Article Text

Abstract
Objectives Australian guidelines recommend annual testing for HIV and sexually transmitted infections (STIs) for all men who have sex with men (MSM) and 3–6 monthly testing for those at higher risk as defined by behavioural criteria. We assessed HIV/STI re-testing rates among MSM attending primary care clinics.
Methods We conducted a retrospective follow-up of HIV negative MSM tested for HIV or STIs (chlamydia or syphilis) at four primary care clinics in the 9-month period: April to December 2006. Re-testing rates for these infections were calculated over 18 months. Logistic regression was undertaken to identify predictors of guideline adherence.
Results Of the MSM requiring annual HIV testing according to the guidelines, the re-testing rates at 1 y were 35% (762/2163). Among the higher risk MSM, 6-monthly HIV re-testing rates were 15% (283/1862). Within the subgroup who reported 11 or more male sexual partners within the past 6 months, HIV re-testing rates within 6 months were 19%. Independent predictors of HIV re-testing within 6 months in higher-risk MSM were reporting 11 or more male sexual partners in the last 6 months (AOR 3.1, 95% CI 1.8 to 4.8); being born overseas (AOR 2.0, 95% CI 1.2 to 3.4); and previous HIV testing more than 12 months earlier (AOR 3.3, 95% CI 1.9 to 5.5).
Conclusion There is poor adherence to national guidelines that recommend regular re-testing of MSM for STIs, particularly among those at higher risk who require more frequent testing. Clinical strategies are urgently needed to encourage more frequent HIV/STI testing among MSM, especially in the higher risk subgroup.
- Health serv research
- HIV
- primary care
- sexual health
- testing
Statistics from Altmetric.com
Introduction
HIV diagnoses in Australia have been concentrated among men who have sex with men (MSM) since the epidemic began over 25 y ago. After a long decline, HIV diagnosis rates in MSM began increasing 10 y ago almost certainly reflecting a rise in incidence.1 In parallel, there has been a resurgence of syphilis among MSM in Australia2 accompanied by increasing chlamydia and gonorrhoea rates.3
Regular testing for HIV and other sexually transmitted infections (STIs) is recognised as a key control strategy. The curable bacterial STIs are often asymptomatic and can be transmitted unknowingly if left undiagnosed.4 Early diagnosis of HIV presents an opportunity to provide preventive counselling, as well as treatment to reduce viral load if clinically warranted. A recent meta-analysis showed the prevalence of high-risk sexual behaviour is reduced substantially after people became aware that they had HIV infection.5
In Australia, clinical guidelines recommend HIV and STI testing at least once a year for all men who have had any sex with another man in the previous year.6 More frequent testing is recommended for men reporting designated high-risk behaviours (multiple partners, attending sex-on-premises venues (SOPV), use of recreational drugs or seeking partners via the internet), or following the diagnosis of chlamydia or gonorrhoea.6 Despite these recommendations, there is no information available in Australia to assess how frequently MSM test for HIV and STIs in a clinical setting.
We assessed the extent and predictors of adherence to clinical guidelines for repeat testing through analysis of 27 months of data collected from a network of primary care sites involved in sentinel surveillance.
Methods
The Victorian Primary Care Network for Sentinel Surveillance (VPCNSS) of STIs and blood borne viruses (BBVs) was established in April 2006. Analyses reported in this paper were based on tests for HIV and other STIs (chlamydia and syphilis) that took place at four of the Melbourne-based clinics in the network. Three of these clinics were general practices (GPs) with a high-case load of MSM clients and the fourth was a large, publicly funded sexual health clinic (SHC). Together these clinics contributed nearly half of HIV diagnoses in Victoria among MSM annually. The VPCNSS was not funded to collate information about gonorrhoea testing and outcomes.
A data collection form was used at GP clinics to collect demographic, behavioural and testing information. Six month timeframes were used for sexual behaviour questions to be consistent with other behavioural research in Australia and other international guidelines for behavioural surveillance.7–9 The top section of the form served as a pathology request slip, contained a unique surveillance number and was completed for all HIV negative individuals undergoing HIV testing with or without accompanying STI testing. Men who gave a history of male to male sex were asked to complete the bottom section that comprised risk behaviour questions. Completion was voluntary and implied consent to participate.
The SHC used a computerised medical records system to collect sexual risk behaviour information as part of pre-testing risk assessment. The questions were slightly less detailed and used 12 month timeframes.
Testing for HIV and STIs was undertaken by each site′s routine pathology provider.
