Article Text

Abstract
Objectives To investigate the molecular epidemiology of isolates of Neisseria gonorrhoeae from Saskatchewan, Canada, using Neisseria gonorrhoeae multi antigen sequence typing (NG-MAST), and to assess associations between antimicrobial susceptibility (AMS) and specific strain types (STs).
Methods 320 consecutive gonococcal isolates, collected between 2003 and 2008, were typed by NG-MAST. STs were grouped if one of their alleles was common and the other differed by ≤1% in DNA sequence. AMS was determined by agar dilution (CLSI) to seven antibiotics.
Results N gonorrhoeae isolates were resolved into 82 individual NG-MAST STs and 18 NG-MAST ST groups with groups 25, 3655, 921, 3654, 3657 and 3656 comprising 53.4% (171/320) of the isolates. N gonorrhoeae isolates susceptible to all the tested antimicrobials were significantly (p<0.05) associated with ST 25 (87%). Other significant associations between ST and AMS included: ST 3654 and isolates with minimum inhibitory concentrations of ≥0.03 mg/L to third generation cephalosporins; ST 3711 (100%) and TRNG; and ST/group 3654 (43%) and chromosomal resistance to penicillin and tetracycline. Several NG-MAST STs/groups were significantly associated with isolates with chromosomal resistance to tetracycline. Isolates resistant to ciprofloxacin (n=5) and azithromycin (n=2) appeared as individual STs. Significant associations were observed among individual STs, sex and age of the patient, and regional and temporal distributions.
Conclusions Associations between N gonorrhoeae AMS and NG-MAST STs were identified and may be useful in predicting AMS regionally. Because STs in different countries vary considerably, the use of NG-MAST for the prediction of AMS globally requires further study.
- Antibiotic Sensitivity
- Neisseria Gonorrhoea
- Molecular Epidemiology
- Molecular Typing
Statistics from Altmetric.com
Introduction
Despite estimates of more than 106 million new cases annually worldwide, gonorrhoea, which is caused by the Gram-negative bacterial pathogen Neisseria gonorrhoeae, remains an under-reported sexually transmitted infection.1 The number of different antibiotics that can be used to treat gonococcal infections has become increasingly restricted due to the development of resistance in this microorganism.1 Currently, gonococcal infections are mostly treatable with third generation cephalosporins alone or in combination with azithromycin.2–4 However, reports of N gonorrhoeae strains with reduced susceptibility or resistance to third generation cephalosporins and treatment failures with these agents, especially with oral cephalosporins (eg, cefixime), have highlighted the urgent need to discover and assess new therapeutic regimens and agents.5 ,6 Consequently, the WHO has issued a global alert on potentially untreatable gonococcal infections and called for increased antimicrobial susceptibility (AMS) surveillance.1
Gonorrhoea transmission occurs in core groups of infected persons and bridging populations, with individuals in the bridging group acting as a link between the core groups and the general population.7 The effective identification of core groups and the gonococcal isolates they transmit is critical for the successful control of gonorrhoea.7 ,8 N gonorrhoeae isolate distribution can be ascertained through DNA sequence based typing schemes which identify isolates with common molecular characteristics thereby providing insight into presumptively linked cases.7 DNA sequence based typing methods, coupled with phylogenetic analysis, provide comprehensive information on the genetic relatedness of different isolates.9 Neisseria gonorrhoeae multi antigen sequence typing (NG-MAST), a DNA sequence based method, has high discriminatory power, reproducibility and enables comparisons of strain types (STs) regionally and internationally.8 This method has been used successfully to identify N gonorrhoeae circulating strains/clusters, investigate sexual networks, track strain transmission in sexual contacts and investigate the distribution of antibiotic resistant strains.8 ,9
Saskatchewan (SK) has one of the highest gonorrhoea rates of all provinces in Canada. In 2008, the gonorrhoea rate in SK was 131.3/100 000 people, 3.4 times higher than the national Canadian rates (38.2 cases/100 000).10 In our study, gonococcal strain distribution across the province (2003–2008) was determined by NG-MAST. NG-MAST STs were clustered into related groups and STs were analysed geographically and temporally. In addition, the association between specific NG-MAST STs and a particular AMS phenotype was evaluated.
Materials and methods
N gonorrhoeae isolate collection and identification
Cultures of N gonorrhoeae (n=320) were consecutively collected at the Saskatchewan Disease Control Laboratory (SDCL), Regina, Saskatchewan, between 2003 and 2008. There were 177 males (55.3%) and 143 (44.7%) females represented in this sample with ages ranging from 3 months to 70 years old (median age 24 years old; data not shown). In both sexes, the highest number of cases of gonorrhoea was in the 20–24 age group. None of the isolates represented duplicate specimens from the same patient.
