Article Text

Abstract
Background Identification of STI risk groups is essential for optimal prevention and medical care. Until now, swingers—that is, heterosexual couples who are practising mate swapping, group sex, visit sex clubs for couples, are not considered as a specific risk group for STI in healthcare services and prevention.
Objective To compare STI prevalence rates in swingers with that in other risk groups.
Methods At the STI clinic, South Limburg, The Netherlands, whether an attendee is a swinger has been systematically registered since 2007. STI clinic surveillance data were analysed to assess the swingers' share of consultations and STI diagnoses—here Chlamydia trachomatis (CT) and/or Neisseria gonorrhoea (NG).
Results Of 8971 consultations, 12% comprised swingers (median age 43 years, IQR 38–48). Overall, STI prevalence was highest in youth, men who have sex with men (MSM) and swingers. Older swingers had a CT prevalence of 10% and an NG prevalence of 4%. The share in STI diagnoses in the older age group (>45 years) comprised 55% for swingers and 31% for MSM.
Conclusions Swingers comprise a substantial proportion of STI consultations. They are a mainly older age group and form an important part of STI diagnoses. While other risk groups for STI, such as young heterosexuals and MSM, are systematically identified at STI healthcare facilities and provided with appropriate services, this is generally not the case for swingers. Swingers, like other groups with risk behaviours, need to be identified and treated as a risk group in STI prevention and care.
- Epidemiology
- heterosexuals
- risk behaviours
- STI control
- surveillance
Statistics from Altmetric.com
Introduction
The economic benefits of STI programmes can be improved by effectively targeting the groups at risk.1 Therefore, continuous evaluation and identification of such groups is essential. Gains are highest when targeting those groups who most fuel the STI epidemic—that is, sexual networks characterised by frequent partner change, concurrent partners and less contact with the healthcare system.2 3
Until now, swingers—that is, heterosexuals whom as a couple practise mate swapping, group sex, visit sex clubs for couples, are (inter) nationally not considered as a risk group for STI in healthcare services and prevention. However, since swingers meet people in places typed by multiple sex partners, concurrent partnerships and risk behaviour practices4–8 —that is, structures enabling quick spread of STI, swingers are a likely target for STI prevention and care. By dealing with them properly, more tailored prevention and enhanced STI screening is likely to produce gains on an individual and population (reduced STI burden) and economic (costs) level.
At our STI clinic, we started in 2007 to systematically register whether an attendee was a swinger. Here, we present surveillance data comparing STI prevalence among swingers, classic high-risk and lower-risk STI groups.
Methods
The outpatient STI clinic of the South Limburg Public Health Service offers a free examination and treatment for STI. The clinic is spread over South Limburg (population 0.63 million) with three locations. At every new consultation, attendees are tested for Chlamydia trachomatis (CT) and Neisseria gonorrhoea (NG) on first-void urine (men) and self swab (women and men) by commercially available nucleic acid amplification tests (NAAT, SDA, Becton Dickinson ProbeTec ET system, Maryland, USA or PCR, Roche Cobas Amplicor, California, USA). Blood is tested on Treponema pallidum, hepatitis B (HbsAg and anti-HBc, AXSYM, Abbott, Chicago, USA) and HIV (anti-HIV (1/2), Axsym; Abbott, Chicago, USA; reactive samples are confirmed by western blot, HIVblot 2.2, Genelabs Diagnostics, Sciencepark, Singapore). Clients comprise people with and without symptoms, including those attending after partner notification. A client is registered as swinger when he or she identifies as heterosexual and as a couple has sex with other heterosexuals.
For statistical analyses, the variable risk category was compiled hierarchically, with non-overlapping categories, from heterosexual, female prostitute and men who have sex with men (MSM) to swinger. We here analyse STI clinic surveillance data from January 2007 through December 2008, South Limburg, The Netherlands to assess STI prevalence and share in STI diagnoses of the risk groups and age categories. For the current analyses, STI is defined as a positive CT and/or NG diagnosis. We did not focus on syphilis, hepatitis B or HIV because of low number of positive diagnoses overall. Univariate and multivariate logistic regression analyses are used to assess nationality, risk category, age (and their interaction), as predictors for STI. We considered a p value <0.05 as statistically significant. Analyses were performed with the SPSS package version 14.0.2 (SPSS Inc).
