Article Text

Abstract
Background Rapid HIV testing is not permitted in Australia at the point of care. The authors evaluate the expected net effect of rapid HIV testing compared with standard serology diagnostic tests in terms of onward HIV transmission.
Methods The authors used data for 174 men who had sex with men testing HIV-positive at the Melbourne Sexual Health Centre, Australia, in an agent-based mathematical model. Time of diagnosis is simulated according to conventional enzyme immunoassays or rapid HIV tests, with different window periods. The authors calculated the expected number of additional/averted transmissions due to missed or earlier diagnoses.
Results Fourth generation rapid tests were simulated to miss ∼2–3% of diagnoses compared with conventional fourth generation enzyme immunoassay tests. However, in the remaining 97–98% of cases the rapid test would result in earlier detection of HIV. Overall, the rapid test would reduce time to patients receiving results by a median of ∼12 days. Assuming no changes in testing rates, the introduction of rapid testing diagnostic technologies would prevent one in every 2000–5000 HIV transmissions compared with the conventional diagnostic test.
Conclusions Rapid tests would have a marginal benefit in reducing HIV transmission between men compared with conventional tests under assumptions of no changes in testing frequencies.
- Rapid test
- HIV
- gay men
- Australia
- mathematical model
- public health
- surveillance
- Chlamydia
- anogenital cancer
- AIDS
- bacterial vaginosis
- epidemiology (clinical)
- NSU
- HIV testing
- HPV
- epidemiology
- case reports
- PID
- STD services
- STD surveillance
Statistics from Altmetric.com
- Rapid test
- HIV
- gay men
- Australia
- mathematical model
- public health
- surveillance
- Chlamydia
- anogenital cancer
- AIDS
- bacterial vaginosis
- epidemiology (clinical)
- NSU
- HIV testing
- HPV
- epidemiology
- case reports
- PID
- STD services
- STD surveillance
Introduction
Worldwide, HIV is responsible for major morbidity and mortality. In many developed countries, men who have sex with men (MSM) constitute the major risk group for HIV acquisition. HIV testing and diagnosis are critical in the prevention and control of HIV. Awareness of positive HIV status is important on an individual level as earlier detection and access to timely antiretroviral therapy leads to improved prognosis and reduced transmission. Individuals who are HIV-positive and aware of their status also usually modify their sexual behaviour to reduce the risk of transmission to sexual partners.1 Thus, improved detection of HIV is likely to lead to improved HIV control.2 3 A recent modelling study has suggested that for MSM who seek partners of the same HIV serostatus as themselves (ie, serosorting), insufficient testing rates among men are likely to lead to greater HIV transmission.4 High testing rates also assist public health surveillance systems for monitoring and evaluating epidemic trends.
Point of care or rapid HIV testing is available for clinical use in many developed and developing countries and their use is supported by the WHO and UNAIDS.5 However, the use of rapid HIV testing technologies as screening tests at the point of care is currently not permitted in Australia. In Australia, there are already high levels of HIV testing among the groups most at risk of HIV infection, namely, gay and other homosexually active men.6 Rapid testing is often cited by individuals as being preferable over conventional testing due to the ease of testing and the immediacy of results,7 8 reducing the waiting time and associated anxiety. Rapid testing removes the typical 1–2-week delay between the testing and the result associated with conventional HIV blood tests and prevents loss of follow-up.9 10 Australian surveys of MSM also strongly indicate preference for rapid HIV testing to conventional serology and therefore its usefulness in Australian context should be further explored.11 12
There are a number of potential limitations with the use of rapid HIV testing. As with conventional HIV enzyme immunoassays (EIAs), rapid tests have a window period and there is the potential for false-negative results as well as the potential for false-positive results.13–15 There are three timeline-related scenarios for the timing of detection of HIV infection: (i) both conventional tests and rapid tests detect infection at the next HIV test following infection; (ii) both conventional and rapid tests detect infection at the second HIV test following infection; (iii) the conventional test detects infection at the first test and the rapid test detects infection at the second test (see figure 1). It is also possible that, due to variations in distributions in window periods between the different diagnostic tests, a conventional test does not detect an infection but is detected by a rapid test.

Schematic timeline of three scenarios regarding the timing of HIV infection and diagnosis with a rapid test or standard enzyme immunoassay (EIA) test relative to the timing of background periodic rates of testing. The star represents acquisition of HIV.
