Article Text

Abstract
Objectives To investigate the drivers behind the epidemic expansion of lymphogranuloma venereum (LGV) cases in late 2009 to help inform infection control.
Methods An epidemic curve of all LGV diagnoses between 2003 and mid-2012 was plotted and divided into the initial detection period, and endemic, growth and hyperendemic phases. Detailed clinical and behavioural data were collected and logistic regression was used to compare the characteristics of diagnoses made during the growth and endemic phases.
Results Between April 2003 and June 2012, 2138 cases of LGV were diagnosed. Enhanced surveillance data were available for 1370 of whom 1353 were men who have sex with men (MSM). 98% of MSM presented with proctitis, 82% were HIV positive, 20% were hepatitis C virus (HCV) antibody positive, and 67% lived in London. Growth phase cases (n=488) were more likely to report meeting sexual contacts at sex parties (11% vs 6%, p=0.014), unprotected receptive or insertive oral intercourse (93% vs 86%, p=0.001; 92% vs 85%, p=0.001) and sharing sex toys (8% vs 4%; p=0.011), and to be diagnosed HIV positive (86% vs 80%; p=0.014), than endemic phase cases (n=423). Unprotected receptive anal intercourse was equally likely to be reported in both phases (71% vs 73%). After adjustment, cases in the growth phase were more likely to meet new contacts at sex parties (p=0.031) and be HIV positive (p=0.045).
Conclusions Rapid epidemic growth coincided with an intensification of unprotected sexual activity among a core population of HIV-positive MSM. Efforts to develop innovative interventions for this hard-to-reach population are needed.
- Lymphogranuloma Venereum
- Epidemiology (General)
- Gay Men
- Sexual Behaviour
Statistics from Altmetric.com
Introduction
Lymphogranuloma venereum (LGV) is a sexually transmitted infection caused by the L serovars of Chlamydia trachomatis. Although historically considered a heterosexually acquired infection of the tropics, reports of LGV infection among men who have sex with men (MSM) have been documented in the USA since the 1970s.1 ,2 Since 2003, LGV infection in MSM has re-emerged with outbreaks in Western Europe, including the UK, the USA, Canada and Australia.3–8 The typical diagnostic profile has been of white, HIV-positive MSM who report high levels of unprotected anal intercourse and STI coinfection, and who are likely to attend sex parties and to report fisting and the use of sex toys.3 ,7 ,9 ,10
The UK response to the outbreak was to set up a diagnostic reference service and enhanced surveillance of LGV in October 2004, overseen by a LGV Incident Group.5 Since then, over 2000 LGV cases have been diagnosed in the UK, which now has the largest documented epidemic worldwide. Most cases have been diagnosed in London, Brighton and Manchester, which have large populations of MSM and established gay scenes.11 Infection control has concentrated on targeting health advice to raise awareness and promote condom use among at-risk MSM, as well as testing and treating symptomatic patients.11 As LGV is focussed in such a well-characterised high-risk population, and most infections are thought to be symptomatic, such interventions might be expected to limit onward transmission.12 However, control has been elusive, and of particular concern was the rapid growth in cases from the beginning of 2009.
The phase-specific epidemiologic model which was proposed by Wasserheit and Aral (1996) and subsequently developed and applied, provides a framework for data analysis and interpretation.13–16 Essentially, this model describes four phases: introduction/invasion, growth, hyperendemic and decline/control.13 Here we explore characteristics of LGV cases around the growth phase to investigate behavioural drivers in the epidemic and inform control strategies.
Methods
Diagnosis and enhanced surveillance of LGV
Details of the LGV reference service have been published elsewhere.5 Briefly, genital and rectal specimens from all symptomatic (proctitis or inguinal lymphadenopathy) MSM attending genitourinary medicine (GUM) clinics who were diagnosed with C trachomatis, or who were contacts of LGV-positive cases, were referred to the Sexually Transmitted Bacteria Reference Unit (STBRU) for LGV typing. This testing policy for LGV has not changed since the reference service was established. From August 2006, Scottish specimens were referred to the Scottish Bacterial Sexually Transmitted Infections Reference Laboratory. All patients were managed and tested for other STIs according to routine clinical practice.
