Article Text

Abstract
Objective To determine the characteristics of general practitioners (GPs) who test and patients who are tested for HIV in Australia.
Design and Setting A secondary analysis of data from the Bettering the Evaluation and Care of Health programme; a cross-sectional, national survey of GP activity.
Methods We identified GP, patient and encounter characteristics that were associated with HIV testing between April 2000 and March 2010. We looked at testing rates for patients with different characteristics, whether they had attended for screening and GP ‘risk factor’ identification. Multiple logistic regression was used to measure the independent effect of each GP, patient and encounter characteristic on testing for HIV.
Results Data were available for 984 200 encounters from 9842 GPs. 1796 (18.2%) of GPs performed at least one HIV test. On logistic regression, independent predictors of HIV testing included the management of a ‘risk factor’ (OR 19.4, 95% CI 17.4 to 21.6), screening (OR 10.6, 95% CI 9.4 to 12.1), younger GP age, practice in a metropolitan area (OR 1.4, 95% CI 1.2 to 1.6), patient age, gender (male > female OR 3.0, 95% CI 2.7 to 3.3), being new to that practice (OR 2.1, 95% CI 1.8 to 2.3) and being Indigenous (OR 1.7, 95% CI 1.3 to 2.4).
Conclusion The most significant independent predictors of testing were identification of a risk factor and attendance for screening. Unless barriers to testing are addressed it is unlikely that altering guidelines alone will improve testing rates and reduce transmission.
- HIV testing
- general practice
- primary care
- HIV screening
- barriers to HIV screening
Statistics from Altmetric.com
Introduction
The annual number of new HIV diagnoses in Australia has steadily increased over the past 9 years from 763 cases in 2000 to 1050 in 2009; many of those who are newly diagnosed were infected in the year prior to diagnosis suggesting that new infections continue to occur despite public health initiatives.1 A similar rise in the annual number of new HIV diagnosis has been reported from other developed countries.2 3 There is a growing acknowledgement that the HIV testing needs to be normalised and its diagnosis considered a task for all medical practitioners even if subsequent management may need to be supervised by specialists.4 5 Screening for HIV has a number of advantages, including reducing morbidity and mortality, and reducing the risk of onward spread through counselling, antiretroviral treatment and provision of condoms and safe injecting equipment. A universal offer of HIV testing is estimated to be cost-effective where the diagnostic rate of HIV is greater than 1 per 1000.6 Recommendations about who should be tested vary from country to country. Australia has a voluntary counselling and testing programme. Some of those recommended for testing include individuals who have had unprotected male to male intercourse; have shared injecting equipment; have been the sexual partner of an HIV positive person; being from a country with a high HIV prevalence; are pregnant and have a diagnosed sexually transmissible infection (STI). Undiagnosed HIV infection is an important reservoir for onward transmission and in Australia it is estimated that about 9% of HIV infected men who have sex with men (MSM) are undiagnosed.7 In the UK, an estimated 86 500 people were living with HIV at the end of 2009, of whom a quarter were unaware of their infection and half of the newly diagnosed adults with HIV were diagnosed late.2 This has prompted a push for more HIV testing in the UK and the guidelines state that where the prevalence of diagnosed HIV infections is greater than 2 in 1000, HIV tests should be offered to all individuals aged 15–59 years registering in general practice as well as to all general medical admissions.8 9 In the USA, The Centres for Disease Control and Prevention (CDC) now recommends that HIV screening be performed routinely in all healthcare settings for 13–64 year olds.10
General practice provides opportunities for diagnosing HIV infection in individuals who may be at risk of acquiring the infection and also in those who present with symptoms and signs that may suggest infection. General practitioners (GPs) are also ideally placed to educate people about risk factors for HIV and how to reduce these risks. Increasing the uptake of HIV testing in general practice has individual and public health benefits. The 2010–2013 National HIV/AIDS strategy in Australia identified GPs as having a key role in diagnosis and prevention of HIV as the majority of testing and treatment of STIs in Australia is believed to occur in general practice.11
In Australia, GPs are the gatekeepers to the healthcare system and about 85% of the population attends a general practice in a given year. Remuneration is on a fee for service basis, but most costs are paid by the Australian government under a universal health insurance scheme.12 Although there is now some information about diagnosis and treatment of STIs in general practice in Australia 13–15 there is little information on HIV testing.
