Article Text

Abstract
Objectives The borderlands are considered areas of increased vulnerability to HIV and sexually transmitted infections (STI). The study aimed to determine the STI/HIV prevalence and risk factors in the triple-border area of the Brazilian Amazon.
Methods A situational analysis of sexual health was conducted in three cities of the Alto Solimões region. This multicomponent research approach included key informant interviews, participant observations and mapping of places where people meet sexual partners. Volunteers recruited from the ‘hot spots’ in each city were invited for interview and STI/HIV testing.
Results Over 6 months, 598 participants were recruited, 285 men of median age 28 years (IQR, 23–37) and 313 women of median age 29 years (IQR, 24–37). Overall, 49.3% reported a casual partner during the past 3 months, but only 38.5% reported consistent condom use. The respective prevalences in men and women were Neisseria gonorrhoeae (1.1% and 0.3%), Chlamydia trachomatis (1.4% and 4.8%), high-risk human papillomavirus (14.4% and 24.0%), active syphilis (3.2% and 2.6%), herpes simplex virus type-2 (51.1% and 72.1%), hepatitis B virus (by hepatitis B virus surface antigen) (7.5% and 4.6%), hepatitis C virus (0.7% and 0.7%) and HIV (1.4% and 0.0%). Risk factors for viral STIs included female sex and age.
Conclusions While the main conditions that contribute to the spread of HIV are in place in the triple-border area, the prevalence of bacterial STIs and HIV are still relatively low, providing a window of opportunity for interventions.
- HIV
- sexually transmitted infections
- rapid assessment methods
- sexual behaviour
- measurement
- risk factors
- vulnerable groups
- Brazil
- transmission dynamics
- syphilis
- syndromic management
- sexual health
- HIV testing
- sexual health hepatitis
- epidemiology (general)
- epidemiology (clinical)
- evidence-based medicine
- RTI
- STD control
- HSV-2
- epidemiology
Statistics from Altmetric.com
- HIV
- sexually transmitted infections
- rapid assessment methods
- sexual behaviour
- measurement
- risk factors
- vulnerable groups
- Brazil
- transmission dynamics
- syphilis
- syndromic management
- sexual health
- HIV testing
- sexual health hepatitis
- epidemiology (general)
- epidemiology (clinical)
- evidence-based medicine
- RTI
- STD control
- HSV-2
- epidemiology
Introduction
The borderlands are often considered areas of increased vulnerability of populations to HIV and other sexually transmitted infections (STI).1 2 These areas are characterised by widespread cross-border movement of people. Population mobility might distribute infection spatially and has been consistently related with high-risk behaviour, including multiple partnerships and sex work.3 Yet, there is often little information available on the epidemiology of STI/HIV in the most at-risk groups in many of these areas, thereby limiting the implementation of STI/HIV prevention interventions. The Amazonian triple-border area is no exception. Set between Indian reservation territories, it brings together indigenous groups and riverine populations of Brazil, Peru and Colombia into close contact with sex workers, male migrant workers, army personnel and insurgencies.4 The region is considered a principal entry point for drug trade and contraband into Brazil. It is a remote region practically inaccessible by road, with limited governmental structures and regulation and weak health services.5 Recent surveillance data among pregnant women in the area indicate an HIV prevalence of 0.1% and a syphilis prevalence of 1.3%,6 but information is lacking on the epidemiology of STI/HIV and on which groups or locations should be targeted by prevention efforts.7 8 A situational analysis was undertaken to provide policy-makers and planners with quality context-specific information to improve sexual and reproductive health and to prevent the spread of STI/HIV.
Different methodologies generate information useful for STI/HIV programme planning and monitoring. The Priorities for Local AIDS Control Efforts (PLACE) method characterises public venues where people meet new sexual partners,9 10 whereas other types of situational analyses define the target population(s) based on high-risk group (self-) identification. The present study was part of a comprehensive situational analysis of sexual health (SASH) conducted in the Alto Solimões region of the Brazilian State of Amazonas. The SASH is a semi-rapid, participatory and multi-component approach that uses a set of standardised methods and techniques to identify, approach and collect data from all possible vulnerable or at-risk populations in a particular locale.11 The aim of the study was to determine the prevalence and determinants of HIV and other STIs in three municipalities of the triple-border area in Alto Solimões.
