 2.3 to 3.2) for men. Ablative treatments in general practice were more common in men (60% of consultations) than in women (37% of consultations). In contrast, more women (16% vs 8%) were referred to specialists, and 75% of ablative procedures requiring hospitalisation were performed in women. The annual cost of management of GW is over A$14 million, with an estimated cost per treated case of A$251 for men and A$386 for women.
Conclusions GW impose a large health and cost burden on Australians. The national immunisation programme with the quadrivalent human papillomavirus vaccine has the potential to greatly reduce this burden, and future research measuring its impact is keenly anticipated.
- Condylomata acuminata
- incidence
- cost of illness
- family practice
- general practice
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Introduction
Assessments of the health and economic burden of genital warts (GW) are critical in evaluating the impact and cost-effectiveness of human papillomavirus (HPV) vaccination programmes. While both licensed HPV vaccines protect women from oncogenic HPV types 16 and 18, which cause the majority of cervical cancers, the quadrivalent vaccine used in Australia also protects against HPV types 6 and 11 that cause approximately 90% of GW.1 GW are one of the most common sexually transmitted viral infections with self-reported lifetime prevalence of approximately 4% in Australians aged 16–59 years,2 5.6% in Americans aged 18–59 years3 and 11% in women aged 18–45 years in Nordic countries.4 In the UK, there has been a 29% increase in diagnoses of first-episode GW reported between 1999 and 2008.5
In Australia, GW are primarily treated by general practitioners (GPs) (57%), with an additional 17% of people managed in sexual-health clinics.2 In this study, we use data from a nationally representative general practice database and from the National Hospital Morbidity Database, to estimate for the first time the incidence and healthcare resource utilisation associated with GW in Australia prior to introduction of the national HPV vaccination programme.6
Methods
Incidence of GW
Age-specific incidence of GW was estimated from the Bettering the Evaluation of Care and Health (BEACH) cross-sectional database. Each year, nationally representative random samples of approximately 1000 practising GPs record details of 100 consecutive patient consultations.7 Patient reasons for consultation, problems managed, therapeutic procedures, clinical treatments, referrals, pathology and imaging tests are classified using the International Classification of Primary Care—Version 2.8 Medications are classified using the Anatomic Therapeutic Chemical classification.9
From April 2000 to September 2006, consultations for female and male condylomata acuminata (ICPC-2 Codes X91 and Y76) were extracted. Incidence was estimated from the annualised consultation rate for ‘new’ GW problems (defined as those never managed by any doctor or a first medical consultation for a new episode of a recurrent problem, designated by GP at consultation), stratified by gender and age, extrapolated to the total annualised GP attendances over the same period10 and normalised to the corresponding 2004 Australian population.11
People with GW managed in sexual-health clinics are not captured by BEACH. For every patient with GW managed by GPs, an estimated 0.298 are managed in sexual-health clinics.2 Therefore, incidence rates were adjusted by multiplying by 1.298 to account for GW cases managed in sexual-health clinics. Respondents not seeking medical treatment for GW are not accounted for in our estimates.
Healthcare burden of GW
We estimated two cost components: the cost per case of GW treatment by GPs and the cost per case of GW treatment in hospitals. The analysis is restricted to direct medical costs incurred by government and/or patients. No additional societal costs are included. Costs are reported in 2009 Australian dollars. (On 6 November 2009, the A$ was worth approximately €0.61, £0.55, US$0.91 and C$0.97.)
General practice
The annual national estimates of ‘new’ and ‘old’ GW cases were determined from BEACH. The average number of GP consultations per GW episode was obtained as the ratio: estimated annual total consultations for GW/estimated annual new consultations for GW.12
Costs of GP visits for GW were determined using the type of medical consultation reported in BEACH and its corresponding unit cost from the Medicare Benefits Schedule (August 2009; see appendix). Adjustments were made for Healthcare Card (HCC) holders, where an additional reimbursement is paid to GPs for billing at the standard rate13 and for non-HCC holders, where out-of-pocket expenses were included by multiplying the appropriate Medicare Benefit by a patient-billed relativity factor (1.59 for GP attendances).14
Full consultation costs were applied to the proportion of GP visits wherein only one problem was managed; if more problems were managed, the cost was divided by that number.
The rate of GP specialist referrals for GW was obtained from BEACH. The cost for an initial referred specialist consultation (appendix) was adjusted for out-of-pocket expenses for non-HCC holders as described above (patient billed relativity of 1.72).
