Article Text

Abstract
Objectives To describe, using routine data in selected countries, chlamydia control activities and rates of chlamydia infection, pelvic inflammatory disease (PID), ectopic pregnancy and infertility and to compare trends in chlamydia positivity with rates of PID and ectopic pregnancy.
Methods Cross-national comparison including national data from Australia, Denmark, the Netherlands, New Zealand, Sweden and Switzerland. Routine data sources about chlamydia diagnosis and testing and International Classification of Disease-10 coded diagnoses of PID, ectopic pregnancy and infertility in women aged 15–39 years from 1999 to 2008 were described. Trends over time and relevant associations were examined using Poisson regression.
Results Opportunistic chlamydia testing was recommended in all countries except Switzerland, but target groups differed. Rates of chlamydia testing were highest in New Zealand. Chlamydia positivity was similar in all countries with available data (Denmark, New Zealand and Sweden) and increased over time. Increasing chlamydia positivity rates were associated with decreasing PID rates in Denmark and Sweden and with decreasing ectopic pregnancy rates in Denmark, New Zealand and Sweden. Ectopic pregnancy rates appeared to increase over time in 15–19-year-olds in several countries. Trends in infertility diagnoses were very variable.
Conclusions The intensity of recommendations about chlamydia control varied between countries but was not consistently related to levels of chlamydia diagnosis or testing. Relationships between levels of chlamydia infection and complication rates between or within countries over time were not straightforward. Development and validation of indicators of chlamydia-related morbidity that can be compared across countries and over time should be pursued.
- Chlamydia trachomatis
- pelvic inflammatory disease
- ectopic pregnancy
- infertility
- epidemiology
- surveillance
- LGV
- STD behavioural
- STD patients
- STD clinic
- STDS
- genital infection
- sexual behaviour
- STD control
- chlamydia infection
- epidemiology (general)
- screening
- general practice
- TB
- HSV-1
- HSV-2
- chlamydia
Statistics from Altmetric.com
- Chlamydia trachomatis
- pelvic inflammatory disease
- ectopic pregnancy
- infertility
- epidemiology
- surveillance
- LGV
- STD behavioural
- STD patients
- STD clinic
- STDS
- genital infection
- sexual behaviour
- STD control
- chlamydia infection
- epidemiology (general)
- screening
- general practice
- TB
- HSV-1
- HSV-2
- chlamydia
Introduction
There is ongoing debate about the long-term effectiveness of chlamydia screening as a public health intervention.1–4 Chlamydia trachomatis is the most commonly reported sexually transmitted infection in Europe5 and can cause female pelvic inflammatory disease (PID), ectopic pregnancy and tubal infertility.6 Randomised controlled trials have suggested that screening for chlamydia can prevent PID in the subsequent year at the individual level.7–9 The impact on ectopic pregnancy and infertility has not been studied in randomised trials.10
Within individual countries, trends in chlamydia have been compared with rates of hospitalisation for PID and ectopic pregnancy, with declining levels of both conditions from the mid-1980s to the mid-1990s in the USA and Sweden, at around the time when chlamydia control measures were introduced.11 12 More recently, discordant trends between chlamydia surveillance data and PID hospitalisation rates have been observed in Australia13 and the USA.14 Cross-national comparisons of routine data sources are another method for examining information about population-level associations between interventions and clinical outcomes.15 The objectives of this cross-national study were to describe, using routine data in selected countries, chlamydia control activities and rates of chlamydia infection, PID, ectopic pregnancy and infertility and to compare trends in chlamydia positivity with rates of PID and ectopic pregnancy.
Methods
We selected countries purposively according to demographic, economic and social indicators, chlamydia testing practices, infection rates and availability of data. Australia, Denmark, the Netherlands, New Zealand, Sweden and Switzerland are all high-income industrialised democracies with healthcare systems with universal access. Denmark, New Zealand, Sweden and Switzerland have small populations (4.4–9.3 million). Australia and the Netherlands are somewhat larger (22.5 and 16.5 million, respectively). We collected disease data at country level from Australia, Denmark, the Netherlands, Sweden and Switzerland. For New Zealand, data were available for six of 20 district health boards covering 48% of the total population (Auckland, Bay of Plenty, Counties Manukau, Lakes, Waikato and Waitemata). The years for which we could obtain comparable data for most countries were 1999–2008. Details of data sources and coverage are described in detail in Supplementary table 1 (online).
