Article Text

Abstract
Objective To integrate the empirical estimates of bisexual behaviour among the bridge population of men who have sex with men (MSM) in China and their HIV and syphilis prevalences stratified by sexual behaviour.
Methods The Pubmed, Chinese Biomedical, Chinese National Knowledge Infrastructure, VIP, Wanfang and Google Scholar databases were searched to January 2011 to identify relevant articles. Data of eligible citations were extracted by two reviewers. All analyses were performed using Stata 10.0.
Results Forty-nine articles (including 28 739 MSM subjects) met the selection criteria. Aggregated findings indicated that the estimated prevalence of bisexual behaviour among MSM in China is 31.2% (95% CI 28.1% to 34.5%). HIV and syphilis prevalences were 5.4% and 11.4%, respectively, among MSM engaging in bisexual behaviour and 3.8% and 9.3% among MSM only having sex with men. HIV prevalence among MSM engaging in sex with both men and women was significantly higher than in those who only have sex with men (OR 1.30; 95% CI 1.04 to 1.62; p=0.02).
Conclusion There is a high prevalence of bisexual behaviour among MSM in China and bisexual behaviour is significantly associated with increased HIV infection risk. The results of this meta-analysis highlight a critical pattern of HIV transmission among MSM in China and indicate that targeted interventions aimed at encouraging safe sex practices and promoting societal and family acceptance of MSM are urgently needed.
- Bisexual behaviour
- CDC
- CD4
- China
- epidemiology (general)
- gay men
- gonorrhoea
- HIV/AIDS
- hepatitis
- homosexuality
- immunology
- men who have sex with men
- prevention
- sexual behaviour
- syphilis
Statistics from Altmetric.com
- Bisexual behaviour
- CDC
- CD4
- China
- epidemiology (general)
- gay men
- gonorrhoea
- HIV/AIDS
- hepatitis
- homosexuality
- immunology
- men who have sex with men
- prevention
- sexual behaviour
- syphilis
According to UNAIDS statistics, in 2008 approximately 70–80% of HIV infections worldwide were acquired through unprotected sexual transmission. In particular, the HIV infection rate of men who have sex with men (MSM) is climbing at an alarming rate.1 MSM are a key population for HIV prevention, not only because they often have multiple sexual partners and unprotected intercourse, but also because they can play both the insertive and receptive roles during intercourse, which could elevate the risk of transmission.2 In mainland China, the proportion of HIV cases attributed to MSM has increased rapidly, from 12.2% of new HIV infections in 2007 to 35.2% of new HIV cases in 2009.3 4 Because homosexuality in China remains highly stigmatised, MSM are a hidden population and many cite a fear of ‘losing face’, meaning damage to their social integrity, as a barrier to revealing their sexual orientation.5 In order to cope with parental pressure for marriage or in order to have offspring,6 many Chinese MSM have sex not only with men but also with women, and in this way, may act as a bridge for HIV transmission to the general population.7
Understanding the frequency of bisexual behaviour among MSM in China is useful for developing targeting interventions and projecting the direction of the national HIV epidemic.8–10 In addition, it is also important to understand whether engaging in bisexual behaviour is associated with HIV or syphilis infections, as this could have important public health implications for HIV control and prevention. However, several small-scale studies have researched the bisexual behaviours of MSM in China, in which some even drew contradictory conclusions. It is still unknown what proportion of Chinese MSM also engage in sex with women. In order to gain a more comprehensive understanding of the associations between HIV, syphilis and bisexual behaviour among the MSM population, we systematically searched the literature and performed a meta-analysis to estimate the prevalence of bisexual behaviour among Chinese MSM and analysed HIV and syphilis prevalences stratified by bisexual behaviour.