For each confirmed LGV case the attending GUM clinician was asked to complete an enhanced surveillance form which collected detailed clinical, demographic and behavioural information (available at http://www.hpa.org.uk/webc/HPAwebFile/HPAweb_C/1194947315758). To improve ascertainment and accuracy of HIV diagnosis information, LGV case reports were matched to new HIV diagnosis reports using the patient ID number. Enhanced LGV surveillance was discontinued in December 2010 and replaced with monitoring through the Genitourinary Medicine Clinic Activity Dataset (GUMCAD).17 Public Health England has approval from the National Information Governance Board (since superseded by the Health Research Authority Confidentiality Advisory Group; application no. 03(c)/2001) to collect anonymised patient-level data for the purposes of public health monitoring and infection control.
Defining epidemic phases
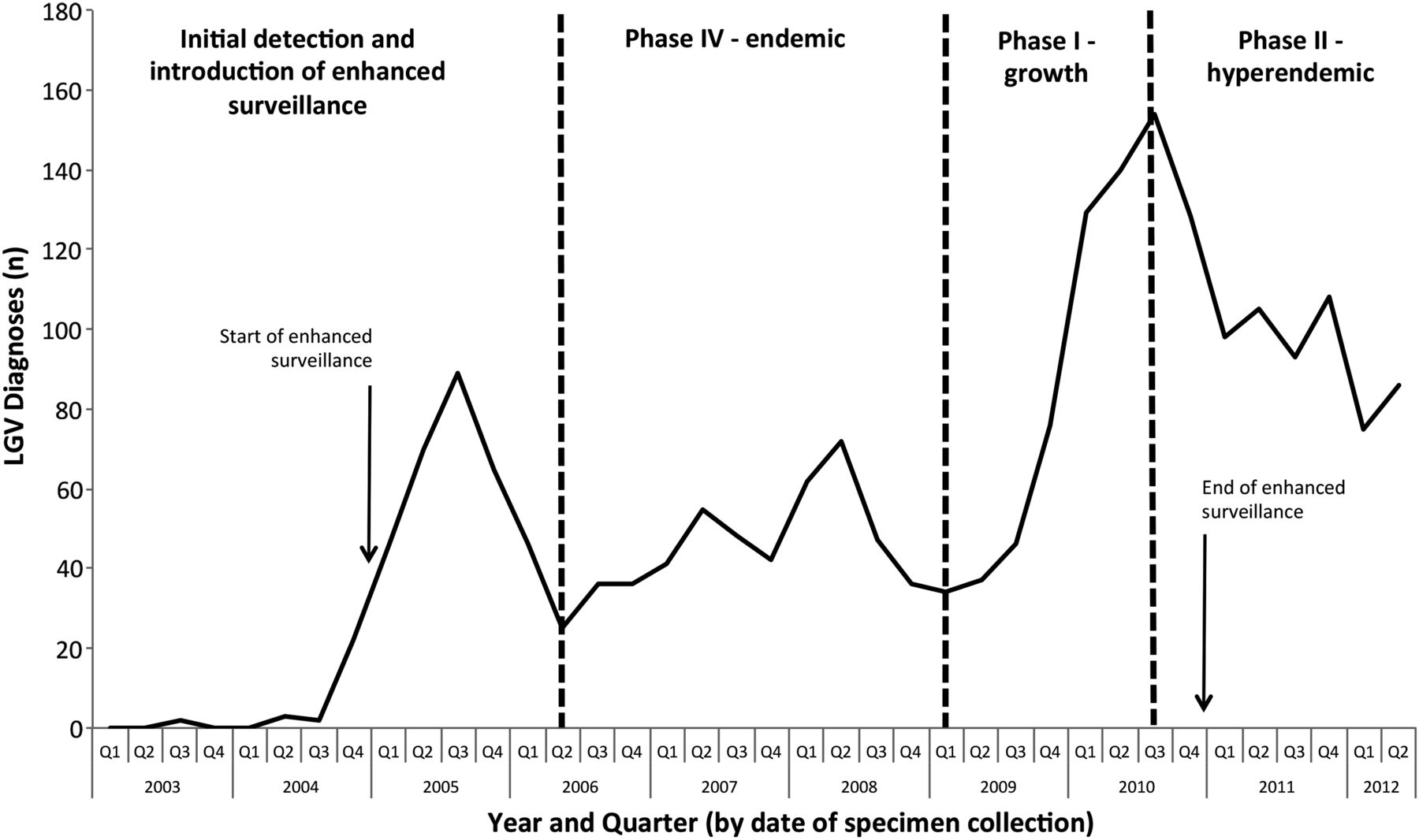
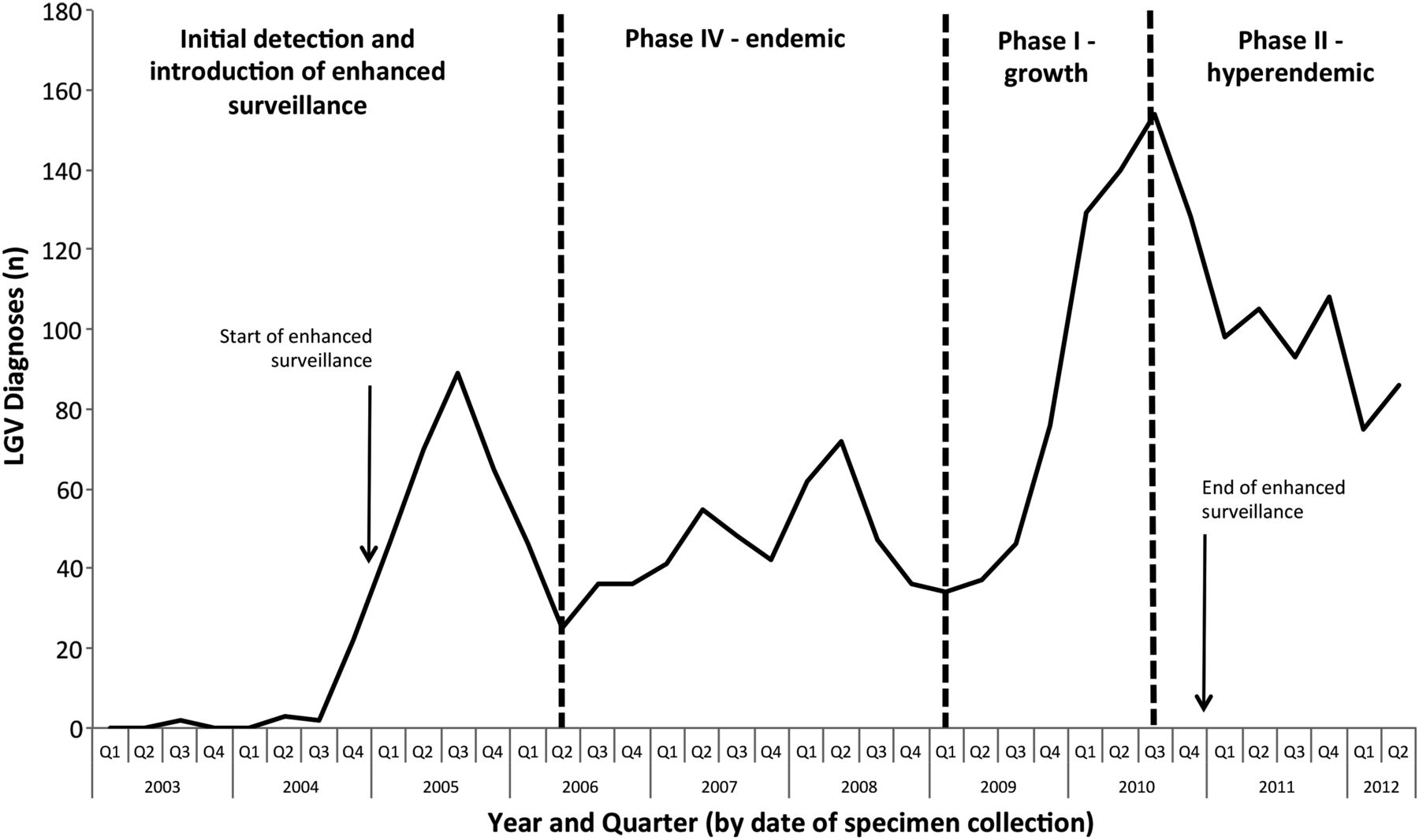
An epidemic curve of all LGV diagnoses up to the end of quarter 2 in 2012 was plotted (figure 1). The plot was divided into four periods:
-
Introduction/invasion: 2003/quarter (Q) 2 to 2006/Q2. This period encompasses the initial detection of an increase in LGV cases, the introduction and widespread use of diagnostic testing and an increased awareness to the infection among healthcare professionals and the public. As a result, there was a peak in diagnoses in 2005/Q3 which consisted of a mixture of incident infections