Chlamydia control activities
We collated information about chlamydia control activities from Denmark, the Netherlands, Sweden and Switzerland using a tool developed for a European project in 2007.16 17 The same information about activities in Australia and New Zealand was provided by coauthors. We obtained the numbers of chlamydia cases from official databases (online Supplementary table 1). For the Netherlands, two data sources were combined; diagnoses in all sexually transmitted infection clinics and extrapolated numbers of cases ascertained in a representative sample of general practices covering 2% of the general population.18 We also obtained laboratory data about the total (not stratified by age or sex) numbers of chlamydia tests performed each year for Denmark, New Zealand and Sweden. Chlamydia test data for Australia covered only general practice and for the Netherlands only sexually transmitted infection clinics. Chlamydia test data were not available for Switzerland.
Chlamydia-associated reproductive tract morbidity
We selected International Classification of Disease codes (ICD-9 or 10) to identify main diagnoses of PID, ectopic pregnancy and infertility from any cause. The codes included were those used in a previous study19 (online Supplementary table 2), with the exception that chlamydial female PID was coded as A56.1 in New Zealand (and N74.4 in other countries using ICD-10). Data were obtained from national hospital registries (online Supplementary table 1), which included public and private hospitals for Australia, Switzerland and Sweden and public hospitals in Denmark, the Netherlands and the six districts of New Zealand. We included both episodes including an overnight stay and those treated as day cases, if available. Data from Denmark and Sweden included only overnight cases. Using data from Australia and Switzerland that presented overnight and day cases separately, we examined the possible degree of underestimation: 10%–20% of ectopic pregnancy episodes were treated as day cases; PID case management was more variable, with day cases accounting for an average of 5% additional cases in Switzerland and 80% in Australia.
Denominator data
We used publicly available data about midyear population estimates of the numbers of women aged 15–39 years in each country and year. For countries with chlamydia testing data, we used the midyear population estimate for the total population in each year. For ectopic pregnancy, the numbers of live births for each age group were used as the denominator to take into account differences between countries in fertility rates.
Statistical analysis
For chlamydia diagnoses, PID and infertility in each country in every year, we calculated rates per 100 000 for all women aged 15–39 years and in 5-year age bands. Data from Australia were based on a financial year (July to June) and are presented in the same calendar year as the start of the financial year. Overall rates were age standardised by the direct method using the European standard population. For ectopic pregnancy, we calculated rates per 1000 live births. For relevant countries, we used total numbers of chlamydia tests to calculate rates per 100 000 total population and rates of chlamydia positivity per 100 tests. For data on all outcomes from New Zealand and chlamydia case data from the Netherlands, which were based on a sample of the population, we calculated 95% CIs for each rate. For all other countries and outcomes, the case counts represented all diagnoses made in the total population of each country so CIs were not calculated.
We used Poisson regression models to explore time trends and examined evidence for compatibility of the observed data with both linear and quadratic functions. For trends in overall rates of each condition between countries, we used random effects models and examined statistical evidence for an interaction between country and year, based on likelihood ratio tests (described in Supplementary text online). For analyses of trends in rates according to age group within countries, we used ordinary Poisson regression models with interaction terms. We conducted limited analyses of associations between chlamydia positivity and complication rates because the positivity rates could not be stratified by age. We examined associations with PID rates among women aged 15–39 years in the same year and with ectopic pregnancy rates in the same year and for lags of up to 5 years later using Poisson regression to estimate the rate ratio (RR) for a 1% change in chlamydia positivity. All analyses were conducted using STATA V.11 (StataCorp., 2009).
