Article Text

Abstract
Objective To assess adherence to post-exposure prophylaxis (PEP) for the prevention of HIV infection in victims of sexual assault.
Methods The authors carried out a systematic review, random effects meta-analysis and meta-regression of studies reporting adherence to PEP among victims of sexual violence. Seven electronic databases were searched. Our primary outcome was adherence; secondary outcomes included defaulting, refusal and side effects.
Results 2159 titles were screened, and 24 studies matching the inclusion criteria were taken through to analysis. The overall proportion of patients adhering to PEP (23 cohort studies, 2166 patients) was 40.3% (95% CI 32.5% to 48.1%), and the overall proportion of patients defaulting from care (18 cohorts, 1972 patients) was 41.2% (95% CI 31.1% to 51.4%). Adherence appeared to be higher in developing countries compared with developed countries.
Conclusions Adherence to PEP is poor in all settings. Interventions are needed to support adherence.
- Adherence
- antiretroviral therapy
- primary HIV infection
- sexual health
- systematic reviews
- teaching
- social science
Statistics from Altmetric.com
- Adherence
- antiretroviral therapy
- primary HIV infection
- sexual health
- systematic reviews
- teaching
- social science
Introduction
Sexual assault is a worldwide public health concern that can place victims at risk of unplanned pregnancies, psychological morbidity and sexually transmitted infections including HIV. The risk of HIV transmission differs according to the mode of penetration (0.1%–0.2% for receptive vaginal exposure and 0.8%–3% for receptive penile–anal exposure)1 ,2 and may be increased by factors associated with sexual assault such as genital trauma, exposure to other sexually transmitted infections and attack by multiple assailants.3 Incidence of sexual assault varies, but high rates of sexual assault have been reported in countries with high HIV prevalence. In Kenya, for example, 24% of women have been raped at least once in their lifetime and about 4% of HIV infection in adolescents is attributable to rape.4
HIV post-exposure prophylaxis (PEP) is a short course of antiretroviral therapy offered to individuals at risk of acquiring HIV. Current WHO guidelines recommend a 28-day course of treatment to be administered within 72 h of exposure using a combination of two or three antiretroviral drugs.5 Adherence to PEP is a challenge, with studies from a range of settings indicating that PEP acceptance, completion and HIV testing rates are generally lower following sexual assault compared with consensual sexual exposures.3 ,6–12 Factors associated with poor adherence include stigma associated with HIV, psychological trauma after rape,13 side effects associated with the PEP drugs, transport costs to the health clinic, poor patient knowledge of the reasons for administering PEP and lack of trauma counselling.3 ,7 ,8 ,14 ,15 Provision of PEP is a particular challenge in resource-limited settings such as sub-Saharan Africa, where the prevalence of both HIV and sexual assault is high and where issues such as limited training of service providers and inadequate follow-up systems further complicate PEP administration.16
We conducted a systematic literature review and meta-analysis to assess rates and determinants of PEP adherence in the context of sexual assault.
Methods
Search strategy
We searched the following databases from inception to 1 June 2011: MEDLINE, EMBASE, Health Management Information Consortium, PsycInfo, The Cochrane Library, POPLINE and Global Health Library using a compound search strategy combining terms for ‘sexual assault’, ‘post-exposure prophylaxis’, and ‘adherence’ was performed. Search terms and MeSH terms are detailed in the study protocol (http://tinyurl.com/3ves67q). Bibliographies of all retrieved articles were also screened. The initial search was carried out by one researcher and subsequently verified in duplicate by two supervising researchers. No language restriction was applied.
Inclusion and exclusion criteria
We included observational and experimental studies that reported data on adherence to PEP among victims of sexual assault. When studies reported data that were previously reported elsewhere, the most complete citation was included.
Data extraction
Information was extracted on study characteristics, indicators of study quality and outcome data. In order to distinguish between patients who were known to be non-adherent to PEP and those who were lost to follow-up but may still be adherent to a number of distinctions were made. Individuals that completed a 28-day course of PEP treatment were defined as ‘Adherent’, those that refused to start PEP treatment were defined as ‘Refusals’, while those that did not return to collect their medication or did not return for follow-up appointments were defined as ‘Defaulters overall’. This latter category included ‘Defaulting on incomplete treatment’ (those who received an initial course of PEP but did not return to collect the remainder of the course and therefore cannot be adherent) and ‘Defaulting with full treatment’ (those that collected a full 28-day course of PEP but did not return for a follow-up visit and who may or may not be adherent).
