Article Text

Abstract
Background The aetiology of bacterial vaginosis (BV) remains unknown.
Objective To describe longitudinal changes in vaginal microbiota.
Methods Thirty-nine women (mean age 36.8 years; 22 (56.4%) African-American) self-collected vaginal specimens twice weekly for 16 weeks as part of a vaginal douching cessation study. In an analysis where each woman serves as her own control, conditional logistic regression was used to evaluate daily, time-varying factors associated with a woman's incident BV episode(s) as compared with her persistently BV-negative sample(s). BV was defined by a Nugent's Gram stain score ≥7.
Results 46.2% of participants had BV in the first 4 weeks of observation. Rapid fluctuation of vaginal microbiota was observed in 226 transitions to BV or spontaneous remission. Duration of BV was often short: 51% of the episodes lasted for only one sample interval (3 days). Among women who had at least one BV episode, the median number of episodes per woman was 8.7 (SD 7.4, range 1–22). Lubricant use 1 day before specimen collection (adjusted OR (aOR)=11.75, 95% CI 1.96 to 70.27) and rectal sex 2 days before (aOR=4.48, 95% CI 2.79 to 7.17) were associated with BV onset.
Conclusion Rapid fluctuation of the vaginal microbiota was seen. Longitudinal studies with long intervals between sampling are likely to miss episodes of BV. Recent report of lubricant use and rectal sex were associated with incident BV.
- Bacterial vaginosis
- Nugent score
- Gram stain
- vaginal microbiota
- epidemiology
Statistics from Altmetric.com
Introduction
The vaginal microbiota have an important protective role in maintaining the health of women. Disruption of the mutual relationship that exists between microbial communities in the vagina and their hosts can lead to bacterial vaginosis (BV), a condition traditionally characterised by a shift in the composition and structure of vaginal microbial communities that results in decreased numbers of lactic acid producing bacteria and elevated vaginal pH.1 BV has been shown to be an independent risk factor for adverse outcomes, including preterm delivery and low infant birth weight, acquisition of sexually transmitted infections and development of pelvic inflammatory disease.2–5 Nationally representative surveys in the USA indicate that the prevalence of BV is 29% by Gram stain analysis of vaginal fluid,6 and despite considerable effort, the aetiology of BV remains unknown. Moreover, recurrence after antibiotic treatment is common.7
In reproductive-age woman, the vaginal microbiota have been shown by cultivation methods to be a dynamic ecosystem subject to shifts over the time course of the menstrual cycle.8 Vaginal microbial communities may also experience various kinds of chronic and acute disturbances caused by exogenous and endogenous factors such as the use of antibiotics, hormonal contraceptives, sexual intercourse, vaginal lubricants, vaginal douching, ageing, phase of the menstrual cycle, pregnancy and stress.9–16
Prospective longitudinal sampling is required to evaluate the factors which may lead to shifts in the composition of the vaginal microbiota. However, the majority of existing epidemiological studies of BV were designed such that samples were collected cross-sectionally (at the time BV was diagnosed), monthly or less frequently, and therefore are not adequate for examining the short-term structural and compositional variations of vaginal microbial communities. There are a few prospective studies with high frequency sampling, and each has suggested a role for several important time-varying behaviours.12 13 17 18
We sought to conduct an epidemiological analysis of daily, time-varying factors and their relation to the incidence of BV as defined by Gram stain in a study of vaginal specimens which were self-collected twice weekly for 16 weeks. As there are many studies on population-level risk factors for BV6 (studies which compare risk factors between women), we used a case-crossover analysis in which each participant acts as her own control during prospective BV and non-BV intervals. The strength of this approach is that we did not need to account for all the variation (and confounding) that occurs between women and we could decipher the factors which were associated with an individual woman's risk for incident BV.
Materials and methods
Cohort design
Thirty-nine non-pregnant women who reported the use of vaginal douche products in the 2 months before screening were enrolled in the parent study—a vaginal douching cessation pilot study.19 Participants were asked to continue their usual practice and frequency (same hygiene products as they normally used) of vaginal douching during a 4-week observation (phase I) and then to stop using all feminine hygiene products for the following 12 weeks (phase II). Thirty-three women successfully completed the longitudinal study (85%). Participants were screened for pregnancy (urine human chorionic gonadotropin), Chlamydia trachomatis and Neisseria gonorrhoeae (nucleic acid amplification, Becton Dickinson, Sparks, Maryland, BD ProbeTec ET) at enrolment and final visits.
