Article Text

Abstract
Objectives Since 2003, US organisations have recommended universal screening, rather than targeted screening, of HIV-infected persons for gonorrhoea and chlamydia. The objective of this study was to determine whether wider testing resulting from these guidelines would produce an increase in gonorrhoea/chlamydia diagnoses.
Methods 3283 patients receiving HIV care in 1999–2007 in the Johns Hopkins Hospital HIV clinic were studied. The two primary outcomes were the occurrence of any gonorrhoea/chlamydia testing in each year of care and the occurrence of any positive result(s) in years of testing. The proportion of all patients in care who were diagnosed with gonorrhoea/chlamydia was defined as the number of patients with positive results divided by the number of patients in care. Trends were analysed with repeated measures logistic regression.
Results The proportion of patients tested for gonorrhoea/chlamydia increased steadily from 0.12 in 1999 to 0.33 in 2007 (OR per year for being tested 1.17, 95% CI 1.15 to 1.19). The proportion positive among those tested decreased significantly after 2003 (OR per year 0.67, 95% CI 0.55 to 0.81). The proportion of all patients in care diagnosed with gonorrhoea/chlamydia therefore remained generally stable in 1999–2007 (OR per year 0.97, 95% CI 0.91 to 1.04).
Conclusions Universal annual screening, as implemented, did not increase the proportion of all patients in care who were diagnosed with gonorrhoea/chlamydia. Similarly low implementation rates have been reported in cross-sectional studies. If future efforts to enhance implementation do not yield increases in diagnoses, then guidelines focusing on targeted screening of high-risk groups rather than universal screening may be warranted.
- Antiretroviral thera
- Chlamydia trachomatis
- cost-effectiveness
- guidelines
- health service research
- HIV
- HIV prevention
- infectious diseases
- Neisseria gonorrhoeae
- screening
- STD control
- syphilis serology
- Treponema pallidum
- treponemal infection
Statistics from Altmetric.com
- Antiretroviral thera
- Chlamydia trachomatis
- cost-effectiveness
- guidelines
- health service research
- HIV
- HIV prevention
- infectious diseases
- Neisseria gonorrhoeae
- screening
- STD control
- syphilis serology
- Treponema pallidum
- treponemal infection
Regularly screening persons living with HIV (PLWH) for Neisseria gonorrhoeae and Chlamydia trachomatis is expected to decrease HIV transmission and reduce the sequelae of pelvic inflammatory disease. Prompting interventions to change high-risk sexual behaviour and reducing genital fluid HIV levels are mechanisms by which N gonorrhoeae/C trachomatis detection and treatment may reduce HIV transmission.1–5 In diverse locations, the prevalence of gonorrhoea and/or chlamydia among patients attending HIV clinics has ranged from 2.5% to 11%.6–17 The incidence may be as high as 15/100 person-years.7 The majority of gonorrhoea/chlamydia infections among PLWH are asymptomatic.6–8 18
In 2003, the US Centers for Disease Control and Prevention and other health and professional organisations strengthened earlier recommendations to screen all sexually active PLWH for gonorrhoea/chlamydia upon enrolment into care and at least annually thereafter.19 20 Oral and rectal (extragenital) sites should be included based upon sexual history. Among men, we have previously demonstrated an increase after 2003 in the level of gonorrhoea/chlamydia screening upon enrolment into HIV care.21
We hypothesised that as a result of the 2003 guidelines, the proportion of HIV patients diagnosed with gonorrhoea/chlamydia would have increased during 1999–2007. This hypothesis presupposed that the proportion of patients tested annually would have increased after 2003 and that the proportion found positive among those tested would have remained relatively constant. To test our hypothesis, we determined trends in the proportion of patients tested annually, the proportion positive among those tested, and the resulting proportion diagnosed with gonorrhoea/chlamydia among all patients in care within a large HIV clinic in Baltimore, Maryland, USA.
Methods
Since 1989, the Johns Hopkins HIV Clinical Cohort study has offered enrolment to all patients who initiate longitudinal care at the Johns Hopkins Hospital HIV clinic. Over 99% of patients have enrolled. As described elsewhere,22 technicians abstract comprehensive demographic, clinical and laboratory data from medical records, health system databases and outside facilities. Use of the Johns Hopkins HIV Clinical Cohort for this analysis was approved by the Johns Hopkins School of Medicine Institutional Review Board (NA_00028824).