Results
Of 8965 consultations, 89.1% of attendees were Dutch, 1.6% German and 4.2% Belgian; 11.7% were aged >45 years, 15.5% were aged between 35 and 45, 60% between 20 and 35 and 12.8% between 16 and 20 years. Overall, 11.6% of consultations comprised swingers (median age 43 years (interquartile range (IQR) 38–48)), 74.8% heterosexuals (median age 24 (IQR 21–29)), 9.6% MSM (median age 32 (IQR 23–46)) and 4% female prostitutes (median age 35 (IQR 28–44)).
The prevalence of CT, NG and CT and NG combined was 9.7%, 0.6% and 10.1%, respectively, in heterosexuals; 10.2%, 6.3% and 14.2% in MSM; 4.2%, 0.8% and 4.8% in female prostitutes; and 6.4%, 4.3% and 10.4% in swingers.
STI prevalence was not associated with nationality, but was associated with age and risk group (both p<0.001). Resulting multivariate modelling including age, group and their interaction (p<0.001) STI prevalence showed a distinct pattern by age and by risk group (table 1): with older age STI prevalence decreased in heterosexuals and increased in swingers (both p<0.001) while remaining stable among MSM and prostitutes. In clinic attendees aged >45 years, a higher STI prevalence was observed in swingers (13.7%) and MSM (14.6%) than in heterosexuals (2.9%) or prostitutes (2.9%). This was the case for both men and women (table 1). Older female swingers had the highest prevalence, even when compared with older male swingers (p=0.032).
Proportion of Chlamydia trachomatis and/or Neisseria gonorrhoea positive test results and risk estimates by age, risk category and gender following multivariate modelling, South Limburg Public Health STI clinic, 2007 and 2008
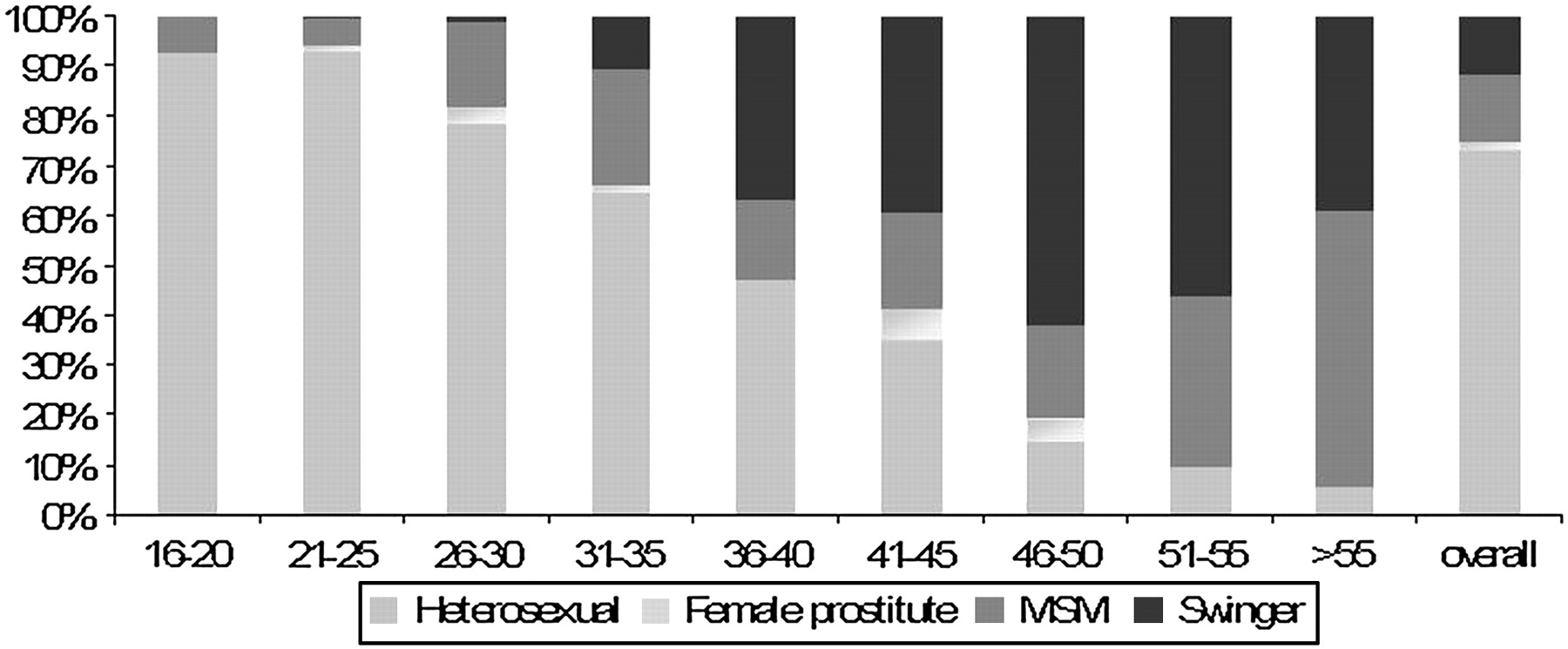
We further evaluated the relative share in STI diagnoses by age and risk categories. Figure 1 shows that in the youngest age groups, heterosexuals contributed the largest proportion of STI diagnoses. In the older age groups, STI was mostly diagnosed in swingers and MSM. The share in STI diagnoses for swingers and MSM increased with age (both p<0.001), reaching 55% for swingers and 31% for MSM in clients with STI who were aged >45 years. Combining all age groups, swingers comprised 12% of STI diagnoses (versus MSM 13%).

{kind=link}
Share of risk categories in positive Chlamydia trachomatis and/or Neisseria gonorrhoea diagnoses by age-group, South Limburg Public Health STI clinic, 2007 and 2008. MSM, men who have sex with men.
Discussion
We confirm previous UK observations suggesting that older STI clinic attendees are a notable proportion of the STI clinic population.9 Here, we add that swingers are a generally missed target for STI services. To our knowledge, no systematic data on STI diagnoses in these heterosexuals exist except for the data we present here from our regional STI clinic showing that swingers contribute considerably to STI consultations and STI diagnoses. They have high STI prevalence, especially the older aged clients. The number of STI consultations and STI diagnoses for swingers is comparable to those of the classic risk group of MSM.