Methods
Study setting
The study was conducted from February to July 2009 in three cities of the triple-border area. Tabatinga (population 52 279) shares a land border with the Colombian city of Leticia and is connected by the Solimões river with Manaus (Brazil) and Iquitos (Peru). The city is an important commercial centre for the region and a cross-road/river for traders, travellers, migrants, indigenous groups and armed forces from the three countries. Benjamin Constant (population 33 391, 18 km from Tabatinga) is situated on the riverine border with Peru and only accessible by boat. Atalaia do Norte (population 15 149, 67 km from Tabatinga) is the westernmost city of the State of Amazonas, houses the State headquarters of the Indigenous health authority (SESAI) and gateway to access isolated indigenous communities.
General methodological approach
The SASH methodology aims to provide, in a relatively short space of time and at relatively low-cost, information on the social, cultural, behavioural, clinical and epidemiological aspects of HIV and STIs, which are needed to make an overall assessment of the situation and to identify priorities and assist in developing effective STI/HIV control interventions. Therefore, the SASH methodology is particularly well-suited for use in Alto Solimões, where little is known on the nature and size of sexual health problems of the various target populations and where urgent interventions are required.
The SASH approach used in Alto Solimões was a modification of the original methodological package developed and used in India and China.11 The SASH requires an interdisciplinary team that combines qualitative and quantitative methods to obtain complementary and mutually validating findings on sensitive information from various groups and places.12 Data are triangulated to ensure a greater validity of the findings. This action–research programme is based on the strong participation of local stakeholders in order to enable them to identify relevant issues and develop subsequent action plans.
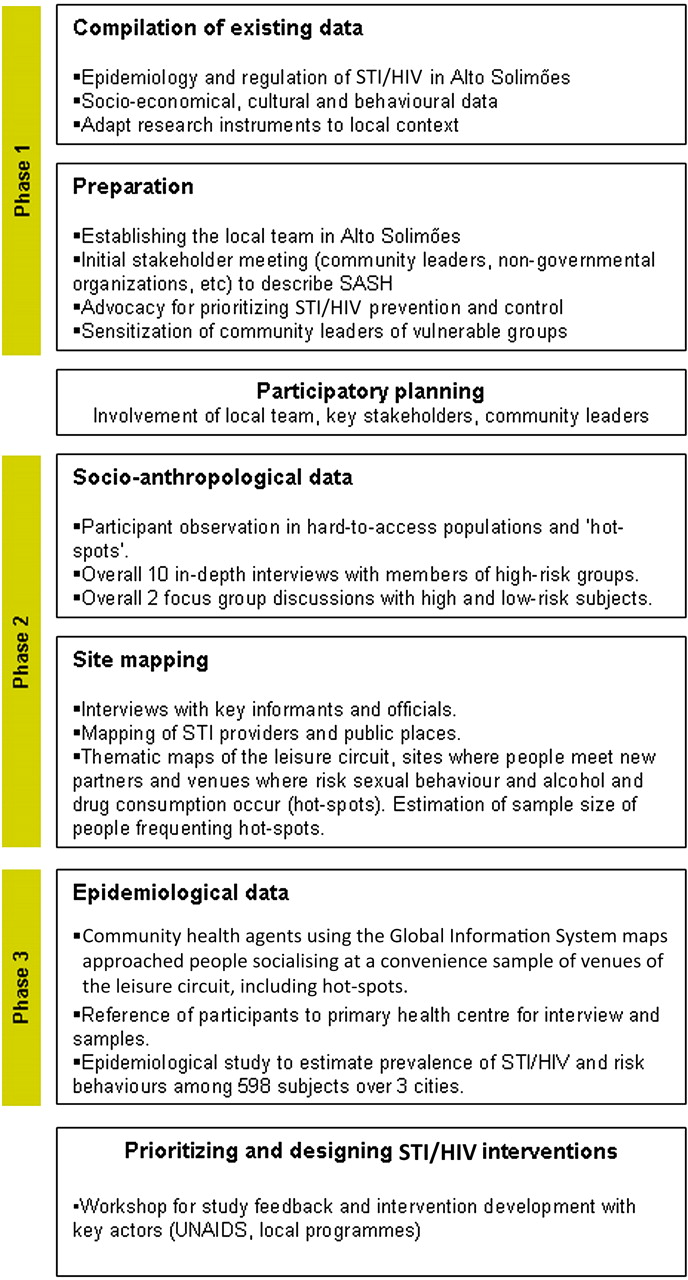
In the triple-border area, SASH was implemented in three phases as shown in figure 1. The SASH protocols were approved by the Ethical Review Committee of the Fundação Alfredo da Matta (approval number: 005/2007), Manaus.