Bettering the Evaluation and Care of Health (BEACH) is an ongoing, cross-sectional, encounter-based survey of general practice activity throughout Australia. We undertook a study using the BEACH database to determine HIV testing patterns of GPs, to determine the GP, patient and encounter characteristics associated with testing.
Methods
The BEACH database
The BEACH programme is a continuous, paper-based, national study of general practice activity in Australia. Sampling and methods have been described in detail elsewhere.16 In summary, each year approximately 1000 GPs from a national, rolling random sample (drawn by the Australian Government Department of Health and Ageing from general practice claims data under a universal health insurance scheme) participate in BEACH. Each GP provides patient demographics and encounter information for 100 consecutive encounters with consenting, unidentified patients. Each annual dataset is weighted for GP activity level and for an identified under-representation of younger GPs. The annual weighted BEACH encounter samples have repeatedly been demonstrated to be representative of all encounters claimed through the universal insurance system.16
Information recorded at encounter includes patient age; gender; whether they are Indigenous people (patient self-report); whether they are from a non-English speaking background (self report); whether they are a new patient; up to three patient reasons for encounter and up to four problems managed at the encounter (recorded by GP as diagnoses or as problem descriptions). ‘Problem managed’ describes the GPs view of the problem managed at the highest diagnostic level possible with the evidence available at the time. Problems managed were classified according to the International Classification of Primary Care (version 2) (ICPC-2)17 and coded more specifically with ICPC-2 Plus18—an Australian GP interface terminology classified to ICPC-2. Opportunity to test was further grouped under two separate types: ‘screening’ and ‘at risk’. The ‘screening’ labels included all problems described by the GP as ‘check-up’ (A30007, A31012), ‘medical exam’ (A30013, A31013), ‘health screening’ (A31008), ‘blood test’ (A34001), ‘disease screen’ (A38005), ‘test results’ (A60001), ‘antenatal check-up’ (W30006) or ‘confirmed pregnancy’ (W78002). The ‘at risk’ labels included ‘contact with sexually transmitted disease (STD)’ (A23001), ‘risk factor of disease’ (A23003), ‘exposure to disease’ (A23008), ‘unprotected sex’ (A23011 and A23012), ‘test for STI’ (A33010 and A33057), ‘STD’ (A78011), HIV/AIDS (the whole of ICPC-2 code B90), ‘fear of HIV/AIDs’ (the whole of B25), ‘HIV/AIDS test’ (B33006 and B33008), ‘hepatitis C’ (D72008), ‘needle stick injury’ (S19003), ‘drug abuse’ (P19) and genital problems (X,Y).
GP-related data elements include age, gender, years in practice, country of graduation, sessions worked per week, proportion of encounters not conducted in English, size of practice, postcode of practice, Fellowship of the Royal Australian College of General Practitioners (FRACGP) status (yes/no) and practice accreditation status (yes/no). Practice postcode was used to define major cities using the Australian Standard Geographical Classification.19
This study investigated BEACH data collected during the 10-year period: April 2000 to March 2010 inclusive. We identified all participating GPs who had requested at least one HIV test during their 100 recorded encounters and investigated the relationship between testing behaviour, GP characteristics and patient characteristics.
Statistical methods
We used conventional, simple random sample methods for GP-based comparisons. The sample of encounters was a cluster-based sample, with the cluster around the GP, so we adjusted the 95% CIs reported for the single stage clustered study design using procedures in SAS version 9.1.3.20 Weighted data were used for analysis on individual years; unweighted data were used when the datasets were combined across years.
Percentages are used to describe the characteristics of all GPs in the BEACH sample, of those who performed at least one HIV test in their 100 encounters and characteristics of patients at all BEACH encounters and for at those encounters where a HIV test was ordered. HIV testing rates per 1000 encounters are reported for each GP and patient characteristic. Statistical significance of differences is judged by non-overlapping 95% CIs.
Multiple logistic regression was used to measure the independent effect of each patient, GP and encounter characteristic on testing for HIV. Those characteristics that were statistically significant at the univariate level were considered. The GP variable ‘years in practice’ was excluded as this is highly correlated with GP age.21 Consequently, the variables included in the regression analysis were GP gender, age group, country of graduation (Australia/elsewhere), practice location (major city/elsewhere), sessions worked per week, practice size, FRACGP status, practice accreditation status; patient gender, age group, Indigenous status, status to the practice (new/seen previously); year of data collection and ‘opportunity to test’. ‘Opportunity to test’ was defined as the presence at encounter of problem labels, strongly associated with GP requests for HIV tests, and included both ‘at risk’ and ‘screening’ labels. Backwards elimination was used to achieve a parsimonious model (ie, where all variables add significantly to the overall model).