Methods
Study selection
The Pubmed, Chinese Biomedical, Chinese National Knowledge Infrastructure, VIP, Wanfang and Google Scholar databases were searched to January 2011 to identify relevant articles. The keywords and medical subject headings pertaining to MSM including ‘men who have sex with men’, ‘MSM’, ‘gay’ and ‘male homosexual’ and sexual behaviours including ‘married’, ‘heterosexual sex’, ‘bisexual behaviour’, ‘bisexual sex’, ‘female partners’, ‘bisexuality’, ‘sexual partners of both genders’, ‘sex with men and women’ and ‘sex with females’ were used to screen for potentially relevant studies. Studies that met the following criteria were included in the meta-analysis: included Chinese MSM participants; reported quantitative data of recent heterosexual behaviour (recall window ≤12 months) and HIV or syphilis prevalence stratified by sexual behaviour pattern or marital status. Duplicate reports, those without mention of the period of the recall window of bisexual behaviour or behaviour recall window longer than 12 months, or studies of male sex workers were excluded. The literature was limited to those published in Chinese and English as both reviewers are fluent in these languages. When additional data were needed, attempts were made to contact authors to access relevant data.
Data extraction and study quality assessment
Data from eligible studies were extracted by two reviewers independently. The following information was abstracted: first author, date of publication, data collection period, study location, sampling method, study design, method of data collection, recall window of bisexual behaviour, sample size, number of MSM engaging in bisexual behaviour and the number of HIV and syphilis seroconversions confirmed by laboratory testing among MSM stratified by sexual behaviour. Excel spreadsheets were used for data extraction. Disagreements between the two reviewers during data extraction were reconciled by discussion.
The quality assessment checklist for observational studies (QATSO score) concerning HIV prevalence/risk behaviours among MSM was selected to evaluate the quality of the included studies.11 Items were scored as 1, 0, NA, which corresponded to ‘yes’, ‘no’, or ‘not applicable’, respectively. The total score was divided by the total number of all applicable items. Values between 0% and 33%, 33% and 66% and 67% and 100% reflect ‘bad’, ‘satisfactory’ and ‘good quality’, respectively.
Methodological approach
The following rules guided data extraction:
Only studies reporting quantitative data of recent bisexual behaviour (recall window ≤12 months) or HIV or syphilis prevalence stratified by sexual behaviour or marital status among Chinese MSM were used to calculate effect sizes.
If study data were published in multiple articles, the most comprehensive study was selected for data abstraction.
Qualitative and post-intervention studies were excluded.
Analytical methods
The pooled prevalence of bisexual behaviour among MSM was calculated using the inverse variance method as follows. First, the proportion variables were transformed into continuous variables using the Freeman-Tukey arcsin transformation,12 for suitability for the data analysis of fixed and random effects summaries. Next the weighted mean of the transformed proportions was calculated; and its 95% confidence interval was obtained by determining limits that were 1.96 times the standard errors below and above it. If tests met the hypothesis of homogeneity, fixed effects models using inverse arcsine variance weights were used to estimate the overall prevalence across studies, otherwise random effects models using DerSimonian–Laird weights were used.13 In the end, the pooled outcome and its 95% CI were back-transformed into proportions. If a report included a prevalence of 0%, the prevalence was considered to be 0.000001 for the calculation of the pooled prevalence. Pooled estimates of HIV and syphilis prevalences were calculated along with the OR stratified by bisexual behaviour (MSM with both male and female partners vs MSM who only had sex with male partners). Statistical heterogeneity was measured using the Q statistic and quantified using the I2 index. An I2 value of less than 25% was considered to reflect low heterogeneity, 50% moderate heterogeneity and 75% high heterogeneity.
The differences among the reported prevalence rates in the studies might be due to the variations in the main characteristics of the target population and methodological differences such as sampling methods, sampling time and recall windows. Therefore, subgroup analysis was conducted by study location (northeast (Heilongjiang, Jilin and Liaoning); north (Beijing, Tianjin, Hebei, Shandong, Henan and Shanxi); northwest (Xinjiang, Qinghai, Gansu, Inner Mongolia, Tibet, Ningxia and Shaanxi); southwest (Sichuan, Yunnan and Guizhou); southeast (Jiangsu, Anhui, Shanghai, Zhejiang, Jiangxi, Hubei and Hunan) and south (Guangdong,Guangxi and Fujian)) based on similarities in the natural and social-economic conditions; sampling settings (venues where MSM are known to congregate (eg, saunas, bars, public parks), voluntary counselling and testing (VCT) centres and other MSM networks (the internet and outreach by MSM-oriented non-governmental organisations (NGO)); sampling method (respondent-driven sampling (which simulates random sampling) and all others); data collection method (interviewer-administered and self-administered); recall window of bisexual sex (3 months, 6 months and 12 months); data collection period (before 2006 and after 2006); and study quality (those that were ‘bad’, ‘satisfactory’ and ‘good’) to examine potential heterogeneous factors that may influence the pooled outcome.