Results
Chlamydia control activities
All countries except Switzerland had guidelines about the case management of chlamydia and recommendations about chlamydia testing that were endorsed by governmental or professional bodies (table 1).
Country characteristics, surveillance practice and recommendations for chlamydia case management, testing and screening
Recommendations about opportunistic chlamydia testing of asymptomatic individuals ranged from testing only of those with risky sexual behaviour or in specific clinical situations in Denmark to testing for wide groups such as sexually active under 25-year-olds in Australia, the Netherlands and New Zealand. In most study countries, chlamydia was diagnosed throughout the study period using nucleic acid amplification tests.
Chlamydia diagnosis, testing and positivity
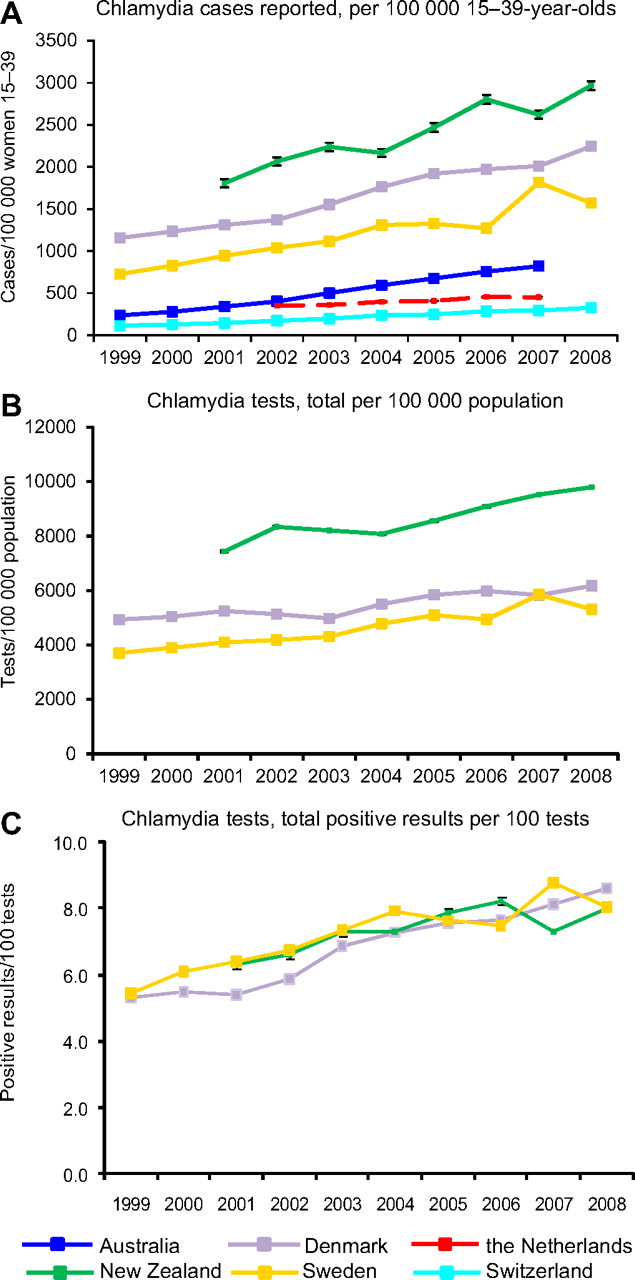
The rate of reported diagnosed chlamydia cases increased in all countries over time (figure 1A). The highest rates were in the six districts of New Zealand, Denmark and Sweden. In the three countries with data about chlamydia testing and positivity rates for the population as a whole, testing rates were highest in the six districts of New Zealand (9801 per 100 000 population in 2008), followed by Denmark and Sweden (6175 and 5309 per 100 000 population in 2008, respectively) (figure 1B). The percentages of chlamydia tests with positive results were very similar in all three countries and increased steadily over the study period (figure 1C). When stratified by age (online Supplementary figure 1), trends differed according to age group in all countries (p≤0.001).