together with long-standing infections. Some infected patients who were diagnosed with LGV during this period reported experiencing symptoms over several months and had been misdiagnosed with inflammatory bowel disease before referral to GUM. This mixture of incident and prevalent cases restricts interpretation of this period within the phase-specific model and, consequently, we did not attribute a phase prior to 2006/Q3.
-
Endemic (Phase IV): 2006/Q3 to 2008/Q4. In mid-2006, the curve stabilised at a lower, endemic level averaging at 46 cases per quarter.
-
Growth (Phase I): 2009/Q1 to 2010/Q3 From the beginning of 2009, diagnoses grew substantially to reach over 154 cases per quarter in 2010/Q3. Transforming the data for this time period to log values and calculating the R2 value for linear trend (R2=0.942) indicated that the data recorded over this time period followed a pattern of exponential growth.
-
Hyperendemic (Phase II): 2010/Q4 to 2012/Q2. Diagnoses stabilised after late 2010 at a new hyperendemic level averaging 99 cases per quarter.
{kind=link}
New LGV diagnoses reports, UK: April 2003 to June 2012.
Data analysis
To better understand the behavioural factors contributing to the exponential growth, cases diagnosed during the endemic and growth phases were compared. Univariable and multivariable logistic regression modelling was used to investigate variations in patient characteristics between the endemic and growth phases (binary outcome: 0=endemic phase; 1=growth phase). For the univariable analysis, information concerning clinical presentation, demographic characteristics, infection status and sexual behaviour were contrasted between the endemic and growth phases. Variables for which p<0.1 were included in the multivariable model. The only exception was proctitis which was excluded, as the proportion of men presenting with proctitis was extremely high in both periods (97% to >99%). Most of the variables included in the multivariable analysis were concerned with sexual behaviour. Cases reporting protected receptive oral intercourse (ROI) and protected insertive oral intercourse (IOI) were grouped with cases not reporting ROI or IOI in the multivariable model as numbers were small. Only cases with complete data were included. All main effects and two-way interactions were tested using the FITINT command in STATA V.12.0 (StataCorp, College Station, Texas, USA).18
Results
Descriptive analysis
In the UK, between 15 April 2003 and 30 June 2012, 6177 samples were tested for LGV, of which 2138 were diagnosed with LGV. Variations in the number of diagnoses closely followed the pattern of samples tested. Enhanced surveillance information was collected on cases diagnosed from October 2004 until the end of 2010. Of the 1581 cases diagnosed to the end of 2010, enhanced surveillance data was available for 87% (1370/1581) of cases. The eight diagnoses seen in heterosexuals, and nine for which sexuality was unknown were excluded from further analysis.