Rapid testing could ostensibly reduce the time between an individual being tested and informed of their HIV diagnosis, reducing transmission. However, a longer window period with rapid testing could lead to missed diagnosis of early infections, which may have been otherwise detected with standard EIAs, with continued transmission occurring. In this analysis, we use a mathematical model informed by clinical data for MSM to estimate the net effect of introducing rapid HIV testing compared with later generation EIAs in terms of further onward transmission of HIV.
Methods
Data for the model were obtained from the medical records of MSM attending the Melbourne Sexual Health Centre (MSHC), Victoria, Australia between July 2002 and May 2009 and who tested positive for HIV for the first time. Any man who reported having sexual contact with a male partner in the 12 months prior to their HIV diagnosis was included in the study. Until 2006, it was standard practice at the MSHC to advise men who had been tested for HIV to return for the test results after 2 weeks. Since 2006, men who were tested for HIV are asked to return for their results after 1 week. A list of HIV-positive men was compiled using information on HIV testing obtained from the Victorian Infectious Diseases References Laboratory, where all HIV serology was processed.
The following data were extracted for use in the model: frequency of sexual activity, including levels of unprotected anal sex in the prior 12 months, HIV viral load at diagnosis and the distribution of the number of days between testing and receiving result. Ethics approval for the project was obtained from the Alfred Hospital Human Research Ethics Committee.
We developed an individual-based mathematical model that simulates 100 000 sexually active gay men in Victoria, Australia who are initially HIV-infected but undiagnosed with their infection. The model simulates regular HIV testing of these men with either a conventional EIA test or a rapid HIV test. These tests are associated with a different window period (ie, time from infection until a test can detect any change). Since there can be uncertainty over when infection actually occurred, we defined the ‘window period’ to be the period between RNA and detectable antibodies. It may be worth noting that there is no precise ‘window period’ at which time a test will detect an infection that it would not have detected prior to this time. Rather, the probability of a positive diagnosis increases over time.16 On the basis of accessible information on the window periods, we used a median (ie, 50% probability of positive diagnosis) of: (i) 5 days for the fourth generation antigen/antibody (Ag/Ab) EIA (such as Abbott's Architect); (ii) 10 days for the third generation EIA; (iii) 10 days for the Determine HIV-1/2 Ag/Ab Combo rapid test (Alere); and (iv) 15 days for the Orasure-produced Oraquick ADVANCE rapid HIV-1/2 antibody test.16 17 There are relatively large uncertainty bounds around such estimates. Based on evidence of the profile of increasing sensitivity of HIV diagnostic tests versus time from the appearance of RNA,16 we used a logistic growth curve with medians equal to these defined window periods such that we captured the increased sensitivity and probability of detecting positive infections (see figure 2A). In the model, each simulated individual is allocated a time of HIV infection that is randomly (and uniformly) distributed in the time between tests. The time between HIV tests is sampled from the empirical distribution of testing frequencies of the MSM who attended the MSHC during the study period and were ultimately diagnosed as HIV-positive: median time between tests was 429 days (IQR=190–1097 days, range 33–5782 days). The duration between infection and testing is then determined. If this duration is less than the window period of the test then diagnosis will not occur but will occur at the time of the next HIV test (ie, the diagnosis would be missed by the first of these two tests). However, if the time between infection and testing is greater than the sampled window period for a given individual then the test will detect the infection: diagnosis and patient notification of detection of HIV will occur on the same day for the rapid test, usually followed by a confirmatory test, but for conventional tests there will be a delay based on the duration until return visit to receive test results. Empirical data from MSM testing positive for HIV at MSHC were used to sample the individual duration between testing and receiving a result for conventional tests.

(A) Assumed sensitivity of HIV diagnostic tests versus the number of days after appearance of HIV RNA for tests of different average ‘window periods’. (B) Assumed HIV transmission rate versus plasma viral load for unprotected anal intercourse according to insertive, receptive with ejaculation and receptive with withdrawal sex. EIA, enzyme immunoassays.
