Article Text

Abstract
The authors report a case of an inguinal bubo in a young man caused by an anaerobe, Prevotella bivia, which was acquired during oral sexual intercourse. As far as the authors know, this is the first reported case of a sexually transmitted infection by Prevotella. Prevotella spp. inhabit the oral cavity and are highly prevalent in bacterial vaginosis, a polymicrobial syndrome resulting from replacement of the normal vaginal Lactobacillus spp. flora by high concentrations of anaerobic microorganisms such as Prevotella spp., Mobiluncus spp., Gardnerella vaginalis and other uncultivated anaerobes.
- Inguinal bubo
- prevotella
- anaerobe sexually transmitted infections
- human bite
- oral sex
- infectious diseases
- penis
- AIDS
- balanitis
- chlamydia infection
- genital ulcers
Statistics from Altmetric.com
- Inguinal bubo
- prevotella
- anaerobe sexually transmitted infections
- human bite
- oral sex
- infectious diseases
- penis
- AIDS
- balanitis
- chlamydia infection
- genital ulcers
Case report
A 34-year-old man presented to our department with a 5-day history of a painful mass in the left groin (figure 1). He had been treated with ciprofloxacin and doxycycline for 3 days without any improvement. His past medical record was unremarkable without any previous sexually transmitted infection (STI) or genital ulcer, but he reported unprotected sexual intercourse with a woman 48 h prior to the appearance of the symptoms.

Warm, tender and fluctuant mass at the left inguinal region (red circle).
Physical examination revealed an erythematous, warm, tender and fluctuant mass, 5×2 cm in diameter, in the left inguinal area. This mass was extremely painful on palpation. No genital, anal or perianal ulcers were observed, and no associated urethral symptoms were present. A detailed exam of the penis and scrotum was also normal.
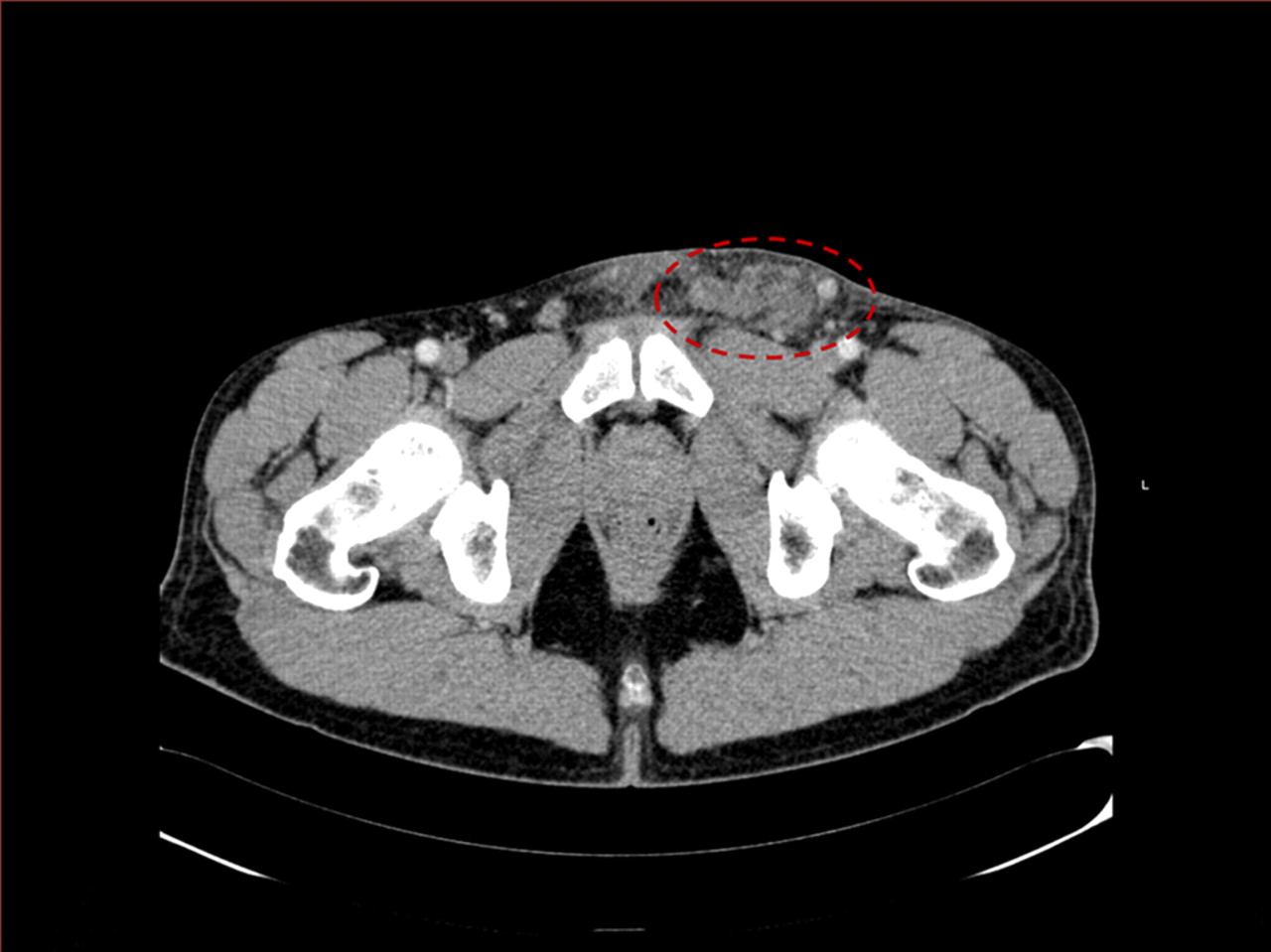
Inguinal ultrasound studies showed a hypoechoic subcutaneous mass and ruled out testicular or epididimal abnormalities. An abdominal–pelvic CT scan disclosed several enlarged lymph nodes at the left inguinal region (figure 2), one of them showing fistulisation to the subcutaneous tissue. No other abdominal masses were detected.