The Burnet Institute acted as coordinating unit for the system. Completed questionnaires from GPs were scanned and along with electronic risk behaviour data from SHCs were electronically linked with HIV and STI testing data using automated matching strategies.
The project was approved by seven Human Research Ethics Committees.
Analyses
Adherence to testing guidelines
We assessed adherence to the sexually transmitted infection testing guidelines for MSM that were promulgated in 2005 and revised in 2008. These guidelines include three recommendations (see box 1).
Box 1 Sexually transmitted infection (STI) testing guidelines for men who have sex with men (MSM), 20056
Recommendation 1: any risk MSM
With or without symptoms, all men who have had any sex with another man in the previous year should be offered tests for STIs at least once a year in the following way:
Pharyngeal swab for gonorrhoea culture
Anal swab for gonorrhoea culture/NAAT* and chlamydia NAAT
First catch urine for chlamydia NAAT
Serology for HIV
Serology (including a Treponema pallidum haemagglutination assay, Treponema pallidum particle agglutination test or enzyme immunoassay test) for syphilis
Recommendation 2: higher risk MSM
3–6 monthly testing including men who have multiple partners.** Indicators may be: attending sex-on-premises-venues (SOPVs), use of recreational drugs or seeking partners via the internet
Recommendation 3
People diagnosed with chlamydia or gonorrhoea should be retested in 3 months.
↵* NAAT=nucleic acid amplification test.
↵** The guidelines were revised in 2008 to define higher risk as also including having 11 or more partners in the last 6 months or at least one episode of unprotected anal sex. The full 2008 guidelines are available at http://www.stigma.net.au/resources/STIGMA_MSM_Guidelines_RACGP_updated_Feb_09.pdf
The analyses were conducted separately for the GP clinics and SHC.
Adherence to recommendation 1 and 2
The entire timeframe under analysis was 1 April 2006 to 30 June 2008. HIV negative MSM seen at participating sites who had their first HIV or STI test between 1 April and 31 December 2006 (baseline) were followed over time until June 2008 to assess if they were tested again at a participating clinic. Only men from whom behavioural information was available at the time of the testing visit during this period were included.
MSM were excluded from all analyses if they reported current sex work, were HIV positive or tested positive during the analysis period. The analyses also excluded HIV testing that was conducted as a component of routine HIV post exposure prophylaxis (PEP) management10 11; or as a second test within 60 days of the first test as it was likely to reflect window period testing in response to a recent high-risk exposure.
Based on self-reported risk behaviour at baseline, men were classified as ‘any risk’ (recommendation 1: annual testing indicated) or ‘higher risk’ (recommendation 2: 3–6 monthly testing indicated). These definitions varied between the GP and SHC based on slight differences in the sexual behaviour information collected.
At the GP clinics, men who reported sex with another man in the last 6 months were classified as ‘any risk’. ‘Higher risk’ MSM were those who reported two or more male anal or oral sexual partners in the past 6 months, attending SOPVs or using the internet to meet sexual partners in the last 6 months or unprotected anal sex in the past 6 months.
At the SHC, men who reported sex with another man in the last year were classified as ‘any risk’. ‘Higher risk’ MSM were those men who reported two or more male sexual partners in the past 12 months or unprotected anal sex with male sexual partners (UAIC) in the last year.
We also separately assessed adherence in each of these behavioural categories as well as 11 or more sexual partners (based on revised 2008 guideline's definition of higher risk).
The proportion returning for testing at 3 month intervals was calculated as; 3 months (61–90 days since their first), 6 months (61–180 days), 9 months (61–270 days), 12 months (61–360 days) and 18 months (61–540 days). Additional testing beyond the second test was not included in the analysis.
Adherence to recommendation 3
MSM diagnosed with chlamydia (whether at single or multiple anatomical sites) in the period April 2006 to December 2007 were followed for a 6-month period post diagnosis and the proportions returning for testing at 3 and 6 months calculated. HIV positive MSM and men who reported current sex work were excluded.
Predictors of adherence to repeat testing guidelines
Analysis of predictors of adherence was restricted to MSM attending the GP clinics as detailed sexual behaviour was not collected by the SHC.
Univariate and multivariate logistic regression analyses were undertaken to identify factors independently associated with recommendations 1 and 2 using backwards elimination. Goodness of fit was assessed using the Hosmer-Lemeshow test.
For recommendation 2, 11 or more sexual partners was used as the basis for the multiple partner criteria. This definition was based on findings from the Health in Men Study, which showed that having 11 or more casual partners in the past 6 months was an independent risk factor for urethral and anal chlamydia and gonorrhoea infections in HIV negative MSM.12 It was not formally used in the 2005 guidelines but incorporated explicitly in the 2008 guidelines.