Although exact estimates are unavailable, the swingers' population is probably large. One of the largest dating websites for swingers (Swingers Date Club; http://www.sdc.com) estimates that there are millions of swingers world wide; in the Netherlands 15 000 couples (30 000 individuals) have a profile on this website.10 The total number of swingers is probably larger. In the Netherlands, awareness that swingers are a risk group is growing, however slowly. The Dutch Ministry recently set up a method to register them in national STI surveillance. However, so far its national implementation is limited (in 51% of consultations it is not registered), showing 3296 consultations by swingers in 2008 (personal communication, F. Koedijk, RIVM, 2009). Swingers are probably not properly identified by STI care services; it is also possible that swingers are not optimally attending for STI care. (Inter)national data on STI care-seeking behaviour or STI rates of swingers are lacking. To our knowledge, no single country mentions swingers as a special focus group in national STI prevention. In 1986 the Centres for Disease Control reported that two female swingers were infected with HIV in a club (New York Times, 14 November 1986). Some outdated studies mention the fear of AIDS or STI among swingers4 but none were followed by more medical or scientific attention for swingers and STI.
Swingers differ from non-swinging heterosexual adults by their sexual network, typed by concurrent sexual partners and high rate of unprotected sex.4–8 These risk behaviours make swingers more prone to STI3 as confirmed by our study. Potentially, they may act as an STI transmission bridge to the entire population. By identifying and testing swingers (regularly) for STI, the individual and population burden of STI as well as the spread of STI can be reduced. Yet, (inter)nationally, swingers are under-represented in the STI services population.
Key messages
Swingers are a hidden risk group who need to be monitored in STI prevention and care services.
Identification of high-risk groups is essential for effective STI control.
Older STI clinic clients should not be overlooked as a potential risk group in STI care services.
Acknowledgments
The authors thank the staff of the STI clinic.
Footnotes
This paper has, in part, been presented at the 18th ISSTDR in conjunction with BASHH Congress in London, 28 June—1 July 2009 (P3.143).
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Whistlestop tour