Because conclusions from subgroup analyses are based on the subdivision of studies and indirect comparisons, and not on formal statistical tests, univariate and multivariate meta-regression techniques were used to test formally whether there is evidence for different effects related to different characteristics of trials. Variables in univariate analysis with p<0.10 were entered into multivariate models. Variables with p<0.05 in the multivariate model were considered statistically significant.
Sensitivity analysis was conducted to examine the impact of methodological quality, different statistical models and study effect size. The meta-analysis was re-analysed by three methods: (1) excluding low quality studies; (2) using a fixed effects model; (3) the overall pooled prevalence was compared with estimates obtained after iterations using k−1 studies (k equals the number of studies). Egger's regression test was used to detect potential publication bias by examining the symmetry of funnel plots. All analyses were performed using Stata V.10.0.
Results
Identification and selection of eligible studies
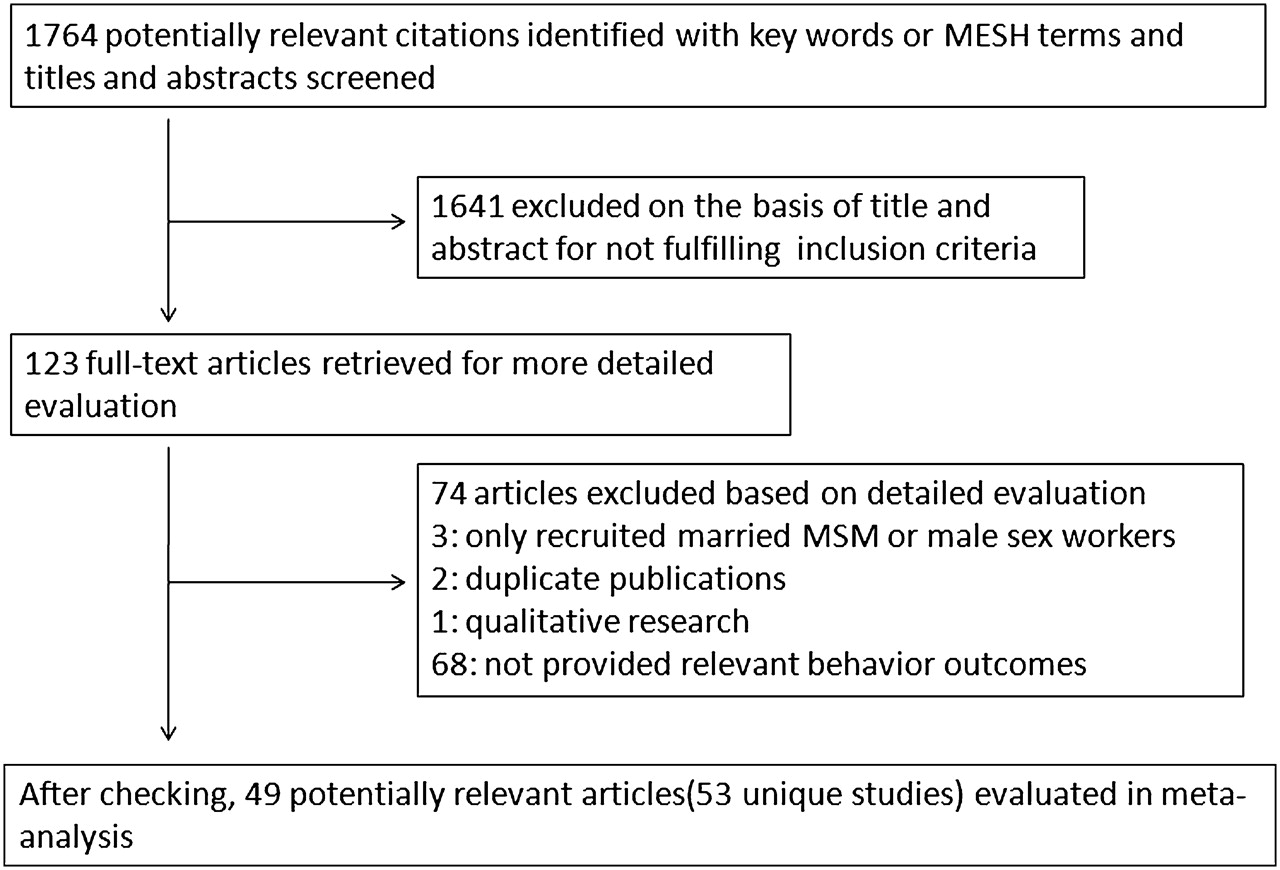
In total, 1764 relevant citations were identified, of which 123 articles were selected for further screening, and 49 articles (11 published in English and 38 in Chinese) met the inclusion criteria (figure 1). Table 1 provides a descriptive summary of these studies. The minimum reported prevalence of bisexual behaviour was 10.6% in Beijing and the highest prevalence was 62.7% in Shenzhen.