OR and 95% CIs were calculated for these associations. A cut-off of p<0.05 was used for all statistical tests. Stata statistical software v9 was used to conduct all analyses.13
Results
Adherence to testing guidelines
Recommendation 1: annual testing indicated
At the GP clinics, 1063 MSM reporting any risk were tested for HIV during the baseline period, 844 were tested for chlamydia and 1028 for syphilis (figure 1). Of those tested as baseline, 37% MSM returned for another HIV test in 12 months. At the SHC, 1100 MSM reporting any risk were tested for HIV during the baseline period, 1184 for chlamydia and 1280 for syphilis. Of those tested at baseline, 33.6% returned for another HIV test in 12 months (figure 2). Similar annual re-testing rates were found for chlamydia and syphilis in both clinical settings.
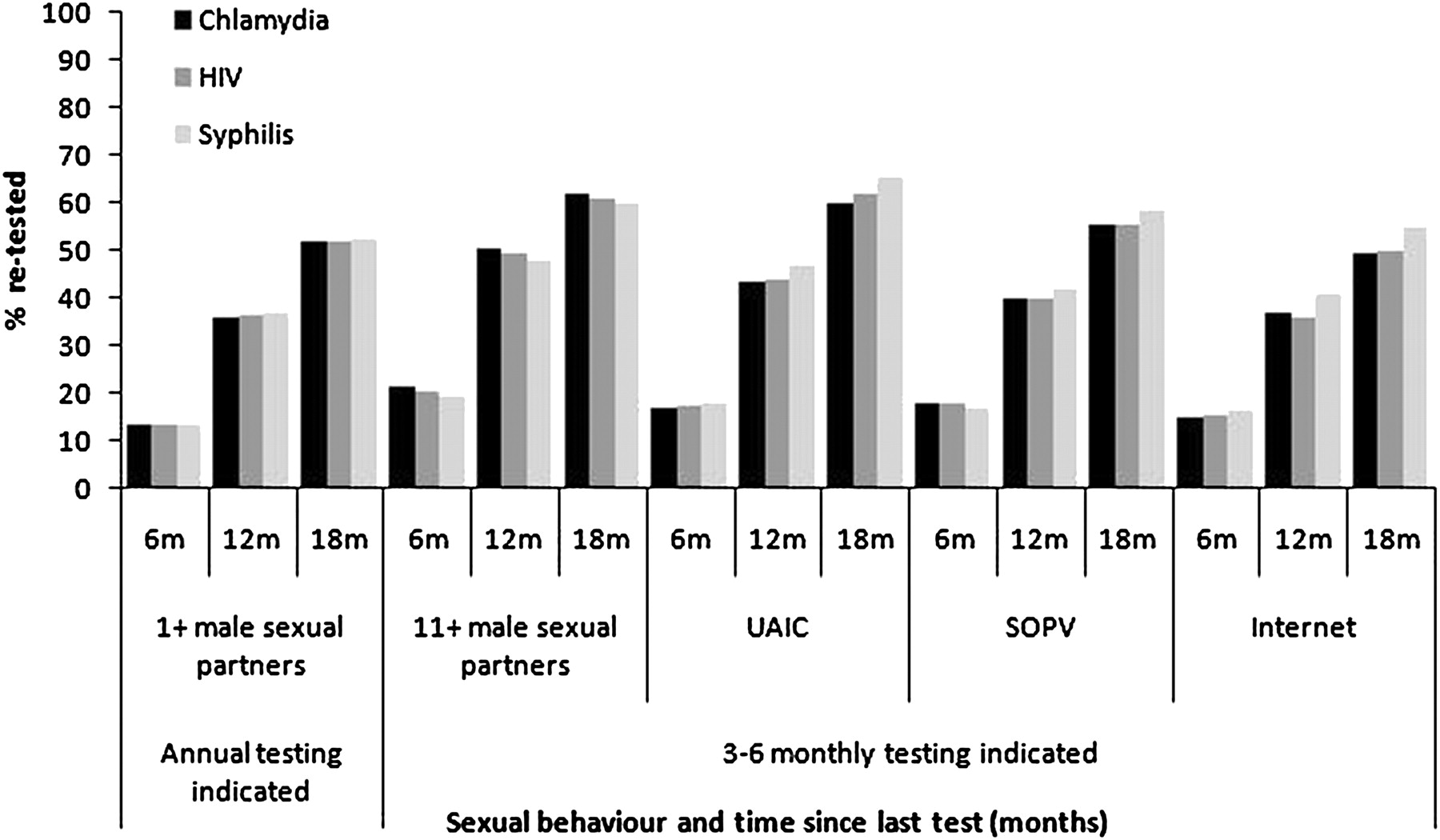
Adherence to recommendation 1 (annual testing indicated) and recommendation 2 (3–6 monthly testing indicated), MSM, April 2006 to June 2008, GP clinics. All behavioural characteristics relate to the past 6 months. GP, general practice; m, months; MSM, men who have sex with men; SHCs, sexual health clinics; SOPV, meeting sexual partners at sex-on-premises-venues (SOPVs); internet, meeting sexual partners on the internet; UAIC, unprotected anal intercourse with casual partners.