Quality and validity
There is no agreed tool for the assessment of methodological quality for observational studies.17 We assessed the following factors as determinants of study quality: proportion of refusals, method of adherence measure, reporting of side effects, specification of inclusion and exclusion criteria, study design, sample size calculation and statistical analysis. We did not attempt to provide a quantitative ranking of study quality, as scoring systems are subject to bias, even for controlled trials.18 No studies were excluded on the basis of quality.
Data analysis
Point estimates were calculated and 95% CIs for the proportion of patients adhering to PEP at various stages in the care pathway from the initial offer of PEP treatment to the final follow-up appointment. Outcomes for cohort studies and randomised trials are reported separately. For cohort studies, the variance of the raw proportions was stabilised using a Freeman–Tukey type arcsine square-root transformation. Anticipating high heterogeneity considering the variation in study populations and healthcare settings, we pooled data using a DerSimonian–Laird random effects model.19 The τ2 statistic was calculated to assess between-study heterogeneity. Potential sources of heterogeneity were investigated through subgroup analysis and meta-regression assessing the following clinical and programme level covariates defined a priori: age (adults vs children/adolescents), drug regimen, country (developed vs developing country) and setting (sexual assault services vs general hospital setting).19 All p values were two-sided, and a p value of <0.05 was considered statistically significant. Analyses were conducted using Stata V.11 (StataCorp LP).
Results
Study selection
The initial search yielded 2159 articles (figure 1), of which 56 were taken through for full review. Reference lists of relevant articles were also searched, yielding one additional study (figure 1). Twenty-four studies matching our inclusion criteria were taken through for analysis. These included two conference abstracts.20 ,21 and one non-English publication (French).22 Unpublished reports and non-peer-reviewed reports were not included. One study was excluded after contacting the authors as this was found to be a sub-analysis of a study already included.23

Flow diagram summarising study selection.
Study characteristics
Participants in 13 studies were adults3 ,7 ,20–22 24–31 out of which two studies included only women3 ,29 three studies included both children and adults as participants.15 ,32 ,33 Two studies were in women of all ages34 ,35 and six studies included children and adolescents only as participants4 ,8 ,36–39 (table 1). Study settings included sexual assault services4 ,7 ,15 ,20–22 ,25 ,28 ,29 ,34 ,35 and hospital emergency departments.3 ,8 ,37–39 In three studies, data were obtained from PEP databases and sexual assault was studied as a subgroup of ‘sexual exposure’ or ‘non-occupational exposure’.26 ,27 ,30 Eight studies were conducted in developing countries.4 ,24 ,25 ,32–36 Seventeen studies were retrospective designs,3 ,4 ,7 ,8 ,20–22 25–31 ,35 ,38 ,39 six were prospective designs15 ,24 ,32 ,33 ,36 ,37 and one was a randomised controlled trial.34 Only three studies assessed interventions to improve adherence such as telephonic psychosocial support34 and different models of care.24 ,33
Characteristics of included studies
Quality of studies
Table 2 shows the methodological characteristics of the included cohorts. Most studies did not report data on the number of patients that refused PEP. Seven studies reported on refusals3 ,7 ,8 ,15 ,22 ,28 ,32 and of these, two studies had refusal rates of greater than 20%.7 ,15 The reasons for discontinuing PEP were poorly documented overall, and side effects were not reported in seven studies.3 ,7 ,25 ,27 ,33 ,35 ,36 Inclusion or exclusion criteria were not specified in five studies.7 ,26 ,33 ,38 ,39 Pill counting was used as a method for measuring adherence in two studies34 ,37; however, the majority of studies did not specify how adherence was measured.