The numbers and types of treatments prescribed, supplied or recommended for over-the-counter purchase for GW at consultations were obtained from BEACH. There is no additional reimbursement for ablative treatments performed as part of a GP consultation. Topical treatments unit costs were obtained from MIMS OnLine (appendix).15
Costs for sexual-health clinic consultations were assumed to be equivalent to GP consultations. Costs of pathology services could not be obtained from pathology orders data in BEACH and are excluded from this analysis.
Hospital procedures
Number and same-day status of hospitalisation episodes (public and private) for vulvovaginal, penile and anal warts (Australian Classifiaction of Health Interventions procedure codes 35507, 36815, 32177, respectively) were determined from the National Hospital Morbidity Database from July 2000 to June 2007.16
Hospitalisation costs are reported for Australian Refined Diagnosis Related Groups, which include multiple-day procedures. To estimate the costs of the GW procedures in public hospitals (appendix) the same-day Victorian cost weights for the DRG codes most closely related to each procedure (Australian Refined Diagnosis Related Groups N09Z, M03B and G11B for vulvovaginal, penile and anal warts, respectively)17 18 were applied to the average public hospitalisation cost for 2008–2009 (Public Weighted Inlier Equivalent Separation payment WIES15: $3468). Costs in private hospitals were assumed to be equivalent to costs in public hospitals. A small number of ablation treatments reimbursed as Medicare Benefits Schedule items may be performed by specialists outside hospital and hence have not been accounted for in our estimates.
Statistical analyses
BEACH is a cluster sample design with the GP as the primary sampling unit, and the GP–patient consultation as the unit of analysis. Robust 95% CI around the point estimates which account for the cluster sample design are reported, using procedures in SAS software (SAS version 9.1, SAS Institute). Non-overlapping 95% CI indicate a statistically significant difference at α=0.05.
Results
National age-specific incidence of GW
From April 2000 to September 2006, data were available from 6460 GPs for about 646 000 consultations (59% female, 41% male). GW were managed at 639 consultations (0.1%), with approximately 35% of these indicated as ‘new problems.’ Table 1 displays extrapolations from these data to estimate the annual number of new GW diagnoses in general practice and incidence rates. When adjusted for people presenting to sexual-health clinics, there were approximately 43 900 (95% CI 37 850–50 050) new cases of GW presenting annually (∼23 350 female, 20 550 male), providing an annual incidence of 2.19 cases per 1000 Australians (95% CI 1.88 to 2.49).
National age-specific genital wart (GW) incidence extrapolated from Bettering the Evaluation of Care and Health (BEACH) data for all GPs and sexual-health clinics
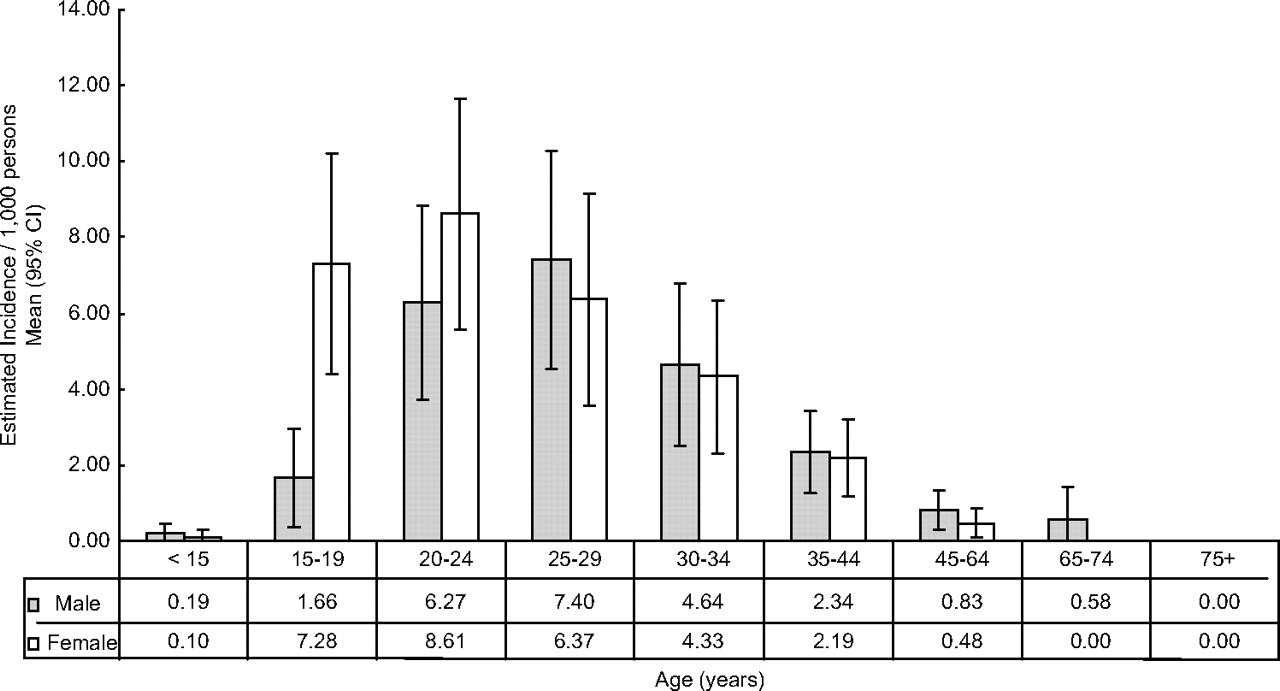
Age- and sex-specific rates of GW incident cases in Australia (BEACH adjusted for sexual-health clinics) are presented in figure 1. GW incidence peaked in women aged 20–24 years at 8.61 cases per 1000 and in men aged 25–29 years at 7.40 cases per 1000.
{kind=link}