Self-collected vaginal smears were obtained twice weekly during the 16-week study. Behavioural diaries included a daily yes/no check list to report menstrual bleeding, vaginal douching, sexual activity (vaginal intercourse, receptive oral sex, digital penetration, rectal sex, sex toys, condoms, spermicides, lubricants), thong undergarment, drugs, use of a diaphragm, sanitary napkin and tampons. These daily, time-varying variables are the focus of the current analysis.
Participants sent the vaginal smears and diaries by mail to the laboratory weekly and one microbiologist batched and evaluated the slides in random order. Vaginal smears were Gram stained, and a microscopy score of 0–10 was assigned using the standardised method described by Nugent et al.20 The Nugent score represents an estimate of the range of vaginal bacterial morphotypes which are characteristic of BV – high Nugent scores reflect absence of Lactobacillus with presence of strict anaerobes Gardnerella and Mobiluncus sp., and low Nugent scores represent the opposite with high abundance of Lactobacillus species and relative absence of anaerobes. A score of 0–3 is considered normal, 4–6 is designated intermediate state and 7–10 is considered BV. Gram stains were evaluated microscopically for polymorphonuclear leucocytes quantified on the basis of the number present per field (×1000). Samples were positive for neutrophils if there was one or more per field. In this analysis, BV was defined by a Nugent score ≥7. With a sensitivity of 89% and specificity of 83%21 compared with Amsel's clinical criteria,22 the Nugent score is a useful research tool,6 and it can be performed on self-collected vaginal smears,23 facilitating longitudinal field-based studies.12 19
The protocol was approved by the institutional review board of the Johns Hopkins University School of Medicine and the University of Maryland School of Medicine. All participants provided written informed consent.
Case crossover analysis
In this longitudinal analysis of vaginal smears, participants served as their own control. A woman had to have experienced both BV onset and persistently negative samples to be included in the model (n=22). The outcome was observation of incident BV, defined by a BV-positive sample which was immediately preceded by a BV-negative sample. The incident BV sample was compared with a woman's own persistently negative samples defined by the second BV-negative sample in a series. Sample intervals were approximately 3 days (twice weekly). Seventy-four incident BV intervals and 340 persistently normal microbiota intervals were available for modelling.
Conditional logistic regression was used to evaluate time-varying factors associated with a woman's incident BV compared with her persistently normal intervals. Because each woman serves as her own control, this approach eliminates problems of confounding by time-invariant factors24 such as risk history and demographics. The model can also account for within-subject correlations.
Time-varying factors collected from daily diaries that had been identified on the basis of previous publications, biological plausibility and preliminary univariable analyses were evaluated as possible confounders. In addition, the regression analyses were performed with backward and forward selection procedures to verify the significant predictors of incident BV. Model fit was also evaluated using Akaike's information criteria. Variables that were felt to be biologically relevant, even if they did not achieve statistical significance, were retained in the final model. Data were analysed using STATA/SE 10.0 for Windows (Stata Corporation).
Results
Parent study cohort (n=39)
The mean age of the study participants was 36.8 years (range 22–53); and 22 (56.4%) were African-American, while 14 (35.9%) were white and three (7.7%) other ethnicities. During the study observation period, participants reported engaging in douching (95%), vaginal lubricant use (26%) and vaginal intercourse (82%). Nine women (23%) reported rectal sex—six women reported the act on just 1 day and the other three women reported on four, seven and 15 days. One woman was prescribed metronidazole for symptomatic BV and four women recorded the use of vaginal antimycotics (topical, over the counter). Among women who completed the 16-week study (n=33), the average number of longitudinally collected specimens per woman was 32.3 (SD 1.2, range 29–34) and behavioural dairies were submitted from 99% of enrolment weeks.19
Rapid fluctuation in BV status was often seen. A total of 226 transitions between normal, intermediate and BV were documented (figure 1). Of the 113 observed remissions, all but one were spontaneous (not the result of antibiotic treatment). Of the 33 women who completed the study, nine women (27%) were found to have persistently normal vaginal microbiota, while the status of 16 women (48%) fluctuated, as defined by two or more fluctuations between normal and BV (table 1). Condom use (ever) was the only significant factor which differed between BV fluctuation groups (table 2).