{kind=link}
Phases of the situational analysis of sexual health (SASH) approach in Alto Solimões Region. STI, sexually transmitted infection.
Two anthropologists and a geographer conducted mapping to identify and locate the ‘leisure circuit’ that included all sites where people meet potential (new) sexual partners (overall 19 sites), places where to rent a room for having sex (overall 78 sites), places where risky sexual behaviour or alcohol and drug consumption occurred (overall 57 sites) and any combination of the above ‘hot spots’ (overall 44 sites).13 14 Markets, squares, bars, discos, hotels and motels were located based on direct observation of daily activities and interviews with key informants from the community assumed to be knowledgeable about the area and were visited for further information.15 Thematic maps using the global information systems were produced and together with the anthropological observations provided a sampling frame that guided the selection of study sites for the next phase of SASH.
Study population and study procedures
Community health agents, guided by the anthropologist and using the global information systems maps, moved from city to city and approached all individuals socialising at ‘hot spots’ and other identified venues of the ‘leisure circuit’ and informed them of the epidemiological study. Information was also provided through the local media, leaflets and posters. A convenience sample size was determined based on allocated study duration, while aiming to provide enough precision to calculate STI/HIV prevalence. The sample size was weighted according to each city's population size and stratified by sex (targets of 300, 200 and 100 individuals, respectively).
Interested individuals self-presented to a primary healthcare centre in each city where a doctor or nurse explained study procedures and obtained written consent. Participants were interviewed using a structured questionnaire on socio-demographic characteristics, knowledge of STI, risk behaviour, risk perception, alcohol and drug consumption, reason for HIV testing, experience of physical and sexual violence and presence of STI symptoms. Endocervical or urethral specimens were collected using brushes that were inserted into vials containing Universal Collection Medium (QIAGEN, Gaithersburg, Maryland, USA) and stored at 4°C. A 7 ml venous blood sample was drawn and stored on local freezers at −20°C. Samples were shipped monthly and processed at the Fundação Alfredo da Matta (FUAM) STI/HIV reference laboratory in Manaus.
Any genital tract infection identified was treated according to national guidelines. STI and HIV results were provided confidentially back to the participants within 30 days, and HIV-positive cases were referred to the appropriate hospitals.
Laboratory methods
Molecular tests were performed on cervical and urethral samples to detect Neisseria gonorrhoeae and Chlamydia trachomatis using Hybrid Capture® 2 CT-ID DNA Test Version 2.0 and Hybrid Capture® 2 GC-ID DNA Test Version 2.0 (QIAGEN); and high-risk human papillomavirus (hr-HPV) genotypes using the Hybrid Capture® 2 High-Risk HPV DNA Test that can detect qualitatively 13 hr-HPV genotypes (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59 and 68).