Trends in chlamydia diagnosis rates, testing rates and percentage of chlamydia test with a positive result, 1999–2008. (A) Chlamydia diagnoses per 100 000 women 15–39 years, age standardised. (B) Total chlamydia tests per 100 000 population; (C) positive tests per 100 chlamydia tests performed in total population. Data from laboratory-based reporting, except for the Netherlands (dashed line), which include all cases from sexually transmitted infection clinics plus cases extrapolated from sentinel general practice clinics (95% CIs shown but are very narrow). Data from New Zealand are from six counties and are shown with 95% CIs.
Chlamydia-associated complications
Overall rates of PID diagnosed in hospitals varied about threefold between countries, with the highest rates in New Zealand (193.7 per 100 000 women in 2008), Denmark (106.0 per 100 000 women in 2004) and Australia (88.8 per 100 000 women in 2007) and the lowest in Sweden (37.1 per 100 000 women in 2008) (figure 2A). In all study countries, the lowest PID rates were reported for the youngest age group, except in New Zealand where rates in 15–19-year-olds appeared to increase and were the highest of all age groups from 2005 to 2008 (figure 2E). Rates of PID in women of all ages combined were negatively associated with the overall rate of positive chlamydia tests in Denmark (RR 0.79, 95% CI 0.75 to 0.84) and Sweden (RR 0.86, 95% CI 0.84 to 0.88). There was no association between overall PID and chlamydia positivity in New Zealand (RR 1.05, 95% CI 0.96 to 1.15).

Rates of hospitalisation for pelvic inflammatory disease (PID), 1999–2008. (A) PID rate per 100 000 women aged 15–39 years, by country, age standardised. (B–G) PID rate in each country per 100 000 women, by age group. Sweden and Denmark (dashed lines) include only overnight hospitalisations; all other countries (solid lines) include both overnight and day cases. New Zealand includes data from six counties and are shown with 95% CIs.
Ectopic pregnancy rates varied by twofold or less between study countries (figure 3A). The highest rate was in New Zealand (17.5 per 1000 live births in 2008) and the lowest in the Netherlands (10.1 per 1000 live births in 2008). Age-specific trends in ectopic pregnancy rates differed between countries (figure 3). In the countries with available data, rates of overall chlamydia positivity were negatively associated with ectopic pregnancy rates in all three countries in all age groups combined. When time lags were introduced, trends in chlamydia rates continued to be negatively associated with ectopic pregnancy rates for up to 4 years later. In analyses of overall chlamydia positivity and ectopic pregnancy rates in 15–19-year-olds in the same year, a positive association was observed in New Zealand (RR 1.16, 95% CI 1.03 to 1.33) but not in Denmark (RR 1.09, 95% CI 0.95 to 1.25) or Sweden (1.05, 95% CI 0.98 to 1.13). Observed rates of ectopic pregnancy in 15–19-year-olds also increased in the Netherlands and Switzerland.

{kind=link}
{kind=link}
{kind=link}
Rates of hospitalisation for ectopic pregnancy, 1999–2008. (A) Ectopic pregnancy rate per 1000 live births in women aged 15–39 years, by country, age standardised. (B–G) Ectopic pregnancy rate in each country per 1000 live births, by age group. Sweden and Denmark (dashed lines) include only overnight hospitalisations; all other countries (solid lines) include both overnight and day cases. New Zealand includes data from six counties and are shown with 95% CIs.
Rates of hospital-diagnosed infertility between countries varied widely and trends over time differed (p<0.001). Age-specific diagnosis rates are shown in Supplementary figure 2 (online).
Discussion
In this cross-national study from 1999 to 2008, all participating countries except for Switzerland recommended opportunistic chlamydia testing in at least one group of asymptomatic women. Chlamydia diagnosis rates were available in all countries, but numbers of tests were only available in three countries and were not stratified by age. Chlamydia testing rates were highest in New Zealand. In Denmark, New Zealand and Sweden, chlamydia positivity proportions were very similar and increased in all three countries. PID rates were highest in New Zealand and lowest in Sweden. Rates of chlamydia positivity were negatively associated with PID rates in Denmark and Sweden but not in New Zealand. Rates of ectopic pregnancy were highest in New Zealand and lowest in the Netherlands. In Denmark, New Zealand and Sweden, rates of chlamydia positivity were negatively associated with ectopic pregnancy rates in the following year and for up to 4 years later.