For each participant, we identified active calendar years as those with at least one outpatient visit and at least one measured CD4 cell count. Because the 2003 guidelines call for gonorrhoea/chlamydia screening upon enrolment into HIV care as well as annually thereafter, the year of enrolment was included if enrolment occurred at least 90 days before 31 December. For subjects exiting the cohort, the exit year was included if exit occurred after 1 July.
The first outcome, the occurrence of gonorrhoea/chlamydia testing, was a binary variable determined for each year of active follow-up and was considered positive if the patient had at least one completed test (either culture or nucleic acid-based) of the genital, rectal, or oral areas for gonorrhoea and/or chlamydia. At the population level, this variable was defined as the proportion tested. The second outcome, the occurrence of gonorrhoea/chlamydia positivity if tested, was a binary variable determined for each year in which testing occurred; it was considered positive if the patient had at least one positive result for gonorrhoea, chlamydia, or both. At the population level, this variable was defined as the proportion positive among those tested. The occurrence of being diagnosed with gonorrhoea/chlamydia was defined as having at least one positive result during a year of active clinic follow-up regardless of being tested or not. At the population level, this variable was termed the proportion diagnosed with gonorrhoea/chlamydia among all those in care.
During the study period, culture was available for all sites and was the only accepted method for the mouth and rectum. From 1999 to 2001, nucleic acid testing was performed using PACE 2 (Gen-Probe, San Diego, California, USA) and was available for cervical and male urethral swabs. From 2001 to 2007, nucleic acid testing was performed using AMPLICOR CT/NG (Roche Molecular Diagnostics, Branchburg, New Jersey, USA), and male urine specimens were accepted.
We measured several exposure variables that may have served to confound our assessment of trends. Age, number of clinic visits, CD4 cell count, HIV-1-RNA level and the occurrence of syphilis testing were time-varying exposures specific to each calendar year. For CD4 and HIV-1-RNA data, mean values were created from all results within each year. Syphilis testing was defined as having at least one rapid plasma reagin test within a year. For purposes of analysis, race/ethnicity was classified as African-American and white/other. HIV risk factor was classified as sexual risk (including any same-sex male contact (men who have sex with men; MSM) or high-risk heterosexual exposure, even if in conjunction with another risk factor) and non-sexual risk.
Analysis was performed using repeated measures logistic regression using generalised estimating equations. After exploration of the within-subject correlation of outcomes over time, exchangeable working correlation structures with robust variance estimators were selected. Because of the a priori hypothesis that the proportion tested annually would change in 2003, calendar time was explored both as a simple linear variable and as a linear spline term with an inflection point in 2003. The quasi-likelihood under the independence model criterion (QIC) value was used to select between models.23 To explore whether the data better fit a model with a different change point, we constructed additional models, each with the inflection point at a different calendar year. The final models selected were those with the lowest QIC values. Final multivariate models included all exposure variables for which the bivariate p was less than 0.2. A two-sided type I error of 5% was considered statistically significant. Stata 11.0 was used for all analyses.
Three planned subanalyses were also performed: (1) results stratified by gender; (2) results among MSM only and (3) N gonorrhoeae positivity and C trachomatis positivity analysed as separate outcomes among the full study cohort.
Results
In total, 3283 patients contributed 13 188 person-years of active follow-up during 1999–2007. The cohort was 65% male, 79% African-American and 24% MSM (table 1), and had a median age of 40 years (IQR 35-46) during the first year of study time (either 1999 or the year of clinic enrolment if later). The median yearly number of outpatient visits to HIV and/or gynaecological providers was four (three to six). During each calendar year, approximately 1465 patients (range 1331–1534) were in active care. The median number of years of active care per patient was 3 years (2–6).
Demographic and clinical characteristics
A total of 3437 testing episodes occurred over the study period, with 44% of patients tested at least once. N gonorrhoeae and C trachomatis were tested simultaneously in 94% of episodes, and nucleic acid testing (instead of, or in addition to, culture) was used in 94% of episodes.