Sera were tested for HIV with Genscreen ULTRA HIV Ag-Ab EIA assay (BIO-RAD, Marnes-la-Coquette, France). Indirect immunofluorescence analysis (Bio-Manguinhos, FIOCRUZ, Rio de Janeiro, Brazil) confirmed HIV-positive results and Western Blot (Abbot Park, Illinois, USA) discordant results. Syphilis serology was performed using both the fluorescent treponemal antibody absorption test (WAMA Diagnostica, São Paulo, Brazil) and the Venereal Diseases Research Laboratory Test (Laborclin, Pinhais, Paraná, Brazil). The HerpeSelect® ELISA (Focus Technologies, Inc., Cypress, California, USA) was used to identify IgG antibodies specific to herpes simplex virus type-2 (HSV-2) using the manufacturer's cut-off of 1.1. The presence of antibodies against hepatitis B core antigen (Anti-HBc total) and of hepatitis B virus (HBV) surface antigen (HBsAg) was tested using a third-generation immunoassays (Hepatitis B DiaSorin®, Saluggia, Italy). The presence of IgG antibodies against hepatitis C virus (HCV) was tested using Hepatitis C Hepanostika® HCV Ultra (BioMerieux, Marcy L'Etoile, France).
Statistical analysis
Data were analysed using STATA V.10.0 (StataCorp). Comparisons between men and women were examined using Pearson χ2 test for categorical variables (and Fisher's exact test for small numbers) and the Student t test or the Wilcoxon rank-sum test for continuous variables. Risk factors for HSV-2 and hr-HPV (separately for men and women) were identified using multivariable analysis by which all factors with a p value <0.05 in the univariable analysis were included in a logistic regression model following a backward stepwise procedure to retain in the final model only factors with a likelihood ratio test p value ≤0.05.
Results
Social behaviour characteristics
Over 6 months, 598 individuals spontaneously presented to the clinics and participated in the study (300 in Tabatinga, 199 in Benjamin Constant and 99 in Atalaia do Norte). Among participants, 415 (71.1%) had heard about the study through leaflets or posters and 168 (28.8%) had heard from a friend from outside the ‘leisure-circuit’. Overall, 285 were men of median age 28 years (IQR, 23–37 years) and 313 were women of median age 29 years (IQR, 24–37 years). All but one participants were Brazilians, but 234 (40.0%) were not born in the Amazon state. Table 1 shows the population characteristics by sex. Overall, 291 participants (49.3%) reported a casual partner during the past 3 months (of those, 14.8% reported two casual partners or more), particularly men (p<0.001), but only 38.5% reported consistent condom use with any partner. Few women (3.5%) self-identified as sex workers, 6.3% of men and 2.3% of women reported having sex with same sex partners (p=0.01) and 12.5% of respondents knew of cases of child prostitution in their city. Men were more likely than women to admit drinking alcohol (65.3% vs 37.9%, p<0.001) and using recreational drugs (14.2% vs 6.9%, p=0.001). Interestingly, most men and women stated that drug use could increase the risk of HIV. Over a third of respondents (34.8%) correctly identified what ‘STI’ stands for, but few (17.3%) could actually report the name of an STI. The main reason for HIV testing (95.2%) was to know one's HIV status. Most respondents (69.5%) believed that HIV was a problem in their cities. Socio-behaviour characteristics by city are shown in the supplementary table S1, available online.
Characteristics of study population in Alto Solimões, Amazonas state, Brazil, by sex
Prevalence of STI and HIV
Women were significantly more likely than men to present STI symptoms (62.8% vs 9.8%, p<0.001) and abnormal findings at genital examination (82.1% vs 6.7%, p<0.001). Table 2 shows STI/HIV prevalence by sex. The predominant STI was HSV-2, with a prevalence of 62.1% (95% CI 58.0% to 66.0%), followed by HBV (anti-HBc 40.3%, 95% CI 36.3% to 44.4%). Overall, there was a relatively low prevalence of bacterial STIs, particularly N gonorrhoeae (0.7%, 95% CI 0.2% to 1.7%). Women were significantly more likely than men to be infected with C trachomatis (4.8% vs 1.4%, p=0.02), HSV-2 (72.1% vs 51.1%, p<0.001) and hr-HPV (24.0% vs 14.4%, p=0.003), while a significantly greater proportion of men were infected with HIV (1.4% vs 0.0%, p=0.04). STI/HIV prevalence by city is displayed in the supplementary table S2, available online.
Prevalence of STI/HIV in 598 men and women in Alto Rio Solimões, Amazonas state, Brazil, by sex
Risk factors associated with HSV-2 and hr-HPV
Table 3 presents risk factors for HSV-2. In the multivariable model, older age and being female remained associated with HSV-2 infection after adjustment.