{kind=link}
{kind=link}
Adherence to recommendation 1 (annual testing indicated) and recommendation 2 (3–6 monthly testing indicated), MSM, April 2006 to June 2008, sexual health clinics. Number of partners relate to the past 12 months. m, months; MSM, men who have sex with men; SHCs, sexual health clinics; UAI, unprotected sex with male partners.
Recommendation 2: 3–6 monthly testing indicated
At the GP clinics, 902 of 1063 (85%) MSM tested for HIV were classified as higher risk. Of these MSM, 14.6% returned for another HIV test in 6 months (figure 1, table 1). Similar 6-month re-testing rates were found for chlamydia and syphilis.
Predictors of adherence with testing for any risk MSM* April 2006 to June 2008, GP clinics
At the GP clinics, the 6-month HIV re-testing rates increased with increasing number of male sexual partners reported, from 15% among those with two or more partners in the last 6 months to 21% in MSM reporting 11 or more partners in the past 6 months. Among MSM reporting meeting sexual partners at SOPVs and UAIC in the last 6 months, HIV re-testing rates were slightly lower at 18% each. Of the MSM who reported seeking sexual partners on the internet, 15% returned for another HIV test in 6 months. Similar 6-month re-testing rates were seen for chlamydia and syphilis (figure 1).
At the SHC, 960 (87%) MSM were classified as higher risk and 16% returned for another HIV test in 6 months. Of the 409 MSM who reported 11 or more male sexual partners in the past 12 months, 18% returned for another HIV test in 6 months compared to 16% among those reporting two or more partners. Similar 6-month re-testing rate were seen for chlamydia but lower re-testing rates were seen for syphilis (figure 2).
Recommendation 3: 3 month test for re-infection indicated
At the GP clinics, 65 MSM were diagnosed with a chlamydia infection between April 2006 and December 2007 and 9% returned for chlamydia testing in 3 months and 18% in 6 months. At the SHC, 222 MSM were diagnosed with a chlamydia infection between April 2006 and December 2007 and 7% returned for another chlamydia test in 3 months and 23% in 6 months.
Predictors of adherence
In the multivariate analysis, HIV negative MSM attending the GP clinics who reported any risk behaviour were more likely to adhere with the recommendation to be tested annually if they reported UAIC in the past 6 months (AOR 1.74, 95% CI 1.3 to 2.40; p=0.001), reported a previous HIV test more than 12 months earlier (AOR 2.1, 95% CI 1.5 to 2.2; p<0.001) or reported meeting sexual partner/s at beats in the last 6 months (AOR 1.9, 95% CI 1.2 to 3.0; p=0.006) (table 1).
MSM were classified as higher risk, were more likely to adhere with the recommendation to be tested every 3–6 months if they reported 11 or more male sexual partners in the last 6 months (AOR 3.1, 95% CI 1.8 to 4.8; p<0.001), reported a previous HIV test more than 12 months earlier (AOR 3.3, 95% CI 1.9 to 5.5; p<0.001) or were born overseas (mainly Western Europe, Eastern Europe and Asia) (AOR 2.0, 95% CI 1.2 to 3.4; p=0.012) (table 2).
Predictors of adherence with testing for higher risk MSM*, April 2006 to June 2008, GP clinics
Discussion
As far as we can ascertain this is the first analysis of its kind that has made use of continually collected clinical information to assess the frequency of both repeat HIV and STI testing in MSM attending primary care clinics. We found that the rate of repeat testing is substantially lower than the level called for in national clinical guidelines.6 Despite recommendations for all MSM to be tested annually, less than 40% of MSM attending the clinics underwent repeat HIV, chlamydia or syphilis testing after 1 y at the same clinic. Furthermore, HIV and STI re-testing rates within 6 months for higher risk men were less than 20% and 3 month chlamydia re-testing rates following a positive diagnosis and treatment was less than 10%.