The number of days from the emergence of RNA until diagnosis was calculated for each of 100 000 simulated individuals, according to use of each diagnostic test. We then investigated the epidemiological significance of different diagnostic tests through use of a standard mathematical transmission modelling framework that estimated the expected number of net HIV transmissions caused during the period between diagnosis with a rapid test compared with currently used diagnostic tests. The probability that an infected gay man would transmit HIV on a given day can be mathematically expressed by:
We examined the effect of using two different rapid HIV tests, the Orasure Oraquick test and the Determine HIV-1/2 Ag/Ab Combo test. Through model simulation, these tests were compared with conventional third and fourth generation EIA tests, which are currently used in Australia.
Results
Over the study period, there were 174 MSM diagnosed with HIV. For the 172 men who received their result, the median time between testing and being informed was 9 days (range 3–71 days, IQR 7–14 days). There were two men who did not receive their positive result despite extensive efforts to make contact with them.
Men reported a median of 1 (range 0–3) regular male partner and 10 (range 0–1000) casual male partners over the 12 months prior to their diagnosis. Among men who reported anal intercourse in the prior 12 months, condom use with regular and casual partners was respectively reported as always for 8% and 20% of men, 38% and 72% reported inconsistent use, while 54% and 8% reported never using condoms; the model is sampled from these data, assuming inconsistent use to be a uniform distribution between 0 and 100%.
According to the distribution of testing frequencies and times from testing to receiving results from men attending the MSHC, the average time from infection to receiving a positive result when averaged over very large population sizes was simulated by the model to be 240 days (median, 87–581 IQR) for the fourth generation conventional test; 246 days (median, 92–586 IQR) for the third generation conventional test; 232 days (median, 79–573 IQR) for the Determine-Combo rapid test; 237 days (median, 84–578 IQR) for the Orasure Oraquick rapid test.
The third generation conventional EIA test, with a slightly longer average window period, was simulated by the model to lead to a missed diagnosis in 2.8% of cases when compared with the fourth generation conventional EIA test but due to chance would detect 0.2% of infections not detected by the fourth generation conventional EIA test (figure 3A). The Determine-Combo rapid test simulations missed a similar proportion of diagnoses, 2.4%, as the third generation conventional EIA test. However, in the remaining 97.6% of cases, the Determine-Combo rapid test would allow a test result to be given at the same visit and not require a return visit for initial detection of HIV (pending confirmation) as required with the fourth generation conventional EIA test. Overall, the Determine-Combo rapid test would reduce the number of days until diagnosis by 12 days (median, 7.4–17 IQR) compared with the fourth generation conventional EIA test (figure 3B). By comparison, the Orasure Oraquick rapid test simulations missed 4.4% of infections detected by the fourth generation conventional EIA tested. However, when offset by the gains made in earlier diagnosis for the remaining 95.6% infections, overall the Orasure Oraquick rapid test reduces the number of days until diagnosis by 11.4 days (median, 7.1–16.9 IQR) compared with the fourth generation conventional EIA test (figure 3C).

Cumulative distribution of simulated outcomes from 100 000 gay men on the expected number of days of known HIV positivity due to use of (A) conventional third generation enzyme immunoassay (EIA) tests, (B) Determine-Combo rapid tests and (C) Orasure Oraquick rapid tests, compared with use of the conventional fourth generation EIA tests. The horizontal dashed line defines the threshold of zero extra days of known positivity and thus highlights the estimated percentage of cases with less days of known positivity compared with the conventional fourth generation EIA tests. The vertical dashed line defines the zero extra days of known positivity threshold and the solid vertical line defines the median number of extra days of known positivity.