Risk factors for HSV-2 serological infection in 280 men and 305 women in Alto Rio Solimões, Amazonas state, Brazil
With regard to risk factors for hr-HPV among women, those single were twice as likely to present a positive hr-HPV test (AOR 1.93, 95% CI 1.12 to 3.33; p=0.02). Among men, being of indigenous descent and having current STI symptoms were significantly associated with a positive hr-HPV test (AOR 2.43, 95% CI 0.94 to 6.29; p=0.07, and AOR 2.42, 95% CI 0.96 to 6.10; p=0.06, respectively). Compared to the reference group (<25 years), older age was associated with hr-HPV infection in women (for age group 25–34 years: AOR 0.46, 95% CI 0.24 to 0.88; p=0.02) and men (for age group ≥35 years: AOR 0.25, 95% CI 0.08 to 0.81; p=0.02).
Discussion
Among the sample of men and women recruited at ‘hot spots’, our findings suggest a relatively low prevalence of bacterial STIs and HIV, being usually higher in men. However, the prevalence of other viral STIs was high, including HSV-2, hr-HPV and HBV, which reflects the high-risk behaviour of these populations with high frequency of casual sex, low consistent condom use and high alcohol consumption. In Brazilian urban population, consistent condom use with any partner has been estimated at 28%.16 The prevalence of syphilis among study participants (3.1%) was higher than that found among nearly 45 000 indigenous individuals recently tested in the area (1.5%),17 although among female participants, the observed prevalence (2.6%) was similar to that of pregnant women in the same region (2.2%).18 The neighbouring department of Loreto in the Peruvian Amazonas boasts the second highest rate of HIV infection (0.46%) after the capital city, Lima,19 and high prevalence of HIV and syphilis at 2.1% and 3.2%, respectively, have been recorded in some American indigenous communities of Peru,20 highlighting the vulnerability of populations living in the Amazon basin. In the general adult population of Brazil, the HIV prevalence has remained relatively stable at 0.6% since 2000,21 whereas it is at 6.2% among female sex workers and at 13.6% among men who have sex with men.22
The complementary anthropological study (not reported in detail in this paper) obtained in-depth information on contextual elements such as the local sex and behaviours that were invaluable to understand the importance of mobility in the context of STI/HIV acquisition in the triple-border area. Actions that individuals take regarding STI/HIV prevention (such as condom use) are intimately linked to the notion of ‘trust’, whereby the perception of one's risk-taking is more related to the dichotomous construction of people viewed as ‘locals’ versus ‘outsiders’, rather than using an implicit epidemiological construct such as belonging to ‘low-risk’ or ‘high-risk’ groups. In these isolated communities, there is a general lack of ‘trust’ of outsiders, who belong to the ‘risky’ groups, but unlicensed behaviour is acceptable with ‘locals’. Interestingly, the high proportion of respondents who themselves originated from other regions of Brazil points to the high levels of mobility in our sample and testifies of their regular patronising of ‘hot spots’. The highly permissive alcohol consumption culture would be expected to enhance their STI/HIV risk.23
While the main risky behaviours that contribute to the spread of HIV are already in place in these populations, our findings indicate that there is still time and opportunity to avert a major HIV epidemic in the Alto Solimões. A rapid spread of HIV could be magnified by the high-risk nature of life in the triple-border area, an important trade and transit centre characterised by drug trade, illegal employment, the presence of vulnerable populations and internal and international mobility, a well-established risk factor of HIV transmission.24 The isolation and distance from services, the lack of resources and inadequate management by local HIV/AIDS control programmes have hampered the implementation of STI/HIV prevention efforts.8
This action–research process emphasises consensus building to design context-relevant, highly acceptable and locally owned interventions through a high degree of consultation and involvement of local stakeholders, including representatives of vulnerable groups who can act as research actors. The methodology does not take a purely risk-group-based approach nor does it focus on traditionally defined risk groups, as in the WHO's rapid assessment and response method of assessing injection drug use.25 26 Instead, like in the PLACE method,10 27 the focus shifts to identifying transmission networks through the places where (new) sexual partners are sought. Therefore, by not asking about particular risk groups, the approach is less stigmatising and more likely to uncover transmission networks. While many of the venues identified by the mapping study were traditional ‘hot spots’ such as bars, night clubs and informal drinking places, other public spaces such as schools and markets were also identified as places where people meet their sexual partners. In particular, the mapping exercise was highly successful and valuable to approach the relevant populations, allowing them to also be included in the behavioural and STI/HIV prevalence surveys. The epidemiological component, which is not included in the PLACE method, may delay the stage of intervention design, but it provides valuable information for the development of relevant interventions as well as providing useful baseline quantitative data for future monitoring.