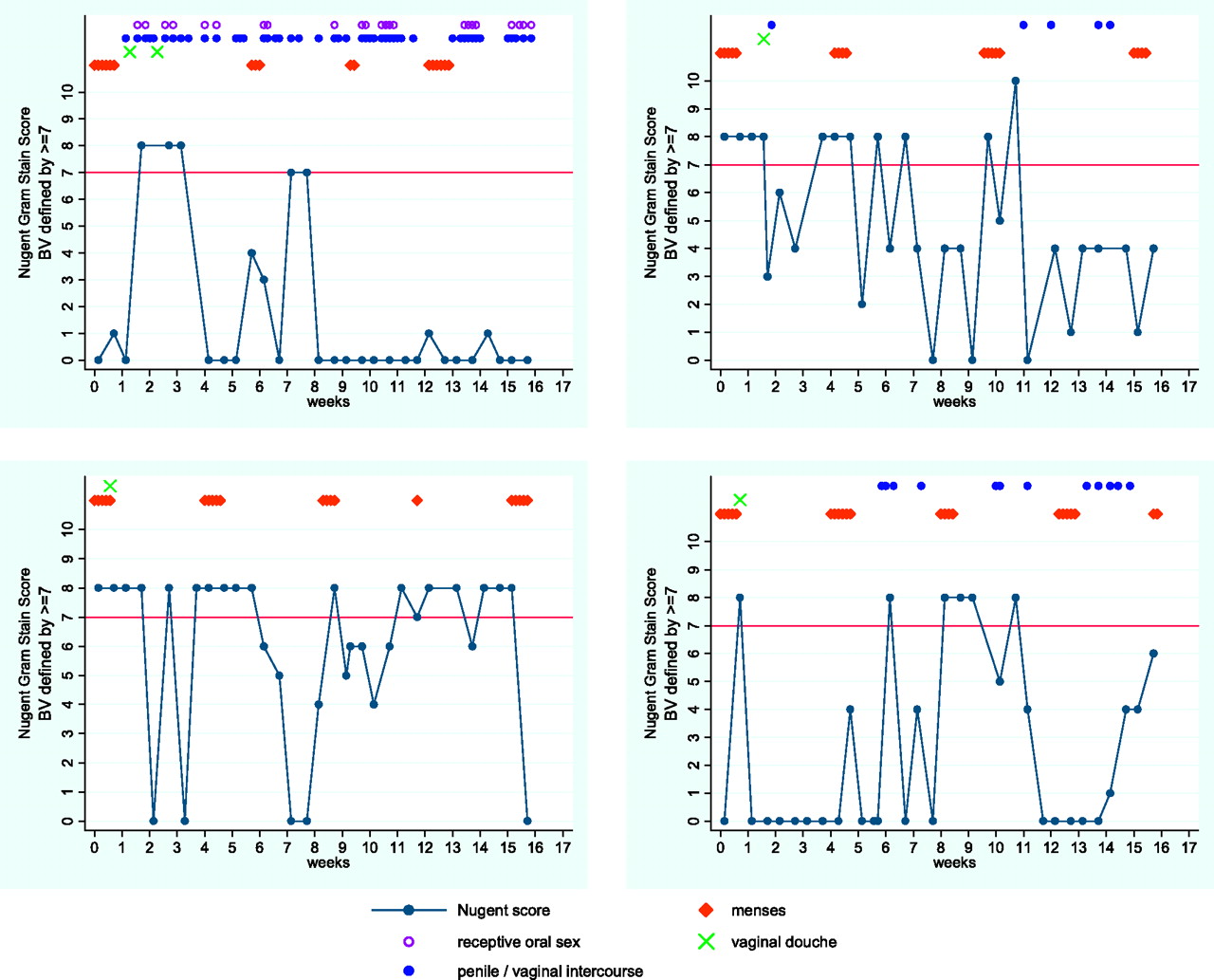
Nugent Gram stain score fluctuation in four participants over the course of the 16-week study. BV, bacterial vaginosis.