Among all patients in care, the proportion tested for gonorrhoea/chlamydia rose from 0.12 in 1999 to 0.33 in 2007 (figure 1A). In a univariate regression, the trend was most efficiently modelled with time as a linear variable with no inflection point. The odds of being tested were estimated to increase by 17% per year (OR per year 1.17, 95% CI 1.15 to 1.19).

Proportion tested and proportion diagnosed with gonorrhoea (NG)/chlamydia (CT) among all those in care. (A) All subjects, (B) women, (C) men and (D) men who have sex with men.
Eighty subjects (6% of subjects ever tested) had at least one positive result during the study interval. Among these 80 subjects, there were 103 positive tests including 60 gonorrhoea only, 38 chlamydia only and five concomitant gonorrhoea/chlamydia infections. Nine subjects had two positive tests and five subjects had three or more positive tests. For patients with multiple positive tests, the median time between repeat positives was 277 days (IQR 111–765).
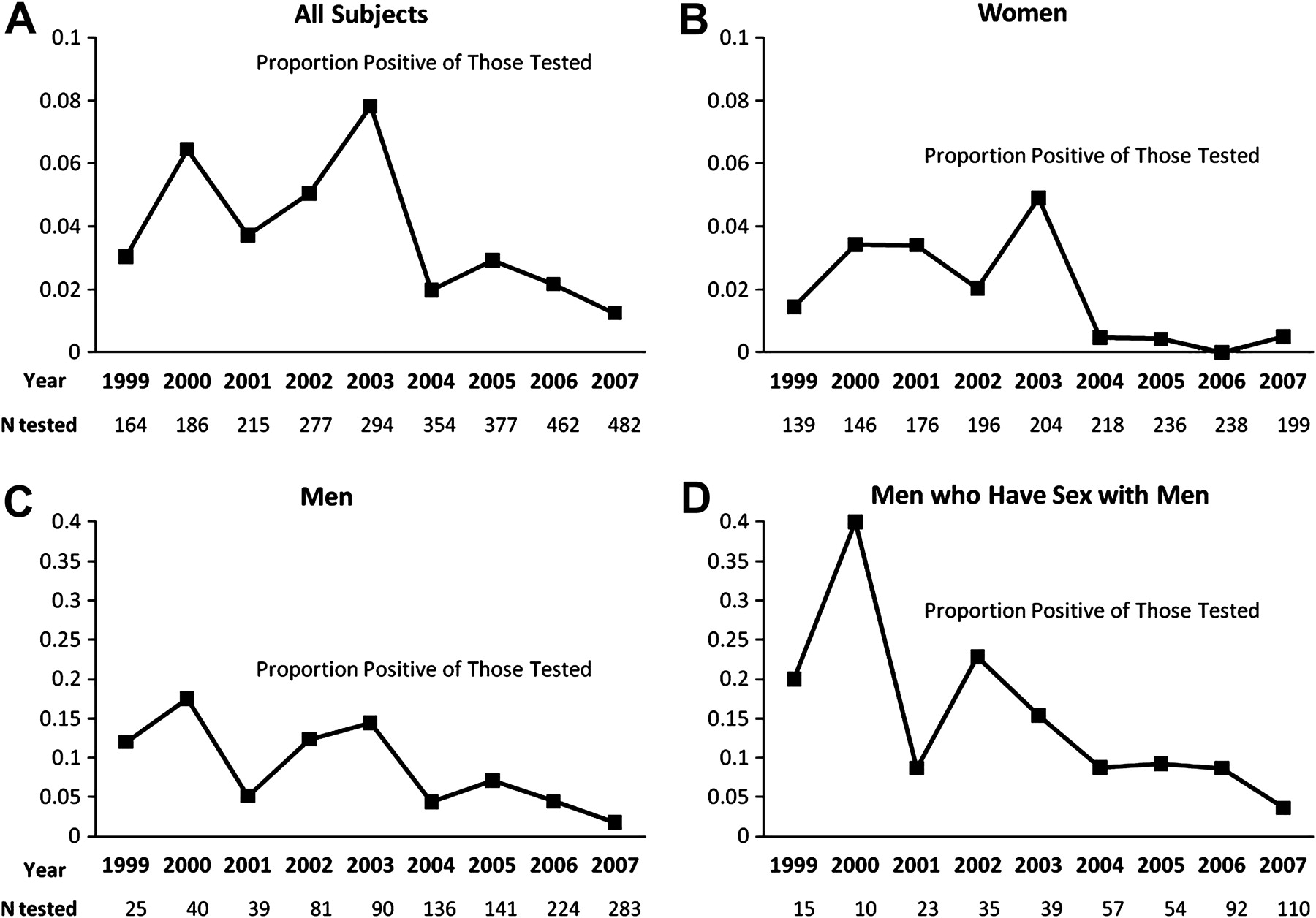
Among all subjects, the proportion positive among those tested varied from a minimum of 0.01 in 2007 to a maximum of 0.08 in 2003 (figure 2A). A univariate regression with year modelled as a linear spline term detected no significant change (OR per year 1.07, 95% CI 0.89 to 1.28) from 1999 to 2003 and then a significant decrease (OR per year 0.67, 95% CI 0.55 to 0.81) from 2003 to 2007.