Strengths and weaknesses
The main strength of this study was that we were able to obtain time trend data from six countries of similar social and economic status about measures of chlamydia surveillance and control activities and about levels of diagnosed infection and reproductive tract consequences managed in hospital. Age standardisation allowed comparisons that adjusted for differences in age structure between countries. In fact, there was very little difference between age-standardised and crude rates and the rankings of countries did not change. The main limitation of an ecological study is that we cannot make causal inferences from comparisons of aggregated data about associations at the level of the individual.23 There were some limitations in the comparability of the data available, but these did not consistently account for between-country differences in rates of morbidity. Chlamydia cases were obtained from laboratory-based reporting in five of six countries, and data were judged by coauthors to be largely complete. Ascertainment in the Netherlands was the least certain; two separate data sets were combined, and there were possible sources of either under- or overestimation.18 Hospitalisations were obtained from national registries in all countries. In Denmark and Sweden, only visits including an overnight stay were available and the proportions of women treated as day cases were not known. Including day cases would not change the interpretation of relative trends between these countries, however. Even assuming 80% underestimation, PID rates in Sweden would still be among the lowest and rates in Denmark would be the highest. There are few private hospitals in Denmark, the Netherlands and New Zealand so their exclusion would not alter the results. We could not examine differences in sexual behaviour between the study countries as a factor contributing to differences in reproductive tract morbidity because of a lack of comparable data.
Comparison with other studies
We believe this to be the only study examining chlamydia-related morbidity in such a range of countries. Trends in rates of chlamydia and associated morbidity ascertained mainly from routine data sources have been examined in single countries.11–13 24 In this study, similarities and differences between countries could be examined. Chlamydia diagnosis rates increased in all countries, and in countries with available data, this reflected increases in testing. A novel finding was the striking similarity in the percentage of positive chlamydia tests over time in Denmark, New Zealand and Sweden, which might indicate similar levels of chlamydia in these populations, despite differences in chlamydia testing rates.
For ectopic pregnancy, a study from 1985 to 1995 found that falling ectopic pregnancy rates in 20–24-year-old Swedish women were associated with chlamydia positivity rates in the same year but that there were time lags at older ages, suggesting an important role for recent chlamydia infections in ectopic pregnancy in women under 25 years.11 In this study, analyses were limited because chlamydia test data were only available for some countries and the available test data were not age stratified. In the youngest age group, ectopic pregnancy cases are rare but appeared to increase in several countries.
Interpretation of the findings
In this cross-national study, tracking long-term trends in routinely available surveillance and hospital episode statistics did not help determine straightforward relationships between chlamydia control activities, levels of chlamydia infection and complication rates. Based on the phase of the epidemic and its control,25 three types of relationships could be hypothesised: first, in the absence of control measures, chlamydia infection rates might be high but undetected (seen as low diagnosis rates) and complication rates would also be expected to be high or be increasing. Second, with sufficiently high levels of screening, detection rates would be high and chlamydia positivity (if a proxy for prevalence) and complication rates would be expected to fall. Between these extremes, increasing levels of case detection could co-exist with high levels of complications, but positivity would be expected to fall over time either as a result of testing more low-risk individuals or controlling transmission. Switzerland is an example of a country with no specific chlamydia control measures; indeed, the lowest rates of diagnosed chlamydia suggest low rates of case detection. Complication rates, with high levels of ascertainment, were not among the highest, however, and PID and ectopic pregnancy rates declined over time. There were three countries with high, and increasing, chlamydia detection and positivity rates. In Denmark and New Zealand (but not Sweden, even allowing for underestimation), PID and ectopic pregnancy rates were high. PID rates, however, fell in both young and older women in Denmark and Sweden and appeared to increase in 15–19-year-olds in recent years in New Zealand women. Overall ectopic pregnancy rates fell in all three countries. These three countries might be at different epidemic phases, with different patterns reflecting more recent introduction of screening recommendations in New Zealand than in Sweden and Denmark. Such an explanation is consistent with some between-country trends but not with the very similar patterns in chlamydia positivity rates in all three countries over time.