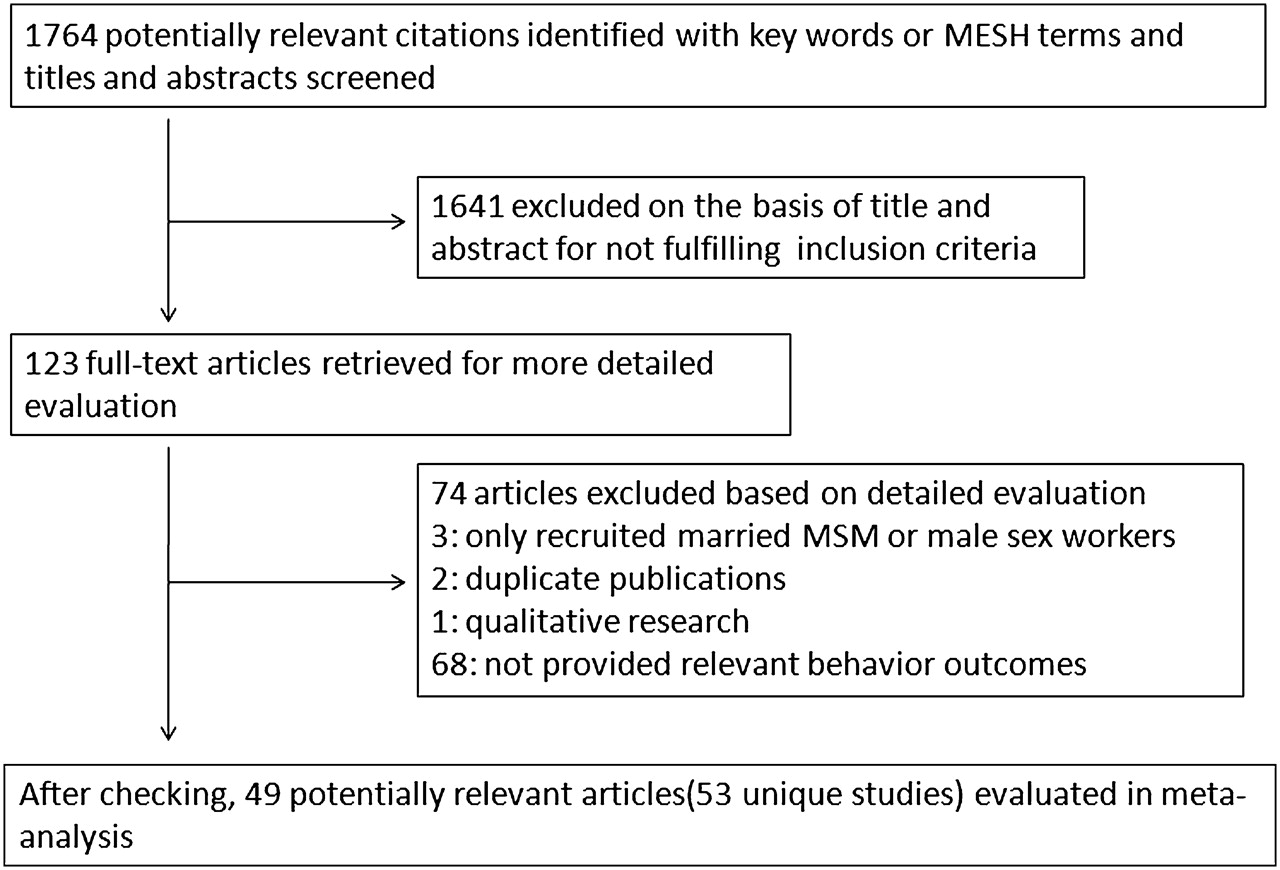
Flow diagram of studies included in analysis. MSM, men who have sex with men.