Rates of incident genital wart (GW) cases (per 1000 persons) stratified by age and gender. All consultations for female and male GW (ICPC-2 Codes X91 and Y76) from April 2000 to September 2006 were extracted from the Bettering the Evaluation of Care and Health database. Incidence was estimated from the annualised consultation rate for ‘new’ GW problems stratified by gender and age, extrapolated to the total annualised GP attendances over the same period, and normalised to the corresponding 2004 Australian population. The resulting incidence rates were adjusted to include GW treated in sexual-health clinics (see Methods).
Resource utilisation
General practice data
Extrapolating from the BEACH database from April 2000 to September 2006, we estimated 95 700 (95% CI 86 450 to 105 000) GP consultations per year for GW, 54% being with women (table 1). The estimated number of consultations per GW case was 2.9 (95% CI 2.5 to 3.3) for women and 2.8 (95% CI 2.3 to 3.2) for men.
Most consultations (∼75%) were Medicare standard consultations, with ∼21% long and 1.2% prolonged consultations (table 2). Women were significantly more likely than men to have a long consultation. Table 2 also shows the weighted average cost of a GP consultation by gender, unadjusted and when adjusted for number of problems managed. Approximately half the consultations involved one problem (48% women, 51% men); 36%/37% two problems and 12.5%/8.5% three problems, and 3.5% of consultations with both women and men had four problems managed.
GP consultations for genital warts (GW)
Treatments used for GW in general practice are summarised in table 3. Medications were prescribed, supplied or recommended for ∼28% of all GW problems managed. Topical medications for GW, imiquimod or podophyllum resin-based, were prescribed at similar rates in ∼26% of consultations with women and 22% of consultations with men. Topical medications were prescribed more often in consultations for new GW problems (∼27% vs 17% in subsequent consultations). The cost of topical medications per GW consultation was A$24 for women and A$20 for men.
Genital wart (GW) management
Ablative treatments were performed significantly more often in men (∼60% of consultations) than in women (∼37%, table 3), with similar rates across initial and subsequent consultations. Women were significantly more likely to be provided counselling treatment (∼28% vs 19% for men). The difference was most marked in initial GW consultations, in which counselling, advice or reassurance was recorded for 62% of women and 24% of men, decreasing to 22% and 16% respectively in subsequent consultations.
Women were significantly more likely to be referred to a specialist (16% vs 8% for men, table 3), translating to an additional cost per GP consultation of ∼A$17 for women and ∼A$8 for men.
Most pathology tests ordered were for sexually transmitted infections. Pap smears were performed in ∼7% of GW consultations with women.
The total cost of a GP consultation for management of GW was estimated at A$83 for women and A$71 for men. As women and men had 2.9 or 2.8 consultations, total GP management costs were estimated at A$240 and A$196 per GW case respectively (table 4). This extrapolates to yearly costs in the general practice setting of approximately A$5.6 million for the estimated 23 350 new GW cases presenting in women each year and approximately A$4.0 million for the estimated 20 550 new GW cases in men.