{kind=link}
{kind=link}
CT pelvic scan: enlarged lymph nodes at the left inguinal region with subcutaneous fistulisation (red circle).
Serological testing for syphilis (treponema pallidum hemagglutination assay (TPHA) and rapid plasma reagin (RPR)), HIV and Chlamydia trachomatis was negative. Since antibiotic treatment had proven unsuccessful, incision and drainage were performed. The foul-smelling purulent exudate obtained was tested for C trachomatis by real time PCR (COBAS® TaqMan® CT Test V.2.0; Roche Diagnostics, Mannheim, Germany) which was negative. Drainage specimen was collected in sterile phial and was inoculated in Columbia CNA agar plate, Chocolate PoliVitex agar plate, Amikacin blood agar plate and Schaedler enriched with 5% of sheep blood agar plate (BioMérieux) and into BBL enriched thioglycolate medium with vitamin K and haemin (Becton Dickinson and Company, London, UK). The cultures were incubated at 37°C for 5 days. The Amikacin and Schaedler agar plates were incubated at 37°C in anaerobiosis for 5 days. Microorganism was identified by using routine microbiological techniques. Anaerobic bacterial culture was positive for Prevotella bivia, whereas the aerobe and Lowenstein culture were negative. The diagnosis of inguinal bubo caused by P bivia was established. The patient received amoxicillin/clavulanate at a dosage of 875/125 mg every 8 h for 10 days after drainage, with no recurrence of the symptoms.
In the next visit, considering the isolation of P bivia in the bubo, and after a more detailed and directed questioning, the patient admitted that he had been bitten in the glans during his last sexual intercourse. That penile injury caused a discrete haemorrhage. It was not possible to contact his sex partner.
Discussion
Inguinal syndrome is defined by the presence of painful, unilateral, inguinal or femoral enlarged lymph nodes, possibly with buboes.1 Lymphogranuloma venereum and chancroid are STI classically producing painful suppurative inguinal adenitis. However, other microorganisms such as Treponema pallidum, herpes simplex, Bartonella hanselae (cat-scratch disease), atypical mycobacteria and some non-infectious disorders have also been incriminated as potential causative agents for inguinal syndrome.
In 1996, Viravan et al reported a series of 113 patients with inguinal bubo who attended a STI clinic in Bangkok between 1987 and 1989. The most frequent aetiological agent was Haemophilus ducreyi followed by C trachomatis.2 The outbreak of lymphogranuloma venereum (LGV) in large cities of Europe and America has to be taken into account in the management of the inguinal syndrome. In a review of LGV cases in London in men who have sex with men, three cases out of 13 displayed an inguinal bubo without penile or rectal ulcer.1 In our case, negative results of C trachomatis PCR tests performed in urine and in the purulent exudate ruled out the diagnosis of LGV. Treatment with doxycycline and ciprofloxacin would have been of benefit in the majority of STI. However, in our case, they failed as they have a poor antianaerobic activity.
Prevotella DNA has been detected in the human vaginal epithelia in 40% of healthy women, with a higher proportion in women with bacterial vaginosis.3 It has also been detected in the glans. Some authors have related the presence of Prevotella in men to BV in their sexual partners.4 In the case presented here, a potential vaginal transmission cannot be completely excluded. However, the traumatic event (human bite) during orogenital sex seems to be the inoculation site of infection giving rise to suppurative inguinal adenitis.
Prevotella spp. inhabit the digestive tract from the oral cavity to the anus.5 They are considered a common causative agent for infections secondary to animal and human bites. Human and animal bites are usually polymicrobial, anaerobes being isolated from more than two-thirds of human and animal bite wound infections, especially those associated with abscess formation.6
Genital human bite wounds causing penile infected ulcers have been previously described, with Eikenella corrodens being the infective agent most frequently isolated.7 8 A case of a penile abscess due to P bivia has been previously described, but the pathogenesis of the infection could not be cleared out.9 Other reports of inguinal phlegmon after penile bites have been reported.10 However, as far as we are concerned, no previous cases of inguinal syndrome secondary to orogenital contact caused by P bivia have been reported. Apart from the well-known causes of inguinal syndrome, this agent should be added to the list of putative aetiological agents and considered when dealing with inguinal buboes developing after orogenital sex, especially when a traumatic event is recorded.
Key messages
Anaerobes such as Prevotella bibia can be the aetiological agent of inguinal buboes.
Diagnosis requires appropriate cultures.
Its innoculation was related to a traumatic event (human bite) during orogenital sex.
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.