Number of women with fluctuation of vaginal microbiota over 16 weeks as defined by Nugent's Gram stain score (n=33)*
Descriptive characteristics of women by fluctuation status of Nugent's Gram's stain score* during 16 weeks of twice-weekly specimen collection, Baltimore, Maryland, USA, 2006–7, n=33†
The duration of BV varied widely, but often (51%) was very short, one sample interval lasting <3 days (figure 2). Among women who had episodes of BV, the mean number of episodes observed was 8.7 (SD 7.4, range 1–22, median 6), with an average of approximately two episodes a month. The estimated average number of sample-days observed with BV was 5.1 (SD 7.2, range 1–35, median 1).

{kind=link}
{kind=link}
Duration of bacterial vaginosis (BV) based on Nugent's Gram stain scores of vaginal swabs obtained twice weekly. Sample intervals were approximately 3 days.
Case crossover analysis
Demographics for the subsample included in the case crossover analysis (women with at least one BV episode and one persistently normal interval, n=22) are shown in table 2 (Fluctuation column). The mean age of the subsample was 36.5 years (range 22–48).
To determine time-varying factors associated with BV onset, we contrasted factors that preceded BV onset with those reported during observation intervals of normal microbiota. In multivariable modelling, menses in the previous 10 days (aOR=2.28, 95% CI 1.11 to 4.70), vaginal lubricant use reported the day before (aOR=11.75, 95% CI 1.96 to 70.27) and rectal sex within 2 days before (aOR=4.48, 95% CI 2.79 to 7.17) were all associated with a woman's BV onset as compared with her persistently normal samples (table 3). The adjusted point estimate for vaginal douching practised the day before suggested a trend that douching is associated with BV onset, but it was not statistically significant (aOR=3.71, 95% CI 0.79 to 17.36).
Case crossover analysis for risk of incident bacterial vaginosis compared with persistently normal samples by exposures occurring in the 1–3 days before specimen sampling* (n=20)
As a proxy for vaginal inflammation, we adjusted for white blood cell presence and the point estimates were not affected. The analysis also demonstrated that sexual activities (vaginal intercourse 1 day before), receptive oral sex (1–3 days before), digital penetration (1 day before), insertive sex toy use (3 days before) resulted in positive point estimates in their univariable association with BV onset but were not statistically significant (table 3).
When BV outcome was defined by a Nugent score ≥4 (representing intermediate category), the results were similar except that menses and rectal sex were no longer statistically significant in multivariable modelling (data not shown). Duration of menstruation (1–3, 4–6, ≥7 days) and vaginal intercourse immediately after menstruation (1–3, 4–7, 8–11, ≥12 days) were also not significantly associated with incident BV (data not shown).
Discussion
As defined by Nugent's Gram stain score,20 our study confirms that women may have short episodes of BV or compositional changes in vaginal microbiota that spontaneously resolve. It was surprising that half of the enrolled women had rapid fluctuation in their vaginal microbial communities. This observation reveals a weakness of traditional cross-sectional or long-interval sampling studies, as BV episodes will be missed if samples are collected on a single observation or are collected weekly, monthly or less frequently. Such studies would underestimate the incidence of BV and the number of recurrences. Our data also indicate that physical disturbances may be associated with BV onset. It is, however, not clear why these changes of the microbiota occur in some women after such activities (or menses) but not in all women. We hypothesise that vaginal microbial community types vary between women and that a number of community types are more susceptible to disturbance and subsequent risk for BV.
Poor sampling technique or observation error cannot account entirely for our observed fluctuations in Nugent scores. Several longitudinal studies with daily sampling have documented rapid fluctuation in Gram stain vaginal smears.13 17 18 25
Lubricant use was a strong predictor of BV onset in this study. Lubricants contain a wide variety of ingredients, including glycerin and chlorhexidine. Chlorhexidine is a broad spectrum microbicide that may cause significant toxic effects to mucosal surfaces. Glycerin may increase local osmolarity and its effect on protective lactic acid producing bacteria is not known.