{kind=link}
{kind=link}
Proportion positive among those tested for gonorrhoea/chlamydia. (A) All subjects, (B) women, (C) men and (D) men who have sex with men.
Among all patients in care, the proportion diagnosed with gonorrhoea/chlamydia ranged from 0.004 to 0.015 and did not show a consistent trend across time (figure 1A). From 1999 to 2003, the proportion diagnosed with gonorrhoea/chlamydia increased (OR per year 1.23, 95% CI 1.04 to 1.47), and from 2003 to 2007 it decreased (OR per year 0.77, 95% CI 0.63 to 0.93). When time was modelled as a simple linear term in 1999–2007, the proportion of all patients in care who were diagnosed with gonorrhoea/chlamydia appeared stable (OR per year 0.97, 95% CI 0.91 to 1.04).
In multivariate analysis of the proportion tested annually, the calendar time trend was most parsimoniously fit with an inflection point in 2001, with an estimated steeper annual increase following 2001 (OR per year 1.13, 95% CI 1.04 to 1.24 from 1999 to 2001 and OR per year 1.28, 95% CI 1.25 to 1.31 for 2001–7, table 2). Other factors significantly associated with the occurrence of gonorrhoea/chlamydia testing included female gender, younger age, African-American race, more visits per year, CD4 cell count greater than 350 cells/mm3 and being tested for syphilis. In multivariate analysis of the occurrence of gonorrhoea/chlamydia positivity if tested, earlier calendar year, male gender, younger age, and CD4 cell count greater than 350 cells/mm3 were significantly associated (table 3).
Factors associated with the occurrence of gonorrhoea/chlamydia testing among 3283 subjects in care
Factors associated with the occurrence of positive results among 1434 subjects ever tested
Subanalyses
The first subanalysis revealed that every year women were more likely to be tested for gonorrhoea/chlamydia than men, but this difference was almost eliminated by 2007 (figure 1B,C). For both genders, annual testing increased significantly across the study period. The proportion positive among those tested was generally lower in women (average across all years 0.017) than men (0.062). In both genders, the univariate and multivariate time trends were similar to that seen in the full cohort with relative stability from 1999 to 2003 followed by significant declines from 2003 to 2007. Among men who were tested, MSM status was associated with having a positive result (adjusted OR 2.19, 95% CI 1.03 to 4.67).
The second subanalysis was of MSM. Approximately 350 MSM were in care each year. Similar to the cohort of all men, a steadily increasing trend in the proportion tested in 1999–2007 was evident (figure 1D), and a significant decrease in the proportion positive among those tested was evident starting in 2003 (figure 2D). The proportion of MSM tested at extragenital sites (rectum or pharynx) was approximately 0.02 each year, and this proportion did not change significantly over time (OR per year 0.99, 95% CI 0.88 to 1.12). Five of 50 (10%) extragenital site tests (two rectal gonorrhoea, two rectal chlamydia and one oral gonorrhoea) were positive.
The third subanalysis separately examined the proportions of positive gonorrhoea and chlamydia results among all patients tested. In both cases, relative stability was seen in 1999–2003 (for gonorrhoea OR per year 1.03, 95% CI 0.83 to 1.29; for chlamydia OR per year 1.15, 95% CI 0.86 to 1.55) followed by statistically significant (or nearly so) declines from 2003 to 2007 (for gonorrhoea OR per year 0.57, 95% CI 0.43 to 0.75; for chlamydia 0.77 per year, 95% CI 0.58 to 1.01).