The public health significance of the guidelines was recently highlighted through mathematical modelling, which explored a range of interventions to reduce syphilis and HIV transmission among MSM in Australia. The model showed quarterly or 6-monthly testing, particularly among MSM with high numbers of sexual partners, would have a substantial impact compared to annual testing and other preventive interventions.14 15
The lower than recommended testing rates may be due to a number of factors. MSM may not return for repeat testing because they do not perceive testing as a priority or consider themselves at risk, or they may choose to get tested at another clinic. The 2003 Melbourne Gay Community Periodic Survey demonstrated that just over half (28/ 49) of HIV negative men recruited from one of the high-case load GP clinics reported their last STI testing was at a SHC.16
However, when MSM do attend the clinic there are likely to be missed clinical opportunities to offer testing. Clinicians may forget to offer testing, make interpretations of specific histories leading to individually tailored testing recommendations or the competing demands of other health issues may reduce the time available to offer or undergo HIV/STI testing or make it inappropriate to do so. A 2007 survey of clinicians in Victoria working in high-case load MSM clinics or SHCs found only 67% of clinicians offered chlamydia and gonorrhoea testing to HIV negative MSM annually and 73% offered syphilis testing annually.17
Our multivariate analysis showed that independent predictors of adherence to repeat testing among higher risk men were having a previous HIV test more than a year prior and being born overseas. It is not clear why this is so, but it is possible that patients who have not tested for more than a year but report high risk behaviour may receive more directive recommendations from their clinicians to undergo regular testing and patients born overseas, whose first language may not be English, may be more likely to adhere with recommendations made by their clinicians due to different health beliefs about the needs for screening and blood tests.
The analysis has a number of limitations. First, the clinic-based analysis reported here may have underestimated the re-testing rate as a proportion of men may have undergone testing at other sites. The annual HIV/STI re-testing rates are much lower than estimates reported from the Melbourne Gay Community Periodic Survey of 60–70% in the past few years.18 However, it possible that the this self-report based survey overestimated testing rates as MSM may have recalled testing over a longer period than a year sought in the survey. Second, the sentinel surveillance questionnaire used by the GP clinics had 6-month timeframes but the guidelines refer to 12 months, which could exclude some men from the lower or higher risk groups if the specific sexual behaviours occurred before the most recent 6-month period. This discrepancy could result in an over or underestimate of adherence rates, depending on the timing of the behaviours. Third, the clinics selected for the sentinel programme specialise in sexual health in MSM and may not be representative of primary care sites, but if anything they should have better adherence than the average primary care clinic. Fourth, the VPCNSS was not funded to collate information of gonorrhoea testing and outcomes. However, as testing for chlamydia and gonorrhoea are virtually always conducted simultaneously in MSN in Australia, the findings for gonorrhoea testing uptake could be expected to be virtually identical to those for chlamydia.
A combination of strategies may be needed to encourage a change in screening behaviour among clinicians and patients. Electronic medical alerts in patient management systems that remind clinicians of the guidelines related to sexual health testing in MSM has been shown to be successful in improving sexual health service delivery.19 SMS, also known as text messaging, has been shown to be an effective method of communicating appointment reminders and reducing ‘missed’ appointments in clinical settings.20 21 Specialised websites allow MSM to set up reminders for themselves to seek sexual health testing at regular time periods.22 Other clinical strategies could include incentives to screen.23 Health promotion campaigns or other strategies focused on more frequent testing among all MSM or those at high risk should also be considered. Although the effects of social marketing campaigns are generally short lived,24 they can be coupled with other strategies, like SMS reminders, which reinforce the health promotion messages.
The results of this analysis demonstrate poor adherence to national guidelines that recommend regular HIV/STI testing among MSM, with a particular emphasis on those at higher risk who require more frequent testing. Improved strategies are urgently needed to ensure a higher level of adherence to these recommendations by MSM and the services that they access.
Key messages
Despite national recommendations, re-testing rates for HIV/STIs after 1 y were less than 40% among men who have sex with men (MSM) attending primary care clinics.
HIV and STI re-testing rates within 6 months were less than 20% for higher risk MSM.
Three month chlamydia re-testing rates was less than 10% for MSM previously diagnosed with chlamydia.
Improved strategies are urgently needed to ensure a higher level of adherence to these recommendations by MSM and the services that they access.
References
Footnotes
Competing interests None.
Ethics approval This study was conducted with the approval of the Department of Human Services, Victoria, Australia.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Whistlestop tour