Cost of genital wart (GW) management
Hospital-based procedures for GW treatment
Between July 2000 and June 2007, there was an average of 2501 hospitalisations recorded annually for GW procedures in women and 829 in men. In women, procedures were for destruction of vulval warts (57%), vaginal warts (25%) and anal warts (17%). Same-day hospitalisations were recorded for 93% of vulvovaginal wart and 88% of anal wart procedures. The average cost of ablative procedures for women was estimated at A$1370, giving an annual cost of approximately A$3.4 million. Assuming 23 350 new female GW cases each year, in-hospital ablative procedures cost approximately A$145 per case (table 4).
Most procedures in men were for destruction of anal warts (88%) or penile warts (12%). Same-day hospitalisations were recorded for 86% of anal wart and 96% of penile wart procedures. The average cost of ablative procedures for men was estimated at A$1429, translating to a yearly cost of approximately A$1.1 million. Assuming 20 550 new male GW cases presenting annually, in-hospital ablative procedures cost approximately A$55 per male case (table 4).
Therefore, the annual total cost of management of GW is over A$14 million, with an estimated cost per treated case of A$386 for women and A$251 for men (table 4).
Discussion
This study is the first to estimate Australian annual incidence and costs associated with clinician diagnosed GW. During 2000–2006, we found an annual incidence of GW of 2.19 per 1000 people. Costs of GW management were estimated at A$386 per case for women and A$251 for men.
Our estimated incidence is somewhat higher than recent reports from similar studies overseas using representative health claims data: 1.26 per 1000 in British Columbia19 and 1.52 per 1000 in UK genitourinary clinics in 2008.20 While acknowledging potential for misclassification of incident (‘new’) cases in our study, the similarity in the average number of consultations per GW case between our study (2.8–2.9) and that of Marra et al (2.7–2.8),19 Insinga et al (3.1),21 and Woodhall et al (2.5–3.1)22 suggests that this is not the case. Hoy et al recently reported an incidence of 1.2 per 1000 in USA private health plans, but this is acknowledged as an underestimate, as it does not capture cases managed through sexual-health clinics.23
Peak ages for Australian GW patients seeking treatment from GPs (20–24 years in women and 25–29 years in men) are comparable with those attending sexual-health clinics24 and are similar to those in the US21 and Canada,19 whereas in the UK and Nordic countries, 20–24 years is the peak age for both genders.4 25
Ablative treatments in general practice are more common in men (60% of consultations) than in women (37% of consultations). In contrast, more women (16% vs 8%) are referred to specialists, and 76% of ablative procedures requiring hospitalisation are performed in women. This is consistent with a previous report on GP management of sexually transmitted infections based on an earlier analysis of the BEACH database26 but contrasts with our previous research in sexual-health clinics24 where ablative treatments are performed in similar proportions of men and women, with very few patients referred on to other services (∼1.5%), reflecting the specialised nature of such clinics. Patient purchased topical treatments for GW are prescribed or recommended in ∼24% of GP consultations, with similar rates of prescription of imiquimod and podophyllum resin based treatments. Rates of topical treatment use are similar in sexual-health clinics, but the cheaper podophyllum resin-based option represents 79% of such treatments.24
Our study estimates approximately 3300 hospitalisations per year for GW procedures. The number of hospitalisations as a percentage of GW cases (∼7%) is consistent with Canadian data, reporting hospital management in 9% of GW episodes.19 Similarly, 11% of patients with recurrent GW, and 19% of patients with resistant GW, are hospitalised in Germany.27 In contrast, hospital management of GW was rarely encountered in US analyses of administrative claims from private health funds, possibly reflecting the study method.21 22
Our estimated cost of A$386 per GW case in women is substantially higher than the A$251 estimated in men, reflecting higher rates of specialist referrals and hospitalisations. Treatment costs for women are also higher in Germany (€414 compared with €315 in men)27 and similar in Canada (C$207 vs C $176 in men)19 and the UK (US$292 vs US$280 in men),22 and appear to be reversed in the USA (US$528 vs US$745 in men).21 23
Our study has several limitations. As discussed above, the definiton of ‘new’ in BEACH data may lead to an overestimation of the number of new cases by including recurrences, although as the number of visits per case is similar to other countries, we think this unlikely. Also, the adjustment to reflect 17% of cases managed in sexual-health clinics is based on self-report.2 In addition, we have assumed costs in sexual-health clinics reflect GP costs, which may not be the case, given the differences in treatment patterns discussed above. This study assumed that all GP referrals of patients to specialists were acted upon, and all prescriptions were purchased, thus potentially slightly overestimating costs. However, as there are no data sources available to accurately quantify specialist follow-up of GW in Australia, the costs of management following referral are restricted to hospitalisation costs only and are thus likely underestimated. Although hospitalisation costs were based on relatively broad diagnosis-related groups rather than on specific procedures, it is unlikely that they have been overestimated, as we have applied same-day costs to all hospitalisations.