Results
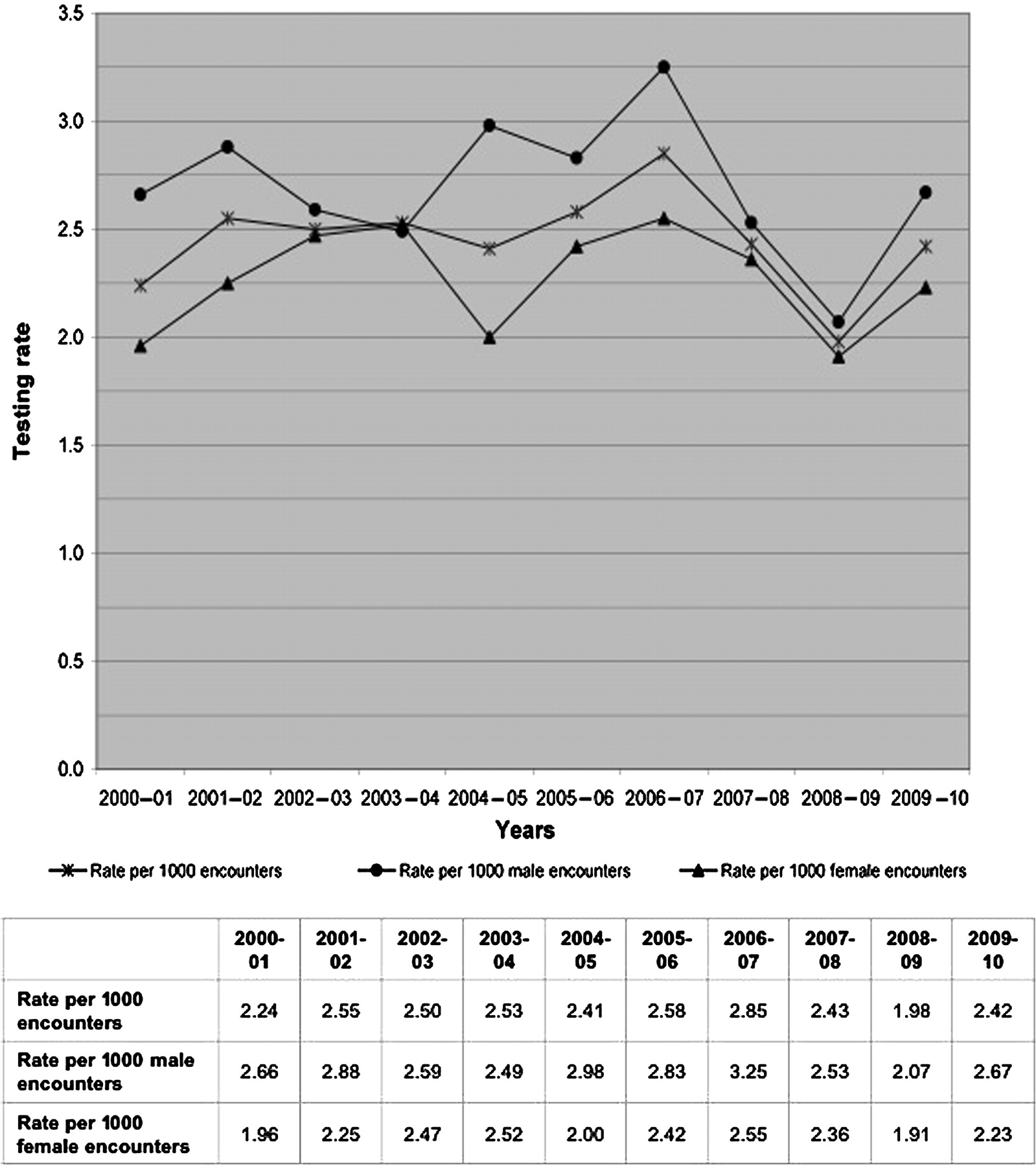
Data were available for 984 200 encounters from 9842 GPs. Of these, 2588 (2.6, 95% CI 2.5 to 2.8, per 1000 encounters) from 1796 GPs (18.2% of the participating GPs) included a HIV test (HIV test encounters). Figure 1 shows the annual order rates of HIV tests from 2000–2001 to 2009–2010. Testing rates did not significantly change across the decade.