Characteristics of studies describing recent heterosexual behaviour among MSM in China
Estimated prevalence of bisexual behaviour
There was substantial heterogeneity between studies (I2=96.5% (95% CI 96.1% to 96.8%), Q test p<0.01), random effects models (Der Simonian–Laird) were, therefore, used. The aggregated findings indicate that the estimated prevalence of bisexual behaviour is 31.2% (95% CI 28.1% to 34.5%) (figure 2).
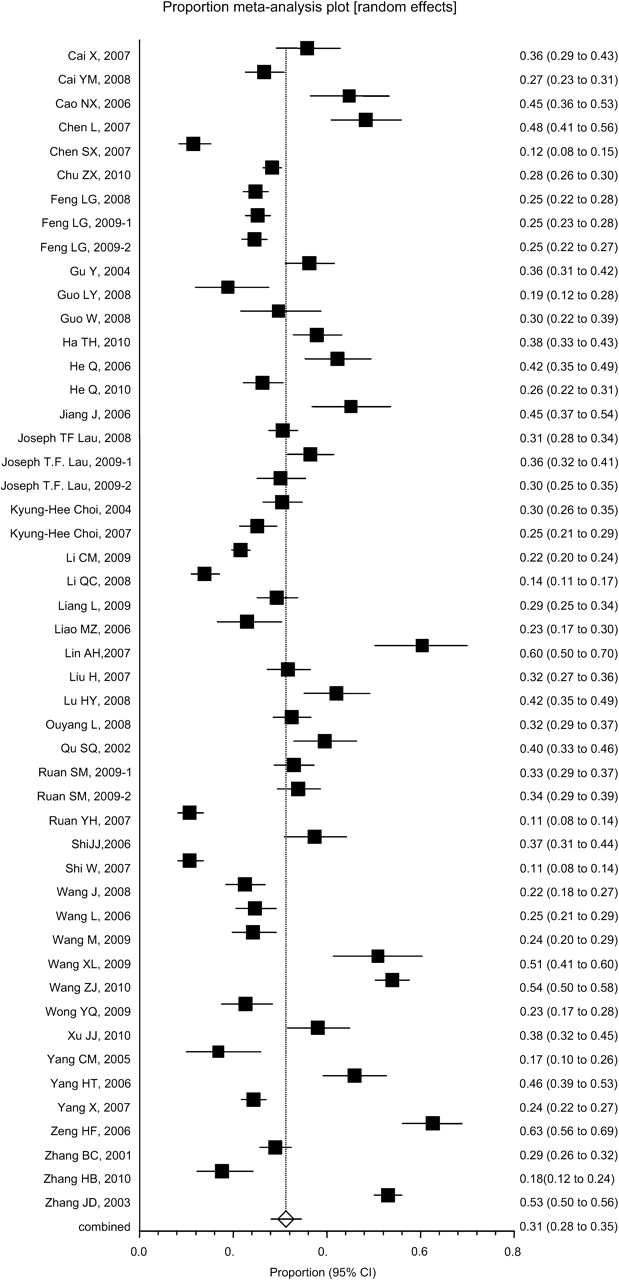
Prevalence estimates of bisexual behaviour among men who have sex with men in China.