The versatile nature of the SASH approach allowed adapting it to the local context focusing on high-risk group rather than add a general population survey component and thus covering only parts of the original package. Antenatal data obtained from the same cities had shown an HIV and syphilis prevalence of 0.2% and 2.2%, respectively.18 28 In both India and China, high-risk populations were also targeted in the epidemiological studies with the sampling strategy stratified subjects by type of sex work, based on prior typology obtained during the anthropological data collection. In Alto Solimões, the sampling strategy was also guided by the anthropological study, which recorded a more diffuse and homogenous risk behaviour centred around hot spots rather than in particular groups.
The SASH method has several limitations. It favours rapidity and triangulation of data at the expense of accuracy. By design, it is not expecting to provide representative population-based data. Indeed, there is an inherent self-selection bias that is likely to account for some of the higher risky behaviours and STI prevalence found among participants or, on the contrary, represents a low-end estimate of prevalence if truly infected subjects did not present to the clinics. Stigma surrounding vulnerable groups, fear of discrimination and fear of a positive HIV result may have acted as potential barriers to accessing the clinics.29 The collection of data on-site using non-invasive samples might had increased participation, but it adds complexity to the study, and we lack evidence on the performance of syphilis and HSV-2 tests on dried blood spots samples.
The SASH method proved an important catalyst for action. As a result, the Amazonaids initiative that was set in the state of Amazon since 2008 has intensified its efforts in the triple-border area30 by (1) improving access to diagnostic and treatment through the implementation of rapid HIV and syphilis testing, (2) increasing prevention activities through training of school teachers on HIV/STI prevention and distribution of prevention material and (3) strengthening the role of civil society in the decision-making process for health.
Key messages
The SASH conducted in the triple-border area of the Amazon state has highlighted behaviours and networks that may contribute to the spread of STI/HIV.
An anthropological study and mapping activities identified sites and networks likely to have higher incidence of STI/HIV but not targeting specifically a group of individuals.
The SASH is a relatively simple and semi-rapid methodology that combines anthropological, clinical and epidemiological studies to elicit complementary and mutually validating findings.
The SASH is an action–research process that emphasises the involvement of local actors to design setting-specific STI/HIV preventive initiatives.
Acknowledgments
We thank the staff at Fundação Alfredo da Matta and Fundação Oswaldo Cruz/Instituto Leônidas e Maria Deane, AM, Manaus (Brazil) for their technical assistance, as well as the participants for their time. We wish to thank Secretaria Municipal de Saúde of the municipalities of Tabatinga, Atalaia do Norte and Benjamin Constant, in particular the Programa de Saúde da Família and Coordenação de DST/AIDS, Conselho tutelar de Tabatinga, Associação dos soropositivos para VIH de Tabatinga, Programa Sentinela de Tabatinga of Brazilian Government, Universidade do Estado de Amazonas of Tabatinga, Universidade Federal do Amazonas of Benjamin Constant, Fundação Nacional do Índio (FUNAI) and Fundação Nacional de Saúde (FUNASA), which today is the Secretaria Especial de Saúde Indígena (SESAI) of the Ministry of Health.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
Funding The study was supported by a grant from the Fundação de Amparo à Pesquisa do Estado do Amazonas/FAPEAM.
Competing interests None.
Patient consent Obtained.
Ethics approval Ethical review committee of the Fundação Alfredo da Matta (FUAM), Manaus, Brazil.
Provenance and peer review Not commissioned; externally peer reviewed.