GW are an important issue in the Australian healthcare system, with high incidence in younger people and costs estimated to be over A$14 million annually. This monetary burden does not include the additional psychosocial implications, which can be significant.28 Reductions in GW cases in young women presenting to sexual-health clinics associated with the introduction of the HPV vaccination programme have recently been reported.29 The baseline data in this study lay the foundation for measuring the population impact of the HPV vaccination programme in the general practice and hospital settings.
Key messages
During 2000–2006, the annual incidence of GW in Australia was 2.19 per 1000 people.
The costs of managing GW in Australia were estimated at A$386 per case for women and A$251 for men.
The peak ages for Australians to present for treatment to GPs with GW are 20–24 years in women and 25–29 years in men.
Acknowledgments
The authors wish to thank J Watts for her advice on same-day hospitalisation costs.
Appendix
| GP/Specialist consultation costs | |||
| MBS Item no* | Description of service | MBS fee ($A) | Patient-billed cost† ($A) |
| 3 | Short consultation | 15.35 | 24.42 |
| 23 | Standard consultation | 33.55 | 53.38 |
| 36 | Long consultation | 63.75 | 101.44 |
| 44 | Prolonged consultation | 93.80 | 149.25 |
| 24 | Home visits | 57.05 | 90.78 |
| 23 | Other—assume standard consultation | 33.55 | 53.38 |
| 104 | Initial attendance specialist, referred consultation | 79.05 | 115.38 |
| 10990 | Healthcare card (HCC)/bulk billing rebate | 6.50 | NA |
| 10991 | Non-capital city HCC/bulk billing rebate | 9.80 | NA |
| Prescription costs‡ | |||
| Brand name | Generic name | MIMS August 2009 ($A) | |
| Aldara | Imiquimod | 159.52 | |
| Podophyllum resin topical 0.5% | Podophyllum resin | 10.46 | |
| Condyline paint | Podophyllotoxin | 54.80 | |
| Posafilin | Podophyllum resin | 10.46 | |
| Wartec cream | Podophyllotoxin | 60.25 | |
| Wartec solution | Podophyllotoxin | 55.00 | |
| Hospitalisation costs | |||
| VIC-DRG | Related procedures | Public hospital same-day costs ($A) | |
| G11B | 32177: Removal of anal warts | 1306 | |
| N09Z | 35507-00/ 35507-01: Destruction of vaginal or vulval warts | 1383 | |
| M03B | 36815: Destruction of penile warts | 2304 | |
Fees and costs used to calculate cost of genital warts (GW) treatment
References
Footnotes
Funding During the data period used in this study, the BEACH programme was funded under research contracts with: the National Prescribing Service Ltd; the Australian government Department of Health and Ageing; AstraZeneca Pty Ltd (Australia); Janssen-Cilag Pty Ltd; Merck, Sharp and Dohme (Australia) Pty Ltd; Roche Products Pty Ltd; Sanofi-Aventis Australia Pty Ltd; the Australian government Department of Veterans' Affairs; and the Department of Employment and Workplace Relations.
Competing interests ELC and AS are employed by CSL Limited and own stock in CSL Limited. SG has received advisory board fees and grant support from CSL Biotherapies and GlaxoSmithKline, and lecture fees from Merck and GSK. SG has received funding through her institution to conduct HPV vaccine studies for MSD and GSK. CSL Biotherapies Pty Ltd commissioned reports on the general practice management of genital warts from BEACH (HB and CH).
Ethics approval Ethics approval was provided by the Human Ethics Committee of the University of Sydney and the Ethics Committee of the Australian Institute of Health and Welfare.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Whistlestop tour