Methodological quality assessment
PEP regimens
Twenty studies provided data on drug regimens. Eight studies used two-drug regimens,4 ,7 ,24 ,25 ,34 ,36 ,37 ,39 seven studies used three-drug regimens,15 ,21 ,22 ,28–30 ,38 while five studies prescribed both two- and three-drug regimens.3 ,9 ,27 ,31 ,32 One study provided different regimens according to the severity of the sexual assault.32 All the drug regimens included zidovudine. Two-drug regimens consisted of zidovudine and lamivudine,4 ,24 ,25 ,34 ,36 ,37 ,39 except for one in which zalcitabine was given with zidovudine.7 The three-drug regimens consisted of single drugs including zidovudine, lamivudine and nelfinavir, indinavir, lopinavir/ritonavir, nevirapine or efiravenz; two studies offered Truvada (emtricitabine/tenofovir) with Kaletra (lopinavir/ritonavir).21 ,29 PEP dispensing practices varied between studies. Eight studies provided patients with starter packs.3 ,7 ,8 ,20 ,22 ,24 ,26 ,34 The duration of the starter packs ranged from 2 to 7 days. Two studies provided all the medication at once28 ,29 and four studies dispensed 7-day packs.22 ,25 ,27 ,36 One study found that patients given a full course of drugs on the first visit were more likely to be fully adherent compared with those given a starter pack with follow-up appointments (at which the remaining PEP was provided) (71% vs 29%).33
Measurement of adherence
Adherence was assessed through pill count (or volume of syrup remaining),34 ,37 self-report7 ,22 ,24 ,29 ,33 ,36 ,39 or by counting pharmacy visits.25 ,27 However, most studies did not specify how adherence was measured. One study assessed the completion of the 28-day PEP course using a calendar and visual recognition tool.33 Two studies measured adherence by counting the number of prescriptions for PEP that participants obtained from the pharmacy, making the assumption that filling in four prescriptions equated to consumption of a full course of PEP.25 ,27 One of these studies recorded whether patients kept appointments for their weekly prescriptions over the duration of 4 weeks.25 The other study cross-referenced dispensary records with the date of exposure and date of PEP initiation.27