We also found that rectal sex was associated with BV onset. This association was inferred from only five women, but the point estimate was significant with a reasonably tight 95% CI. Transfer of micro-organisms from the rectum to the vagina may disrupt the vaginal equilibrium or induce local inflammatory responses that may lead to an increased susceptibility to changes in the vaginal microbiota and BV. Despite the frequent report of this sexual practice by women (25% of participants in the parent study), data on the association between rectal sex and BV are scarce and conflicting.26–28
In this analysis, douching the day before was marginally associated with BV onset. Because samples were collected every 3 days, the study design was not adequate to determine if the observed association was causal or due to women douching in response to BV symptoms.
A strength and unique aspect of our study is the analytical method which allows each woman to serve as her own control. Therefore, we do not need to control for time-independent factors which vary between women (such as age or medical history). However, a limitation of this case-crossover approach is that only women who have discordant pairs (women with fluctuating BV status) contribute to the analytical model. Our results, however, are consistent with standard between-woman evaluations of time-varying risk factors.12
There are several limitations to our study. Time-varying exposures noted as associated with BV onset are hypothesis generating and therefore were not corrected for multiple comparisons. Our findings were data driven. It is not known what time frame, whether 1 or 3 days before sampling, should be used to evaluate different intravaginal exposures. In addition, daily information on vaginal symptoms was not collected. As the parent study was a longitudinal field-based study with self-sampling, the study design did not include evaluation for BV by Amsel's clinical criteria.22 The study population may also not be generalisable. The study recruited women who reported use of vaginal douche products, and this population may represent a group of women who have increased variability in their vaginal microbiota. However, the reasons for douching were varied19 and as demonstrated by 27% of women persisting with normal Nugent scores throughout the 16 weeks of observation, women with both disturbed and undisturbed vaginal microbiota were sampled. African-American women were over-represented in the cohort and they are at higher risk for BV6 and potentially recurrent BV. Fifty-seven per cent of this cohort had at least one episode of BV, while data from a nationally representative survey found a prevalence of BV of approximately 38% among US women who reported recent douching.6 Finally, risk for BV may be modulated by contraceptive method15 and 45% of participants reported a history of tubal ligation.
Both the aetiology of BV and the vaginal microbiome remain poorly understood. It is not known how the transient fluctuations observed on Gram stain reflect a clinician's diagnosis of BV. The fluctuations may represent temporary states of limited clinical significance. However, future research on the implications of longitudinal changes in vaginal microbiota is warranted. If a healthy microbiota is a protective state and a BV or disrupted microbiota is viewed as a non-protective state (guards down) in part because of the bactericidal and virucidal actions of lactic acid, fluctuations of vaginal microbial communities may result in intervals of increased susceptibility to sexually transmitted infections and HIV.3 4 29–31 Use of new molecular technologies will facilitate a more comprehensive understanding of the changes in vaginal microbial populations that characterise BV and the differences in microbial species composition and abundance that occur between healthy and BV-prone microbiota.
Together with previous studies,13 17 18 25 we have highlighted the dynamic nature of the vaginal microbiota and demonstrated the need for frequent prospective sampling in order to significantly advance our understanding of the dynamics of vaginal microbiota structure and function, and the microbiological, biochemical, molecular and behavioural contributions to onset and remission of BV.
Key messages
Rapid fluctuations in vaginal bacterial communities are common.
Women may have short episodes of bacterial vaginosis that spontaneously resolve without antibiotic treatment.
Longitudinal studies may miss bacterial vaginosis episodes if samples are collected infrequently.
Recent report of lubricant use and rectal sex were associated with incident bacterial vaginosis as defined by Gram stain.
References
Footnotes
Parts of this study were presented at the British Association for Sexual Health and HIV – American Sexually Transmitted Diseases Association 3rd Joint Conference, 7–10 May 2008, Brooklyn, NY, Oral presentation # O-20 and The International Society for Sexually Transmitted Disease Research, 18th Biennial Congress, 28 June 28–1 July 2009, London, poster # P4.137
Funding This study was supported by NIH grants: K12-RR023250 (to RMB), UH2-AI083264 (to JR), R03-AI061131 (to JMZ) and K24-AI001633 (to JMZ).
Competing interests None.
Ethics approval This study was conducted with the approval of the Johns Hopkins School of Medicine, University of Maryland School of Medicine.
Provenance and peer review Not commissioned; not externally peer reviewed.