Discussion
During 1999–2007, the proportion of patients in care who were diagnosed with gonorrhoea/chlamydia did not increase. The proportion tested increased steadily from 0.12 in 1999 to 0.33 in 2007, but this increase was countered by a sharp decline in positive results among those tested. These findings are relevant to the evaluation of guidelines issued in 2003, which call for universal annual gonorrhoea/chlamydia screening among PLWH.
We suspect that the proportion of clinic patients diagnosed with gonorrhoea/chlamydia remained stable because the additional testing in later years did not occur at body sites or among patients likely to test positive. Over the study interval, there was no increase in the proportion of MSM tested at oral and rectal sites. Although the number of MSM tested at extragenital sites was too small to be conclusive, the 10% positive rate is consistent with extragenital sites being a substantial reservoir of undetected infections. Patients, MSM or otherwise, who rarely attend clinic, who avoid testing, or who are infrequently offered screening because of multiple competing medical issues may be the patients most frequently infected with N gonorrhoeae and C trachomatis and thus could represent another reservoir of undetected infections. Although less frequent clinic attendance was not associated with having a positive result among individuals tested, such an association may have been apparent if all or nearly all patients in care had been tested each year.
Publicly reported sexually transmitted infection data for Baltimore in 1999–2007 do not reveal evidence of a strong declining trend in the number of gonorrhoea/chlamydia diagnoses per capita. Comparing 2004–7 with 1999–2003, combined gonorrhoea and chlamydia diagnoses per capita in Baltimore exhibited a 5% decrease,24 which is far less than the 59% decrease in the proportion of tests positive seen in our study between these time periods. While we cannot rule out a tripling of the proportion of the city-wide population tested (such as occurred in our clinic), we have no reason to believe such an uptake in testing happened during 1999–2007 as there were no large-scale city gonorrhoea/chlamydia campaigns. Also, we do not believe that detection remained stable because providers were effectively capturing most incident cases before 2003. This would imply a less than 1% point prevalence in our clinic population, which is inconsistent with literature predicting a 2.5–11% point prevalence6–17 and with the overall high rates of gonorrhoea/chlamydia in Baltimore.25
Kahle et al26 evaluated trends in the proportion tested for gonorrhoea/chlamydia and the proportion diagnosed among 1720 HIV-infected persons in Seattle before and after publication of local guidelines for annual screening in 2001. The proportion tested for gonorrhoea/chlamydia increased from approximately 0.1 before the guidelines to 0.2 afterwards (reported data extrapolated to yearly intervals). Similar to our results, the proportion diagnosed with chlamydia among all individuals in care remained unchanged. In contrast, the proportion diagnosed with gonorrhoea increased.
Contrary to the hypothesised large uptake after 2003, annual gonorrhoea/chlamydia testing in our clinic increased uniformly across the study period. The uniform rise may be explained by providers gradually adopting new behaviour as supporting literature accumulated.1–3 6 8 20 27 The multivariate analysis estimated a small upward inflection in 2001; a contributing factor may be the introduction of urine sampling (replacing urethral swabs) for nucleic acid testing in men in 2001.
Similarly low proportions of patients tested for gonorrhoea/chlamydia (ranging from 0.15 to 0.33) have been reported in multiple US and international HIV clinics despite local guidelines.6 15 16 26 28 29 These collective findings suggest that implementing universal gonorrhoea/chlamydia screening is difficult. Remembering and finding time to broach sexual health and convincing patients to submit non-blood samples may represent substantial challenges. The very low level of extragenital testing among MSM probably reflects these challenges. Additional evidence that obtaining non-blood samples may be a major barrier comes from the comparison of gonorrhoea/chlamydia testing with syphilis testing in our subjects. During 1999–2007, the proportion of patients tested annually for syphilis (data not shown) ranged from 0.53 (2007) to 0.64 (2001), and thus was substantially higher than for gonorrhoea/chlamydia in all years.