Adherence outcomes
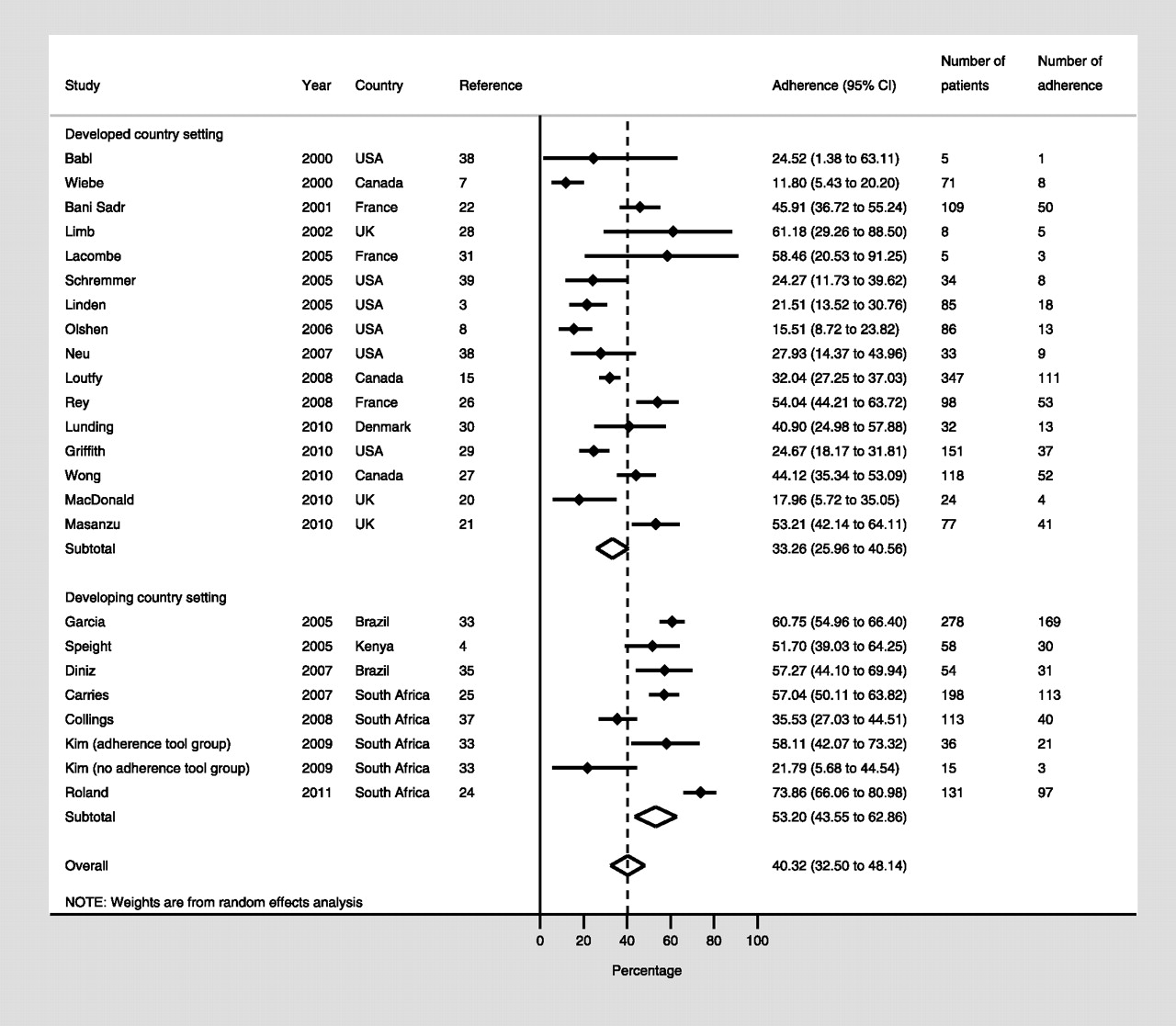
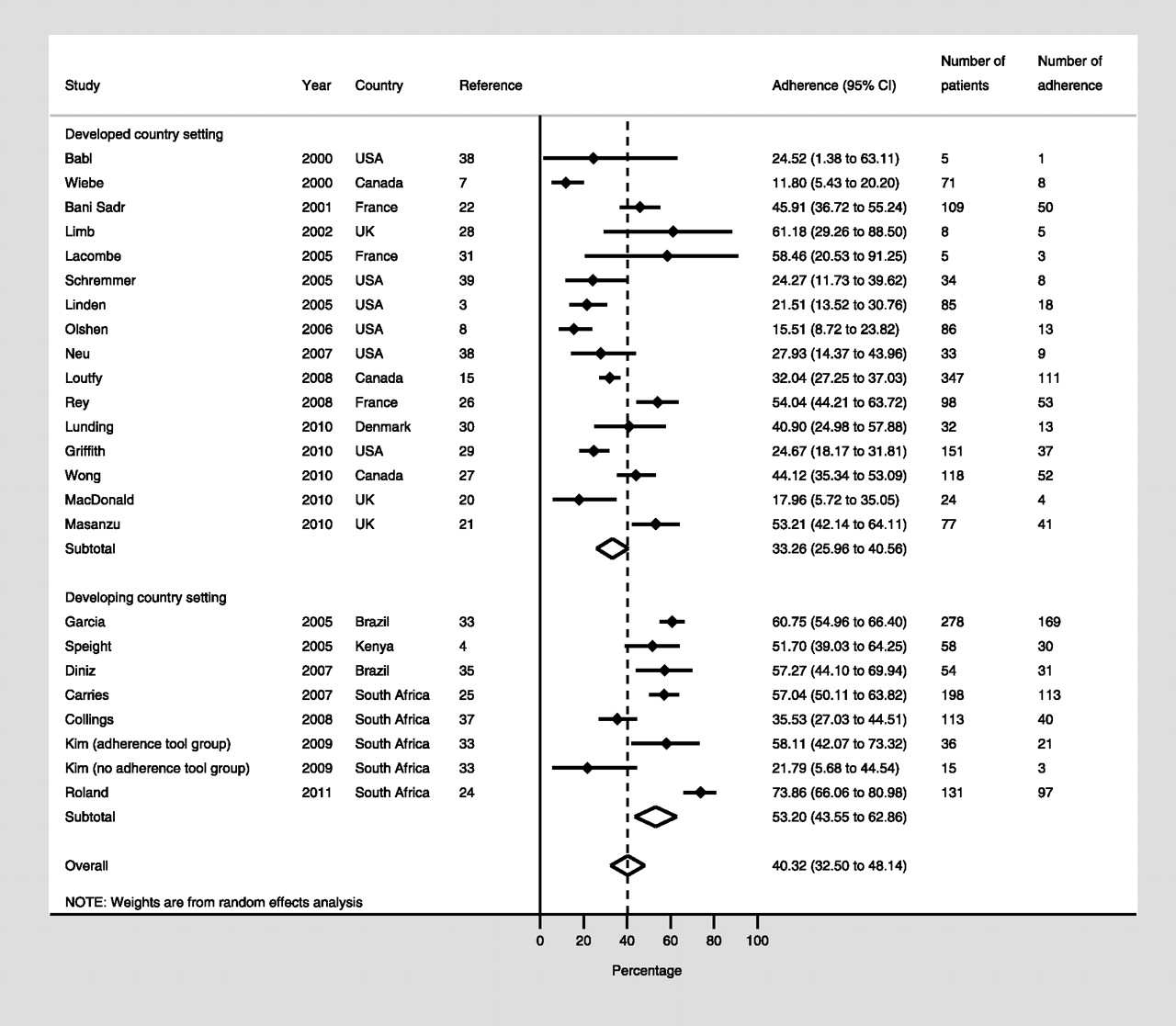
Twenty-three cohorts and one randomised trial reported on the overall proportion of patients adhering to PEP. The proportion of patients adhering to PEP in the cohort studies (2166 patients) varied considerably across studies, ranging from 11.8% (95% CI 5.4% to 20.2%) to 73.9% (95% CI 66.1% to 81.0%), with an overall pooled proportion of 40.3% (95% CI 32.5% to 48.1%) (figure 2). Heterogeneity was high (τ2 331.9). Adherence appeared to be higher in developing countries (53.2%, 95% CI 43.5% to 62.9%) compared with developed countries (33.3%, 95% CI 26.0% to 40.6%) (p=0.01), a difference confirmed through meta-regression (β-coefficient 20.3, 95% CI 6.2 to 34.3, p=0.007). All other covariates were non-significant.
{kind=link}
{kind=link}
Pooled proportion of patients fully adherent to post-exposure prophylaxis.
For the randomised trial, adherence was 38.2% in the intervention arm and 31.9% in the control arm (p=0.13).
Eighteen cohorts and one randomised trial reported on the overall proportion of patients defaulting from PEP. The proportion of patients defaulting overall from PEP in the cohort studies (1972 patients) ranged from 2.9% (95% CI 2.4% to 22.7%) to 75.7% (95% CI 65.2% to 84.8%), with an overall pooled proportion of 41.2% (95% CI 31.1% to 51.4%). Heterogeneity was high (τ2 445.0). In meta-regression, there was no difference in the overall proportion of patients defaulting from PEP by age (p=0.4) or setting (p=0.3).
For the randomised trial, the proportion defaulting was 27.2% in the intervention arm and 35.5% in the control arm.