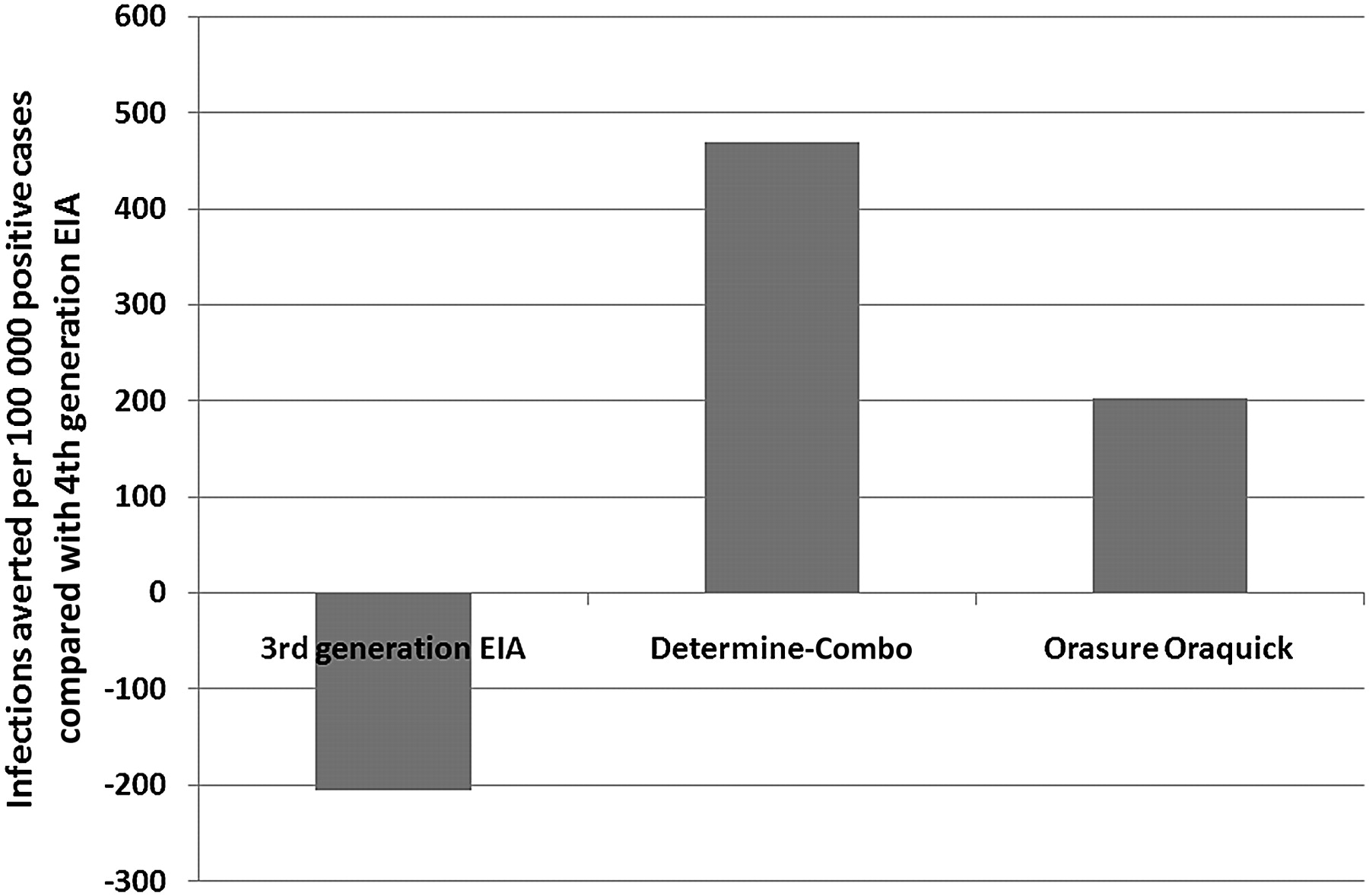
The average number of HIV transmissions per person that would result from the period between individuals being tested and receiving their results with conventional tests is substantially less than one. However, when the different window periods are included the differences in the probability of transmission per person according to different diagnostic tests may have a noticeable effect at the population level. Relative to the fourth generation conventional EIA test, the average person will cause 0 (median, 0…0.0019, 95% CI) additional infections for the third generation conventional EIA test, −0.0045 (median, −0.0253 −0.0001, 95% CI) fewer infections for the Determine-Combo rapid test and −0.004 (median, −0.025…0.183) fewer infections for the Orasure Oraquick rapid test. According to the mathematical transmission model, use of the third generation conventional EIA test would result in an extra 206 (median, 174–236 IQR from uncertainty analyses) infections per 100 000 HIV-positive people compared with the fourth generation conventional EIA test but the Determine-Combo rapid test would avert 469 (397–538) infections per 100 000 cases and the Orasure Oraquick rapid test would avert 202 (171–231) infections per 100 000 cases compared with the fourth generation conventional EIA test (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Estimated number of infections averted per 100 000 HIV-positive cases detected using the conventional third generation enzyme immunoassay (EIA) test, Determine-Combo rapid test or Orasure Oraquick rapid test compared with the conventional fourth generation EIA test.