Our increase in the proportion of patients tested for gonorrhoea/chlamydia without a resultant rise in detection signifies a need for additional studies on the feasibility and cost-effectiveness of a universal screening approach. Our study is the first that we know of to compare the proportion of patients in care diagnosed with gonorrhoea/chlamydia before and after the 2003 guidelines. Before strong conclusions about the effectiveness of a universal approach can be drawn, studies from additional centres are needed. Also, our clinic's implementation fell too far short of standards to be able to draw strong conclusions about a universal approach. Better implementation has been reported.15 29 30 During 2005, an HIV clinic in Melbourne, Australia, performed complete genital and extragenital gonorrhoea/chlamydia testing on 41% of MSM.15 Further research is needed to determine if high (eg, >50%) adherence to universal screening with appropriate coverage of extragenital sites can be routinely implemented in HIV clinics and if such an approach is optimal for case detection.
An alternative to universal screening that deserves implementation and cost-effectiveness research is targeted screening of high-risk groups. Targeted screening offers the advantage of requiring far fewer tests, but it may be inconvenient for providers repeatedly to reassess risk status. Many studies, including the present, have examined predictors of positive results among those tested, and have therefore shed some light on defining high-risk groups.6 7 11 26 It should be noted, however, that our findings of factors associated with gonorrhoea/chlamydia positivity are open to bias given that we could only examine the 44% of patients who were ever tested.
Urethral gonorrhoea in men contrasts with other sites of infection in both men and women and with chlamydia at all sites because it is more likely to be symptomatic.31 This should be considered when determining whether a population of men should undergo screening, as opposed to diagnostic (symptom-prompted) testing, at the urethral site. In previous studies of HIV-infected MSM, 80–100% of gonorrhoea (and, interestingly, nearly the same proportion of chlamydia) found during screening (ie, all patients were asymptomatic at the time) were from extragenital sites.7–9 Therefore, another scenario to consider from health, feasibility and cost standpoints is whether screening in HIV-infected MSM should be limited to extragenital sites.
Our study is limited by our inability to distinguish diagnostic testing from screening. We suspect the majority of increased testing in later years represented screening. A steady yearly increase in symptomatic complaints among patients in care seems unlikely without a rise in the proportion diagnosed with gonorrhoea/chlamydia. Although our clinic provides comprehensive HIV and primary care, some patients may have been treated for gonorrhoea/chlamydia at other locations such as emergency rooms. We do not suspect that a large rise in such treatment occurred after 2003. Our data come from a single clinic with a large population of African-American individuals and injection drug users. Nonetheless, our findings may be applicable to many urban HIV clinics.
Our study has found that an increase in the proportion of patients undergoing annual testing for gonorrhoea/chlamydia during 1999–2007 was not associated with an increase in the proportion of patients found to be infected. Our findings indicate a need to re-evaluate the clinical effectiveness and cost-effectiveness of a universal screening approach for gonorrhoea/chlamydia case detection compared with alternatives such as targeted screening of high-risk groups. Until clear evidence exists, annual gonorrhoea/chlamydia screening according to guidelines should continue being promoted. Better implementation of universal screening may be widely feasible and may increase case detection.
Key messages
Widening testing for gonorrhoea and chlamydia did not increase detection of these sexually transmitted infections in an HIV clinic population.
Screening oral and rectal sites among MSM may be especially important to gonorrhoea/chlamydia case detection in HIV clinics.
If efforts to improve implementation of universal gonorrhoea/chlamydia screening do not increase detection, targeted screening of high-risk PLWH may be preferable.
Acknowledgments
The authors are grateful to all the patients, physicians and staff involved in the Johns Hopkins HIV Clinical Cohort.
References
Footnotes
Conference presentation: The findings herein were presented, in part, at the 47th Annual Meeting of the Infectious Diseases Society of America, 1 November 2009, oral abstract #1258.
Funding This study received funding from the National Institutes of Health K23AI084854, R01 AG026250, R01 DA011602, R01 AA16893, K24 DA00432 and the National Center for Research Resources KL2RR025006-01.
Competing interests RDM has been a consultant for Bristol-Myers Squibb and has received research funding from Merck, Pfizer, and Gilead. KAG has been a consultant and received research funding from Tibotec. All other authors report no conflicts of interest.
Ethics approval This study received ethics approval from the Johns Hopkins School of Medicine Institutional Review Board (NA_00028824).
Provenance and peer review Not commissioned; externally peer reviewed.