We further assessed rates of defaulting at various stages in the care pathway from the initial offer of PEP treatment to the final follow-up appointment at the end of PEP treatment. Six cohort studies reported on the proportion of eligible patients refusing the offer of PEP, which ranged from 0.09% (95% CI 0.08% to 0.78%) to 72.39% (95% CI 66.80% to 77.66%) with a pooled proportion of 28.69% of patients refusing PEP (95% CI 0.20% to 57.69%). Nine cohort studies and one randomised trial reported on the proportion of patients who defaulted PEP prior to receiving a full course of treatment (‘Defaulting on incomplete treatment’), for which patients could be considered non-adherent. For the cohort studies, the proportion of patients defaulting ranged from 2.9% (95% CI 2.4% to 22.7%) to 64.5% (95% CI 55.5% to 73.0%) with an overall pooled proportion of 33.4% (95% CI 20.8% to 45.9%). For the randomised trial, 21.3% of patients in the intervention arm and 28.3% of patients in the control arm defaulted prior to receiving the full course of treatment. Finally, six cohort studies reported on the proportion of patients who defaulted after having received a full course of PEP (‘Defaulting with full treatment’) and thus patients may or may not be adherent. The proportion of patients defaulting ranged from 2.9% (95% CI 2.4% to 22.7%) to 25.0% (95% CI 12.1% to 40.7%) with a lower overall pooled proportion of 9.9% (95% CI 2.8% to 17.0%).
Side effects
Three studies found that adherence was associated with drug side effects.15 ,32 ,37 Of these, one reported that those taking a three-drug regimen in a high-risk group had worse side effects than those taking a two-drug regimen in a medium-risk group.32 The second study found that the only predictive variable for non-adherence to follow-up visits and non-adherence to PEP was the presence of side effects,37 and the third study found that participants who experienced vomiting were less likely to complete PEP than those who did not (OR 0.27, 95% CI 0.12 to 0.6, p=0.0007).15 Two studies reported that side effects did not appear to influence PEP completion.20 ,34 The most frequently documented side effects across all studies included nausea, vomiting, diarrhoea and fatigue.