Subgroup and meta-regression analyses
Because high heterogeneity was observed, a series of subgroup analyses were conducted. As seen in table 2, prevalence estimates for bisexual behaviour among those who self-administered questionnaires were higher than those of the interviewer-administered group (36.5% vs 28.4%); and were higher among studies that recruited participants from MSM venues and via NGO compared with those through VCT and other MSM networks (35.1% and 38.9% vs 23.8% and 26.7%). Regions varied in their prevalence of bisexual behaviour. Across the entire country of China, the summary prevalence was the highest (40.8%), followed by south (40.3%), east (32.6%), northeast (31.0%), southwest (27.3%), and north China (26.1%). For studies that used a 12-month behaviour recall window, the prevalence of bisexual behaviour was higher than those taken with 6-month or 3-month recall windows (41.7% vs 29.0% vs 29.1%). The prevalence of bisexual behaviour for studies recruiting participants through respondent-driven sampling compared with all other sampling methods was 29.8% and 31.8%, respectively. The pooled estimates for studies with good quality, 1000 or greater sample size or collected data in 2006 and later were lower than those scored satisfactory, fewer than 1000 sample size or collected data before 2006. Although subgroup analyses were conducted, variations were still present within each of these subgroups. Meta-regression was additionally conducted to examine formally the relationship between these possible heterogeneous factors and the overall estimate of bisexual behaviour. The results showed that only the sample setting was a marginally significant factor (p=0.064).
Prevalence of bisexual behaviour among MSM by study and design characteristics
Sensitivity analysis and publication bias
In sensitivity analysis, the conclusions remained robust. The outcome was not altered when a fixed effects model was used (29.4%, 95% CI 28.8% to 29.9%). When only ‘good’ quality studies were evaluated, the prevalence was also not significantly altered (29.6%, 95% CI 23.9% to 35.5%). And the k−1 sensitivity tests did not reveal any individual study that exerted influence on the total outcome. Egger's regression test showed that there was negligible publication bias among the included studies (bias 3.19; 95% CI −1.37 to 7.74; p=0.17).
Pooled prevalence of HIV and syphilis among MSM with and without bisexual behaviour in China
Given the considerable heterogeneity among studies (I2=93.6% and 91.7%, Q test p<0.01) (table 3), random effect models were used to estimate the summarised HIV prevalence. The summarised HIV prevalence was 5.4% among 12 studies on bisexual behaviour and 3.8% among 10 homosexual behaviour studies. Having sex with both male and female partners was associated with a 30% increase in the odds of HIV infection (OR 1.30; 95% CI 1.04 to 1.62; p=0.02 for overall effect) (table 3).
HIV/syphilis prevalence estimates among Chinese MSM with and without bisexual behaviour
Six studies examined the association between sexual behaviour patterns and syphilis prevalence. Significant heterogeneity was observed for the calculation of syphilis prevalence. The aggregated syphilis prevalence was 11.4% among MSM with bisexual behaviour compared with 9.3% among MSM who had only engaged in homosexual sex. Pooled results showed no significant association between the infection of syphilis and having female partners (OR 1.07; 95% CI 0.82 to 1.40; p=0.64 for overall effect) (table 3).
Discussion
This is the first meta-analysis of bisexual behaviour among MSM in China, which found that almost one-third of study participants had had sex with women. According to statistics from the Chinese Ministry of Health, there are approximately 5–10 million MSM in China,4 and considering the low rates of condom use,58 China's HIV epidemic could easily spread from this high-risk group to the general population.59
An explanation for the high prevalence of bisexual behaviour among Chinese MSM might be due to traditional social norms. Chinese society, like many Asian cultures, emphasises the importance of social standing and homosexuality remains highly stigmatised.60 61 Many homosexuals are pressured to get married or to date women in order to meet family expectations and societal standards of masculinity.61 Encouraging societal and familial acceptance and promoting the understanding of homosexuality may be an effective means of changing Chinese social norms.62 63 Chinese MSM are a complex group; male commercial sex workers (ie, ‘money boys’) and a proportion of rural migrant workers who are distanced from their wives and girlfriends have sex with men, but would not consider themselves gay.64 65 Large numbers of male sex workers and migrant rural workers64 65 and convenient means of communication such as the internet could facilitate the high prevalence of bisexual behaviour.