{kind=link}
Rate of HIV testing in Australia 2000–2010.
Characteristics of patients being tested for HIV
Table 1 shows the demographic characteristics of patients who were tested for HIV compared to patients at all BEACH encounters. The far right column provides the test rate per 1000 encounters for each characteristic. More than half the tests were taken from individuals aged 25–44 years and 30.0% from those aged 15–24 years. Altogether, 44% of the HIV test encounters were with men and 56% with women. The likelihood of being tested was significantly higher at encounters with patients aged 15–24 years (8.5 per 1000) followed by 25–44 years (5.9 per 1000). In addition, testing rates were higher among Aboriginal people (5.6 per 1000), among those new to the practice (6.8 per 1000) and where there was an opportunity to test (17.8 per 1000).
Characteristics of patients at all BEACH encounters and of those at HIV test encounters with rate of HIV tests per 1000 encounters
Characteristics of GPs requesting HIV tests
The GPs more likely to test for HIV at one or more of their 100 patient encounters were women; younger; those working in a group practice; those practising in a metropolitan area; those working only a few sessions a week; those who graduated in Australia; those who conducted less than 50% of their consultations in a language other than English and those working in an accredited practice (table 2).
Likelihood of at least one HIV test, and order rate per 1000 encounters, by general practitioner (GP) characteristics
Multiple logistic regression
We conducted two logistic regression models (table 3). The first model adjusted for all variables that were significant in univariate analysis except for ‘screening’ and ‘at risk’. This model showed that HIV testing was independently associated with several GP and patient characteristics. The GP characteristics were gender (women more likely to test than men; OR 1.40, 95% CI 1.25 to 1.58); younger age, especially those aged <35 years (OR 1.74, 95% CI 1.41 to 2.16) compared to those aged 55 years and older; working in major cities (OR 1.4, 95% CI, 1.24 to 1.59) compared to GPs from regional/remote areas; working in a large practice (OR 1.28, 95% CI 1.05 to 1.56) compared to solo GPs and working in an accredited practice (OR 1.31, 95% CI 1.1 to 1.5) compared to GPs not working in an accredited practice. Patient characteristics were gender (men being more likely to be tested than women; OR 1.49, 95% CI 1.35 to 1.64); age (patients aged 15–24 years being more likely to be tested compared to all other age groups; and Indigenous status, Indigenous patients being more likely to be tested (OR 2.03, 95% CI 1.50 to 2.77) compared to non-Indigenous patients. Finally, patients new to that GP practice were more likely to be tested compared to those seen previously (OR 1.92, 95% CI 1.71 to 2.16).
Logistic regression: the independent effect of general practioner (GP), patient and encounter characteristics on the chance of a HIV test being ordered
In the second model, ‘opportunity to test’ was added first as a single variable and then separated into ‘at risk’ and ‘screening’. All variables that were significant in the initial regression remained significant with the exception of GP gender and FRACGP status for which no differences remained after adjustment for opportunity to test. The other major difference between the two regression models was gender of the patient, with men three times more likely to have a HIV test done than women, after adjustment for opportunity to test. Opportunity to test ‘at risk’ was highly correlated with HIV testing (OR 19.4, 95% CI 17.39 to 21.57) as was opportunity to test ‘screening’ (OR 10.63, 95% CI 9.36 to 12.07).
Discussion
Testing rates for HIV in general practice in Australia did not significantly change between 2000–2001 and 2009–2010. By extrapolating the GP HIV order rate to the average 100 million annual patient/GP encounters in Australia between 2000–2001 and 2000–2010, we estimate that approximately 275 000 HIV tests were ordered annually by GPs in Australia (about 120 000 for male patients and just over 150 000 for female patients) during this period. HIV testing rates in primary care in the UK increased slowly but remained low in the decade to 2005.22 Testing rates in sexual health clinics have also remained steady.1 During the study period there were a number of social marketing initiatives directed at MSM but no programmes directed at the general public.
The strongest independent predictor of a HIV test being ordered was an opportunity to test when the patient presented for ‘screening’ or was considered to be ‘at risk’ by the GP. This suggests that GPs are making decisions based on a risk assessment or guidelines. The findings of this study imply that there are real barriers to GP testing for HIV when the problems managed at the encounter do not provide them with an opportunity to open discussion on HIV testing.