Interventions to improve adherence
Three studies assessed interventions to improve adherence.24 ,33 ,34 A randomised trial in which two groups were given written information and an adherence diary but one group additionally received telephone counsellor support found no benefit of telephone counselling but some evidence that the telephone counselling led to more participants reading the information pamphlet (p=0.06) and using the adherence diary (p=0.001).34 Another study evaluated a nurse-driven model of post-rape care integrated into hospital services and found an increase in self-reported adherence (from 20% to 58%) and patient treatment literacy compared with the previous service delivery model.33 Finally, a study piloted a proactive, flexible nurse-driven follow-up system for sexual assault survivors.24 In this non-comparative study, nurses offered follow-up visits over the course of 6 months at four sites: a rape treatment centre, a research office, a primary care health centre or at the participant's home. The completion rate was 74%.
Discussion
Our review confirms an overall low rate of adherence to PEP among victims of sexual assault with considerable variation in rates of adherence and defaulting across a broad range of settings. Low adherence is a concern as it is associated with a risk of reduced efficacy and increased resistance to antiretroviral therapy.
We found adherence to be lower in developed country settings compared with developing country settings. This finding is consistent with rates of adherence to antiretroviral therapy more generally40 and may be due to a higher awareness of the risks of HIV transmission in settings where HIV prevalence is higher. HIV prevalence in the countries in which the studies included in this review were done ranged from 0.20% to 0.60% in developed countries and from 0.45% to 17.8% in developing countries41 (table 1).
Defaulting was high across all studies and varied across the PEP care pathway but few gave reasons for defaulting. While uptake of PEP was reasonable, around a third of patients defaulted before being given the full course of treatment. However, only 10% were likely to default after receiving the full course of treatment.
Our meta-analysis is subject to substantial heterogeneity that calls for caution in the interpretation of the pooled estimates. For example, our pooled estimate of 40.3% for adherence overall is derived from a set of studies in which adherence ranged from 12% to 74%. Because assessment of heterogeneity in pooled proportions may be misleading,19 ,42 we report the τ2 statistic as this is less affected by the number of studies than the more commonly used I2 statistic.43 We used a random effects model, which is more appropriate for meta-analyses in which heterogeneity is anticipated.19 We also explored potential sources of heterogeneity in meta-regression, which found that studies conducted in developing country settings resulted in higher rates of adherence. However, the inconsistency in reporting of clinical and programme factors that could potentially explain differences in adherence to PEP limited further exploration. Unmeasured factors such as the social context of blame and stigma associated with sexual violence are also likely to play a role.44 Despite these concerns, we consider that a meta-analysis is justified provided these limitations are taken into consideration.45
There are several other limitations to note. First, the reporting of adherence outcomes along the care pathway was not consistently reported across studies, leading to small sample sizes and greater imprecision for certain outcomes. Second, our assessment of the methodological quality of included studies indicated a number of potential sources of bias, in particular the lack of objective measures of adherence (which may result in either under- or over-reporting of adherence) and the retrospective design of several studies (which may lead to reporting bias). Finally, the potential for publication bias exists for this study as for all systematic reviews. Formal measures to assess publication bias are not appropriate for data derived from observational studies,46 but the poor outcomes reported by studies suggest no clear bias towards the reporting of positive results.
Our review serves to highlight the considerable variation in the way in which PEP is offered in terms of number and class of drugs, frequency of dispensing and provision of patient support. While we were not able to find any association between these variables and patient outcomes, the extent of variation suggests a need for future research to help standardise the package of care offered to patients. Studies also varied in the definition, measurement and reporting of adherence outcomes, pointing to a need to better standardise reporting in PEP programmes.
Finally, this review points to several areas for future research. An important limitation to the available literature is the absence of reporting of reasons for poor adherence to PEP and few evaluations of interventions to support adherence. Despite a substantial number of studies reporting poor adherence to PEP over the last decade, we were only able to find three studies assessing interventions to improve adherence. Future research should be directed to assess reasons for poor adherence and therefore potential interventions that could address these issues and improve adherence to PEP.
Key messages
Adherence to post-exposure prophylaxis is poor in all settings.
Adherence appears to be better in developing countries compared with developed countries; this may be due to a higher awareness of the risks of HIV transmission.
Future research should be directed at defining interventions to support adherence.
References
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.