Attempts were made to explore sources of heterogeneity by clinical and methodological variables by subgroup and meta-regression analyses; however, the degree of heterogeneity did not decrease after pooling different subgroups, indicating the presence of other sources of heterogeneity. In all included studies, because MSM was one of the nation's hardest to reach populations, non-probability sampling (eg, convenience and snowball sampling) was often used to sample from the targeted population, which may not be representative of the population of interest. The variation in the overall estimates in different sampling settings reflected this problem. Sampling methods and sampling settings could explain the high heterogeneity and indicate that probability-based sampling methods are important for precise estimations of the health status of MSM in China. In addition, behavioural and demographic characteristics of MSM may also be sources of heterogeneity, but detailed information on these variables could not be abstracted from the literature. However, the re-analysis of these data from high quality studies and by fixed effects models demonstrated a robust outcome, and the sensitivity tests did not reveal any individual study that exerted influence on the overall prevalence estimate.
Although the association did not reach statistical significance, subgroup analysis can also give some meaningful qualitative conclusions. Subgroup analysis by study regions may give an overall description of the present condition of bisexual behaviour among MSM in China. As seen from figure 3, the higher prevalences of bisexual behaviour were mostly found in coastal cities with rapid economic development and regions with large floating populations and flourishing sex industries, such as ‘south China’ (42.6%) and ‘east China’ (31.8%). So targeted measures should be taken, which consider the risk profile of MSM in different regions of China in order to curb the spread of HIV.

{kind=link}
{kind=link}
{kind=link}
The regional distribution of pooled prevalence of bisexual behaviour among men who have sex with men in China.
This meta-analysis also found that having sex with both men and women seems to be a significant risk factor that increased the odds of HIV infection by 30% compared with MSM who only had male sex partners. These results are quite similar to a study of Indian MSM, which found that those with partners of both genders were more likely to be HIV infected (adjusted OR 2.73).66 Some studies have reported that men with bisexual behaviour were less likely to have always used condoms during the past year for vaginal sex than for insertive anal sex with men,67 68 and having sex with women increased the likelihood of insertive unprotected anal intercourse with men.69
This meta-analysis is subject to several limitations. The data were mostly abstracted from cross-sectional studies, which cannot describe changes in bisexual behaviour over time. Original studies on HIV and syphilis prevalences by sexual behaviour or marital status are limited, so the results of the current study should be confirmed with large cohort studies. In addition, the literature that reported HIV and syphilis prevalences, only classified marital status as either ‘single’ or ‘married or cohabitating’. The prevalence of bisexual behaviour among MSM who are divorced or widowed may differ from these two groups, and the sexual behaviour of these other marital statuses should also be considered in future research. Another limitation is that most of the surveys were performed in urban areas with the exception of two mailed questionnaires, which were conducted nationwide, therefore the conditions of MSM in rural areas warrants further study. The conclusions of the current study should be considered under these limitations.
There is a high prevalence of bisexual behaviour among MSM in China and bisexual behaviour is significantly associated with an increased risk of HIV infection. The results of this meta-analysis highlight a critical pattern of HIV transmission among MSM in China, and indicate that targeted interventions aimed at encouraging safe sex practices and promoting societal and family acceptance of MSM are urgently needed.
Key messages
Chinese MSM engaging in bisexual behaviour may act as a bridge of HIV infection to the general population.
The current study is the first meta-analysis on the prevalence of bisexual behaviour among Chinese MSM.
The estimated prevalence of bisexual behaviour among MSM in China is 31.2% (95% CI 28.1% to 34.5%).
HIV prevalence among MSM engaging in sex with both men and women was significantly higher than in those who only have sex with men (OR 1.30; 95% CI 1.04 to 1.62).
Acknowledgments
The authors appreciate all the researchers whose articles were included in the study. In addition, the authors would like to thank Dr. Kathleen Reilly for reviewing the present article and providing great guidance.
References
Footnotes
Funding This work was supported by the mega-projects of national science research for the 11th Five-Year Plan (2008ZX10001–001); National Nature Science Foundation of China (81001291); Shenyang Science and Technology Plan (F10-149-9-50).
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data are free to sharing with related studies.