How much of the risk assessment was performed by the GP and how much was down to the patient revealing information about themselves is not known, but both are likely to be important. A study from New York showed that MSM who had revealed their sexuality to their healthcare worker were more likely to be tested for HIV than those who had not.23 However, in the USA, many providers are reluctant to discuss HIV risk behaviour24–26 and testing barriers for patients are a low perception of risk and fear of stigmatisation.27 Basing tests on screening guidelines, or a risk assessment based on gender, age, sexual history and previous STIs, can improve the yield of positive tests.28 29 However, basing the decision to test on the opportunity given by management of specific related problems may miss some ‘high risk’ individuals managed for unrelated morbidity. In addition, a study from 10 counties in Sub-Saharan Africa showed that although 70% of people said that they planned to be tested for HIV the actual proportion who were tested was much lower ranging from 24–64%.30
Other GP factors independently associated with testing were younger age, practise in a major city, working in a practice with five or more GPs and working in an accredited practice. This aligns with our previous findings that younger GPs who work in cities are more likely to manage patients with STIs and sexual health problems and to test patients for chlamydia13–15 and similar differences have been noted in relation to chlamydia testing in general practice from the USA.31 32
Patient characteristics independently associated with being tested include age between 15 and 24 years, being a new patient to that practice and being Indigenous. The observation that patients new to a practice are more likely to be screened suggests that some individuals may choose to attend a GP who is unknown to them to obtain an HIV test, highlighting that for some patients fear of stigmatisation maybe a major barrier to testing. A similar difference has been noted in relation to chlamydia testing.14 In the unadjusted logistic regression, men were 1.5 times more likely to be tested than women. However, after adjusting for opportunity to test, they were three times more likely to receive a HIV test than women suggesting that GPs are more likely to test a man even when they do not have a related problem. This may be due to the fact that men are recognised to be at an increased risk of HIV in Australia as the majority of new infections have been in MSM.
The strengths of this study are that BEACH is an encounter-based database reflecting what GPs actually do, the random nature of the GP sample—thus being representative of all GPs in Australia—and the large encounter sample with a small cluster effect. A limitation of our study is that our results only include GPs who ordered a ‘HIV test’. It does not include requests for a ‘STI screen’, which may include an HIV test, so the number of HIV tests being conducted as a result of GP encounters may be higher than our study suggests.
It is increasingly recognised that HIV testing needs to be offered in wider settings and general practice has an important role. There has been a change in the guidelines for HIV testing in the USA and UK10 33 to reflect this shift. However, even when HIV testing is considered as ‘routine’ and the recommendation is to test all or selected patients between 15 and 64 years of age, as in the USA, unless they ‘opt out’, barriers to implementation remain. These include inadequate clinician time, inadequate resources and concerns regarding provision of follow-up care.29 34–36 Unless all the barriers to testing are addressed and healthcare providers are given the opportunity to test, it is unlikely that altering guidelines alone will improve testing rates and reduce HIV transmission. Improved GP training may assist in the process.
Key messages
The strongest predictor for a general practitioner to test a patient for HIV was an opportunity to test when the patient presented for ‘screening’ or was considered to be ‘at risk’.
Even when HIV testing is considered as ‘routine’ barriers to implementation remain. These include inadequate clinician time and resources, and concerns regarding provision of follow-up care.
Unless barriers to testing are addressed it is unlikely that altering guidelines alone will improve testing rates and reduce HIV transmission.
Acknowledgments
We wish to thank the general practitioners who participated for their generosity. We thank the Australian Government Department of Health and Ageing for supply for Medicare claims data used for adjustments.
References
Footnotes
Funding During the data collection period of this substudy, the BEACH programme was funded by the Australian Government Department of Health and Ageing, the Australian Institute of Health and Welfare, National Prescribing Service Ltd, Abbott Australia, AstraZeneca Pty Ltd (Australia), Janssen-Cilag Pty Ltd, Merck, Sharp and Dohme (Australia) Pty Ltd, Pfizer Australia, Sanofi Aventis Australia Pty Ltd, Wyeth Australia Pty ltd, Roche Products, Aventis Pharma Pty Ltd, the Office of the Australian Safety and Compensation Council (Australian Government Department of Employment and Workplace Training) and the Australian Government Department of Veterans' Affairs.
Competing interests None declared.
Ethics approval BEACH data collection for this study was approved by the Human Research Ethics Committee of the University of Sydney and the Ethics Committee of the Australian Institute of Health and Welfare.
Provenance and peer review Not commissioned; externally peer reviewed.