Discussion
In this study, we found that the introduction of rapid HIV testing into a clinical service that is already using fourth generation conventional testing would only have a marginal effect on further HIV transmission between men. In Australia with about 1000 HIV diagnoses among MSM per year, one infection would be averted every 2 years by using the Determine-Combo rapid test and about one infection would be averted every 5 years by using the Orasure Oraquick rapid test compared with the fourth generation conventional EIA test. This result is influenced by our assumptions of some reduction in risk behaviour upon diagnosis; specifically, we assumed an average 20% decrease in potential transmission events (with a range of 10% increase to 50% decrease). Our qualitative results hold independently of this assumption but if risk behaviour changes by a different amount after diagnosis, then the average time between infections averted would be scaled accordingly. A key qualitative finding from this model is that we would not expect any major benefit in terms of reducing HIV transmission from men who attend this clinical setting but importantly nor would we expect more HIV transmissions due to longer window periods associated with rapid testing. Hence, the major benefit of rapid HIV testing in our setting, where few MSM detected with HIV failed to return for their result, would lie in the reduction in waiting time an individual would experience. In addition, the availability of rapid HIV testing may encourage greater coverage and increased frequency of testing for HIV among priority population groups, which may significantly reduce further transmission.
A strength of our modelling analysis is that it simulated events at an individual level, which accommodates the large heterogeneity that exists and the occurrence of relatively rare events in a population. The model was also directly informed by detailed individual line data from a large sexual health centre. However, as with all models, our simulation framework is a simplistic abstraction of reality. While the difference in time to HIV detection between the diagnostic tests is dependent on testing frequency (and thus time from infection to receiving a test), time from test to delivering the test result and test sensitivity, modelling rates of sexual transmission can be highly complex. We used a simple risk equation to estimate the average (static) risk of transmitting infection and based this on the best data available on viral load (from men at the time they were diagnosed at the MSHC) and international studies on rates of transmission. The introduction of rapid tests is likely to increase testing rates. However, in this analysis we conservatively assumed that testing rates remain unchanged. It is important to note that if the interval between regular tests decreases substantially then differences in window periods would become more important. We also acknowledge the limitation of assumed homogeneity in risk behaviour among MSM who are positive. While men who become HIV-positive are more likely to engage in similar high transmission-related risk behaviours than the risk behaviours of all MSM, there is heterogeneity in their sexual behaviours that have the potential for onward transmission. Due to the small numbers of acts involved in the estimated period of difference between the diagnostic tests, the risks of transmission are minimal. Our estimates provide an indication of the order of magnitude of the difference in expected transmissions, namely, in the Australian context one infection may be averted approximately every 2 years on average with the use of rapid tests compared with conventional tests. Incorporation of greater heterogeneity in risk behaviour may more accurately estimate the numbers of related transmissions but we do not expect this estimate to change substantially.
A limitation of this study is that the results are only applicable in similar clinical settings. Testing frequencies differ for men who do not have repeat HIV tests in similar clinical settings and our quantitative results cannot be extrapolated to other population groups or to other HIV testing environments. Only 1% of MSM diagnosed at the MSHC failed to be informed of their positive result. However, the impact of rapid testing in terms of HIV transmission could be different if there were a significantly higher proportion of men diagnosed with HIV who did not return for their result. Additionally, our model assumed that there is a uniform distribution of time from infection to testing. However, some gay men may test in response to known exposure or unprotected sex. The use of a uniform distribution in the model would, if some testing is motivated by risk, perhaps bias results in favour of the fourth generation conventional EIA test with its shorter window period.
The results of the model are dependent on assumptions around the window period chosen for the rapid and conventional tests. There are few data on precise window periods or sensitivities of the various diagnostic tests versus likely time since infection. We made assumptions of increased sensitivity and relative differences between the tests based on the best information available to us. We elected to include performance characteristics of conventional fourth generation EIAs as the baseline standard since an estimated 85% of all HIV tests performed in Australia are with these assays. In clinical settings where third generation EIAs are used, the difference in window periods between conventional serological testing and rapid tests would be smaller, changing results in favour of rapid testing. At the time of writing, no rapid HIV tests are approved for clinical use in Australia.