It is possible that trends in all-cause hospitalisation for PID, ectopic pregnancy and infertility are not sensitive or specific enough to reflect changes in chlamydia infection rates. For PID, the fall in hospitalisation rates was initially thought to reflect shifting management trends from secondary care.13 However, PID rates in primary care have also fallen in several countries14 26 27 (and Supplementary figure 3 online) so the other factors contributing to this need to be investigated. No country in this study had high chlamydia detection rates and falling positivity and complication rates. A further possibility is, therefore, that chlamydia control activities have not been implemented intensively or regularly enough in any country to have affected the prevalence of chlamydia or the incidence of reproductive tract complications.1
The extent to which the percentage of positive chlamydia tests can represent population prevalence remains uncertain since this measure is strongly influenced by changes in the numbers and characteristics of those being tested.3 Increasing positivity rates, seen in Denmark, New Zealand and Sweden in this study, have been observed in sexual health clinic attenders in Australia.28 These trends, however, differ from prevalence trends from the US National Health and Nutrition Examination Surveys which have been stable or slightly decreasing since 1999.29
Implications for research, practice and policy
The impact of public health prevention programmes should be monitored with reliable and valid indicators that can, ideally, be collected routinely and compared internationally. Repeated population-based surveys of chlamydia prevalence, like the US National Health and Nutrition Examination Surveys,3 29 should be used to monitor the impact of chlamydia control activities where controlling chlamydia transmission is an objective. Monitoring the intensity of chlamydia testing requires information about both frequency of testing and positivity. Data are increasingly available from record systems that can track individuals longitudinally30 and across clinical settings31 but are not currently available in routine surveillance. Data about the numbers of partners of chlamydia cases, as collected in the English chlamydia screening programme, can also aid interpretation.32 The level, frequency and mode of implementation of chlamydia screening and management required to effect a quantifiable reduction in chlamydia prevalence or reproductive tract morbidity still need to be determined, however.10 Results are keenly awaited from randomised evaluations of systematic register-based screening in the Netherlands21 and of opportunistic screening in Australia,20 which will measure changes in chlamydia prevalence over multiple screening rounds, with PID as a secondary outcome. Levels of PID diagnosis are already monitored to assess trends in sexual health in the USA, despite acknowledged diagnostic limitations.14 The utility of data about chlamydia-associated complications could be improved with updated estimates of the proportions of PID, ectopic pregnancy and infertility cases due to chlamydia and collation of both in-patient and out-patient/primary care sources of data. Studies of the role of chlamydia at the time of ectopic pregnancy diagnosis in 15–19- and 20–24-year-old women would also be valuable as this might be a future indicator of levels of complicated chlamydia in larger countries. In summary, this study demonstrates some of the complexities of meaningful analyses of routinely available national surveillance data to estimate the long-term impact of chlamydia control activities. Further analyses that focus on comparable data from cohorts of women and include cohorts with higher testing rates might provide more insights. Development and validation of indicators of chlamydia-related morbidity that can be compared across countries and over time should be pursued.
Key messages
There is marked variation between countries in descriptions of chlamydia control activities, reported rates of chlamydia and hospital-diagnosed episodes of chlamydia-associated reproductive tract morbidity.
Tracking long-term trends in surveillance and hospital episode data did not help determine straightforward relationships between the changes in levels of chlamydia infection and all-cause hospitalisation rates for pelvic inflammatory disease, ectopic pregnancy and infertility.
Development and validation of indicators of chlamydia-related complications that can be compared across countries and over time should be pursued.
Acknowledgments
We acknowledge R. A. Verheij and colleagues from the Dutch National Institute for Health Services Research (NIVEL, Utrecht, NL) for their input in providing data from the Dutch GP surveillance network.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.