Of the 1353 remaining cases, completion of data fields varied considerably: proctitis (100%), genital symptoms (100%), duration of symptoms (81%), age (99%), city (100%), HIV positive (97%), hepatitis C virus (HCV) antibody positive (80%), STI coinfection (100%), number of sexual partners (100%), number of new sexual contacts (100%), where new sexual contacts met (100%), location of sexual contact (87%), receptive anal intercourse (RAI) (69%), insertive anal intercourse (IAI) (79%), receptive fisting (RF) (52%), ROI (87%), IOI (86%), and sharing sex toys (46%). Most of the diagnoses (67%; 900/1353) were seen in London. Almost three-quarters (74%; 997/1353) of MSM reported genital symptoms, and virtually all (98%: 1331/1353) presented with proctitis. Two-thirds of cases were aged 35 years or more and 89% (1191/1332) were white. Coinfection was common: 82% (1082/1316) were diagnosed HIV positive, 20% (219/1088) were HCV antibody positive, and 36% (492/1353) were coinfected with another sexually transmitted infection, such as syphilis (any stage), gonorrhoea and genital herpes (primary and recurrent). At least one new sexual contact in the preceding 3 months was reported by 93% (1261/1353). Most (92%; 1092/1181) infections were acquired in the UK, 6% (73/1181) elsewhere in Europe and 1% (16/1181) outside of Europe. RAI was reported by 94% (1165/1243), IAI by 88% (945/1072), RF by 20% (145/710), ROI by 91% (1069/1180), and shared use of sex toys by 15% (95/623). Seventy-three per cent of the episodes of RAI, 77% of IAI, 77% of RF, 97% of ROI and 89% of sharing toys were classified as unprotected, namely, they occurred without use of barrier protection (condoms or latex). Repeat LGV infection was seen in 11% (142/1353) of cases.
Logistic regression analysis
There were 423 cases during the endemic phase and 488 cases during the growth phase (excluding 21 cases with repeat infection during these phases) (table 1). Growth phase cases were more likely to have met new sexual contacts at sex parties (11% vs 6%; p=0.014), to have had unprotected ROI (93% vs 86%; p 0.001), IOI (92% vs 85%; p<0.001) and sharing of sex toys (8% vs 4%; p=0.011), and to be diagnosed HIV positive (86% vs 80%; p=0.014) than those in the endemic phase (table 1). Growth and endemic-phase cases were equally likely to report unprotected RAI (71% vs 73%), to be HCV antibody positive (20% vs 19%) or to have a concurrent STI (37% vs 36%) (table 1). In the adjusted analysis of 757 complete cases, those in the growth phase were more likely to meet new contacts at sex parties (p=0.031) and to be HIV positive (p=0.045) (table 2). Reporting unprotected sharing of sex toys (p=0.072) was weakly associated with growth phase cases in the adjusted model 58) (table 2).
Comparison of characteristics of endemic and growth phase LGV cases (definitions in Methods): unadjusted estimates and 95% CIs
Risk factors associated with LGV cases in the growth phase compared with those in the endemic phase (definitions in Methods): adjusted estimates and 95% CIs
Discussion
The UK currently has the largest documented, ongoing LGV epidemic in MSM. Despite concerted control efforts, the epidemic has intensified, with over half the 2138 cases reported since 2003 having occurred since October 2009. As the epidemic has progressed, the profile of diagnoses—predominantly white, HIV-positive MSM frequently presenting with STI and HCV coinfections and engaging in high-risk sexual behaviours—has persisted.
Comprehensive enhanced national surveillance of over 1000 of these cases has provided unique insight into the recent epidemiology of LGV infection in MSM. There are few studies on factors associated with LGV transmission in MSM,3 ,7 ,9 ,10 and none with such extensive clinical and behavioural information on such a large number of men. However, as with any analysis based on passive surveillance data, a major weakness of this investigation was the extent to which information on some of the behavioural parameters was missing. More recent cases were typically less likely to have missing information, suggesting that reporting of clinical and behavioural information improved over time. Nevertheless, the large sample size allowed us to restrict our investigation to a complete-case analysis, thereby strengthening our principal findings.