The diagnosis of HIV has clear benefits for HIV-infected individuals as well as the population. Rapid tests have a large potential to increase uptake of HIV testing, as demonstrated by increases in testing of 40% in the USA.7 32 In 2003, there was an estimated 25% of men with HIV infections in the USA who were unaware of their status,33–35 and 28% in the UK.36 While the rates of HIV testing among MSM in Australia are higher than among MSM in other industrialised countries,37 data suggest up to 20% of all infections remain undiagnosed.38 Rapid testing may be useful in maintaining the current high levels, encouraging uptake of testing among men who remain untested or increasing the frequency of testing among men most at risk of infection.39 40 Consequently, encouraging further uptake of testing to decrease the proportion of people who are undiagnosed is an important goal in Australia's public health effort against the HIV epidemic.
Due to their longer window period, rapid tests have not achieved adequate performance and have not been supported by the Australian Testing Policy for use as screening tests in Australia. However, Australian Testing Policy and the related assessment process conducted by the Australian Therapeutic Goods Authority and Australian National Reference Laboratory do not take into account important aspects of rapid HIV tests relevant to their use as screening tests at point of care, which in the experiences of services using them in other settings have demonstrated many public health benefits. Our study provides further evidence that the introduction of rapid tests is unlikely to do more harm than using current diagnostic tests and may have some modest additional epidemiological benefits.
If a rapid HIV test is used and it is reactive then it should be confirmed using conventional supplementary testing such as western blot or EIA tests. Ideally, this should take place at the point where a provisional reactive rapid test result is received to ensure confirmation is undertaken.41 Any programmes using rapid HIV testing should also have adequate quality controls in place and provide training for accurate interpretation of results.13 14 41 42 Since current rapid tests require longer window periods than the best laboratory EIA tests, we recommend that where rapid tests are offered, pretest discussions should carefully assess whether the client had a recent risk exposure. For clients with recent risk exposure, the most sensitive available HIV test should be recommended. This will normally mean a conventional fourth generation Ag/Ab EIA test or a proviral DNA test should be offered instead of a rapid HIV test.
The cost-effectiveness of the different diagnostic tests is also an important consideration. The unit cost of a rapid test kit is more than the cost of processing a sample in a laboratory on an EIA testing platform. However, the unit cost of processing a sample in a laboratory does not take account of the fixed costs of running a laboratory, salaries, equipment and the cost of transporting samples to the laboratory. Where rapid tests are used, most results will be HIV-negative and samples would not need to go to a laboratory, and so less laboratory capacity would be needed. Assessing the comparative cost of providing rapid HIV testing services and current HIV testing services was beyond the scope of this study. Assessment of the testing and behaviour data for men attending a large sexual health centre, through our model, predicted that there would be a small net benefit in terms of reduced new HIV transmissions as people undertaking rapid testing would learn their HIV status earlier than in the current environment and missed diagnoses would occur in a very small proportion of cases. Additional advantages of rapid HIV tests include that they are less invasive, can be used outside established clinical settings, can lead to an increased proportion of those testing receiving results, and will likely increase HIV testing coverage and frequency. As rapid HIV testing technologies have improved it appears that it is time for them to be introduced in Australian clinical settings.
Key messages
Rapid tests would result in earlier receipt of HIV results for unmissed diagnoses.
Rapid testing would probably prevent one in 2000–5000 HIV transmissions among men who have sex with men in Australia compared with fourth generation enzyme immunoassay tests.
Assuming no greater HIV testing frequency upon the availability of rapid tests, there may not be any substantial difference in HIV transmission between men associated with the use of rapid tests compared with enzyme immunoassay tests.
Acknowledgments
We wish to thank Rob Warren from the Victorian Infectious Diseases Reference Laboratory for data on HIV testing and Afrizal from the Information Technology unit at the Melbourne Sexual Health Centre for clinical data as well as other Melbourne Sexual Health Centre staff for support. The authors acknowledge funding from the Australian Research Council (DPW). The National Centre in HIV Epidemiology and Clinical Research is funded by the Australian Government, Department of Health and Ageing. The views expressed in this publication do not necessarily represent the position of the Australian Government. NCHECR is affiliated with the Faculty of Medicine at the University of New South Wales.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
Funding The authors acknowledge funding from the Australian Research Council. The National Centre in HIV Epidemiology and Clinical Research is funded by the Australian Government, Department of Health and Ageing.
Competing interests None.
Ethics approval Ethical approval for this study was granted by the Alfred Hospital Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.