The phase-specific epidemiological model provides a useful conceptual framework within which the development of an epidemic can be interpreted in relation to intervention and control strategies. The steep gradient of the epidemic curve between 2004 and 2005 likely reflected the development of diagnostic facilities and improved awareness and response. This period reflects a mixture of incident and prevalent cases as some patients who were diagnosed with LGV had experienced symptoms over several months and, in some cases, had been given a competing diagnosis before referral to GUM.5 Consequently, it is difficult to fit this early epidemic-stage epidemic within the phase-specific model. After the beginning of 2006, trends in diagnoses over time are unlikely to reflect changes in testing practice, as only symptomatic cases were tested, and consequently, the dataset reflects changes in MSM presenting to clinical services with symptoms. In terms of this investigation, initial control efforts were not sufficiently effective to eradicate the infection, and endemicity (phase IV) was indicated by the majority of cases being locally acquired. After a period of rapid epidemic growth (phase I), numbers fell into an oscillating plateau (phase II), suggesting that the infection has reset at a new hyperendemic level. The pattern of sexual mixing is thought to influence the likelihood of infection spreading and on the eventual prevalence, as the more tightly connected sexual networks are, the more likely it will be for infection to persist.15 This appears to be what has been seen within the LGV epidemic. Over time, the risk profile of the cases has remained largely unchanged, suggesting LGV continues to circulate in a highly sexually active core population of HIV-positive MSM.19 HIV prevalence has risen throughout the last decade as has the number of HIV-positive MSM on therapy.20 Seroadaptive behaviours intended to reduce the risk of HIV transmission (such as seeking unprotected sexual encounters with other HIV-positive men) among this growing population have likely increased the opportunity for the transmission of other STIs including LGV, and potentially HIV where HIV-negative MSM are part of the network.21
Yet, some important changes in the profile of cases appear to have emerged. During the growth phase, cases were more likely to report (predominantly unprotected) oral sex, but this is unlikely to reflect a shift towards the adoption of safer sexual practices. During the same period, more cases reported unprotected sharing of sex toys, and levels of unprotected RAI remained high and unchanged, being reported by almost three-quarters of all cases. There was also evidence of an underlying shift in preference for meeting partners at sex parties among this core population. That this shift coincided with a concomitant rise in LGV transmission could suggest that partnerships formed at sex parties may be inherently ‘riskier’. A study of young MSM in New York found that those attending sex parties were both HIV-positive and HIV-negative, had limited access to condoms and lubricant, and reported more casual sexual partners, unprotected anal sex, drug use and other psychosocial problems than those who did not.22 High-risk drug taking (including injecting of methamphetamine and mephedrone) by MSM at private sex parties in London, typically organised through networks based on social media, is of growing concern and is likely leading to greater disinhibition and sexual risk-taking.23 Controlling infection transmission in these environments is likely to be highly challenging and may require innovative and tailored public health interventions.
In 2010, Public Health England (formerly the Health Protection Agency) launched an initiative to improve awareness to LGV at sexual and social venues and internet sites used by MSM diagnosed with LGV and local Health Protection Units collaborated with Terrence Higgins Trust to encourage the display of health information and provide hygiene advice at ‘sex on premises’ venues.11 Leaflet campaigns and targeted press releases were also being employed to raise awareness and promote condom use and LGV testing of HIV-positive MSM during routine clinical care.24 It is tempting to speculate that the modest decline and plateauing of LGV diagnoses since late 2010 to its current hyperendemic state may have been at least partly in response to the more intensive approach to intervention, and suggests such activities ought to continue. Increased screening of asymptomatic MSM at extragenital sites for Chlamydia and gonorrhoea using nucleic acid amplification tests in response to new testing guidance may also have led to increased detection and treatment of presymptomatic LGV infection.25
Partner notification (PN) is crucial to the control of sexually transmitted infections, and a number of techniques were used. Patient-initiated PN was undertaken through direct contact with partners or using the Gay Men Fighting AIDS (GMFA) online resources (http://www.gmfa.org.uk), and provider-initiated PN was also used. Despite these efforts, the majority of partners remained uncontactable (Patrick French, pers. comm.). Consequently, PN success rates were probably well below what is recommended by the British Association for Sexual Health and HIV for the management of gonococcal infection in London.26 This raised concerns about a significant undiagnosed pool of infection and the potential for ongoing transmission.
To date, LGV infection control initiatives in the UK have focussed on raising awareness and testing and treating symptomatic cases as asymptomatic infection has been considered rare.12 However, this has been questioned, and investigations are currently underway to evaluate the extent to which asymptomatic infection may be contributing to LGV transmission in the UK.27 ,28 This will help inform any revisions to LGV infection control plans to ensure that all MSM infected with LGV, regardless of symptoms, are diagnosed and treated effectively. Nonetheless, infection control of LGV is unlikely to be achieved by better testing and treatment of cases alone. Raising awareness of LGV, its symptoms and how it can be prevented among MSM, especially HIV-positive MSM, is going to be crucial to curtail this epidemic.
The data we present are a cause for concern. They suggest there are highly active sexual networks of predominantly HIV-positive MSM that are increasingly engaging in unprotected sex in environments where public health interventions may have limited influence. This is likely fuelling the transmission of STIs, HCV and other sexually transmissible infections, such as Shigella flexneri.21 ,29–30 Reducing STI and HIV transmission among MSM is a serious public health challenge; concerted efforts to develop innovative internet-based interventions, and to strengthen STI prevention activities for this population are urgently required.
Key messages
-
The UK has the largest documented epidemic of lymphogranuloma venereum with over 2000 cases reported since 2004.
-
The rapid epidemic growth that began in 2009 coincided with an intensification of unprotected, high-risk sexual activity among HIV-positive men, increasingly linked to private sex parties.
-
Seroadaptive behaviours among highly active sexual networks of HIV-positive men who have sex with men are likely leading to greater transmission of STIs and other sexually transmissible infections.
-
Interventions should focus on developing new approaches to improve awareness and maximising opportunities for testing at every contact with clinical services.
Acknowledgments
We would like to thank members of the LGV Incident Group, past and present, and all clinicians who reported to enhanced LGV surveillance. We also thank all members, past and present, of the Public Health England Sexually Transmitted Bacteria Reference Unit who have been involved in processing specimens, and of the HIV and STI Department involved in the processing and analysis of enhanced LGV surveillance data. We are grateful to Victoria Gilbart for case follow-up, Anthony Brady and André Charlett for advice on the statistical analysis and Andrea Marongiu, Zheng Yin and Maria Solomou who helped coordinate data collection and follow-up.
References
Footnotes
-
Handling editor Jackie A Cassell.
-
Collaborators Past and present members of the LGV Incident Group: Barry Evans, Kevin Fenton, Heather Jebbari, (HIV & STI Department, Public Health England Colindale); Patrick French (Mortimer Market Centre, London); Gillian Dean, Andy Parkhouse, Zoe Warwick and Iain Reeves (Claude Nicol Centre, Brighton); Anne Sullivan, Sanjeeva Pallawela, Gary Seaton, James Hardie and Naa Torshie Annan (Chelsea and Westminster Hospital, London); Neil Irvine (Health Protection Agency Northern Ireland); John White (Guys and St Thomas's Hospital Trust, London); Neil Macdonald (Imperial College London, London); Kirstine Eastick (Scottish Bacterial Sexually Transmitted Infections Reference Laboratory); Andy Winter (HIV and Genitourinary Medicine, Sandyford Initiative, Glasgow); Lesley Wallace (Health Protection Scotland); Daniel Rh Thomas and Gemma Northey (National Public Health Service for Wales); Alexander Macmillan and Dan Clutterbuck (Edinburgh Royal Infirmary); Ben Tunstall, Marc Thompson and Rod Watson (Terrence Higgins Trust); Helen Maguire, Paul Crook and Josh Forde (Public Health England London Epidemiology Unit); Lorraine Hickey (HSE, Republic of Ireland).
-
Contributors GH, CI, IS and HW conceived the study. CI and SA developed the LGV testing reference service and managed specimen testing. IS, SC and CP managed the enhanced surveillance data and undertook all analyses. GH prepared the first draft, and all authors contributed to the final version of the manuscript.
-
Funding This work was supported by Public Health England.
-
Competing interests None.
-
Ethics approval National Information Governance Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.