Primary isolation and identification of N gonorrhoeae were completed as described previously.11 Isolates were stored at −80°C in Brain Heart Infusion medium (Difco BD Biosciences, Oakville, Ontario, Canada) containing 20% glycerol. Frozen stocks of N gonorrhoeae isolates were retrieved on GC Agar Medium Base (GCMB, Difco BD Biosciences, Oakville, Ontario, Canada) supplemented with 1% modified Kellogg's supplement (GCMBK) and incubated at 35°C with 5%–7% CO2 in a humid environment for 20–24 h.11 ,12 Isolates were reconfirmed as N gonorrhoeae using the oxidase test and Gram staining.11
Amplification of DNA sequences and molecular typing
DNA isolation was performed using overnight N gonorrhoeae growth collected from GCMBK plates and a Qiagen DNeasy Tissue Kit (Qiagen Inc., Valencia, California, USA). DNA was eluted in sterile distilled water and stored at −20°C. NG-MAST was performed on all DNA extracts as previously described.13 Following the purification of PCR products (PCR Purification Kit, Qiagen, Mississauga, Ontario, Canada), DNA sequences of both strands for each amplified locus were determined using an Applied Biosystems 3730×1 DNA Analyser (Plant Biotechnology Institute, National Research Council of Canada, Saskatoon, Saskatchewan, Canada). STs were grouped as one NG-MAST group if one identical allele (porB and tbpB) was shared and showed ≥99% similarity in other allele (≤5 bp difference for porB and ≤4 bp for tbpB) and comprised ≥2 isolates of the group.14
AMS testing
The minimum inhibitory concentrations (MICs) of 320 N gonorrhoeae isolates to penicillin, tetracycline, ciprofloxacin, azithromycin, cefixime, ceftriaxone and spectinomycin were determined, in duplicate using the agar dilution method of the Clinical and Laboratory Standards Institute.12 WHO strains B, C, F and K and ATCC 49226 were used as reference strains for AMS testing and antibiotics were purchased from Sigma Aldrich (Oakville, Ontario, Canada).12 ,15 ,16 β-lactamase production was determined using nitrocefin (Calbiochem, EMD Chemicals Inc., Darmstadt, Germany). AMS resistance criteria were those of CLSI12 and the Gonococcal Isolate Surveillance Project (USA).17
Verification and editing of DNA sequences
Chromas Lite (http://www.softpedia.com/get/Science-CAD/Chromas-Lite.shtml) was used to view chromatograms. ClustalW and Jalview (http://www.ebi.ac.uk/Tools/clustalw2/index.html) were used for alignment, viewing and editing of the DNA sequences of both complementary strands. porB and tbpB sequence from N gonorrhoeae FA19 (GenBank #M21289) and UU1008 (GenBank #2286066) were used as controls for NG-MAST analysis.13 DNA sequences of porB and tbpB fragments were submitted to the NG-MAST database (http://www.ng-mast.net)13 for the assignment of STs.
Statistical analysis
Yates’ χ2 tests were used for statistical analysis and significance was set at p value of <0.05.18
Results
AMS and NG-MAST STs
None of the gonococcal isolates displayed resistance or reduced susceptibility (ie, MIC≥0.25 mg/L) to cefixime and ceftriaxone and all were susceptible to spectinomycin. Penicillin resistance was observed in 4.7% (15/320) of the isolates; 86.7% (13/15) of these isolates carried chromosomal resistance to penicillin and tetracycline (ie, chromosomally resistant N gonorrhoeae (CMRNG)) and 13.3% (2/15) were penicillinase producing N gonorrhoeae (table 1). Tetracycline resistance was observed in 66.0% (212/320) of the isolates with 6.6% (14/212) carrying plasmid-mediated tetracycline resistance (tetracycline resistant N gonorrhoeae (TRNG)) and 93.3% (197/212) with chromosomally-mediated tetracycline resistance (CMTR) alone or in combination with resistance to other antibiotics. Low levels of resistance to ciprofloxacin (1.6%, 5/320) and azithromycin (0.63%, 2/320) were noted.
Neisseria gonorrhoeae multi antigen sequence typing STs of 320 Neisseria gonorrhoeae isolates and their association with antimicrobial susceptibility phenotypes
The 320 gonococcal isolates were resolved into 82 NG-MAST STs of which 55 were new to the NG-MAST data base. In all, 42 STs were associated with two or more N gonorrhoeae isolates and 40 STs were represented by a single isolate. Overall, 65.9% (211/320) of the isolates were classified into 15 individual NG-MAST STs (table 1) with the 10 most predominant STs being 25 (n=46), 3655 (n=23), 3654 (n=21), 3657 (n=15), 3672 (n=14), 3556 (n=13), 921 (n=13), 3656 (n=13), 3711 (n=10) and 508 (n=10) with half being identified for the first time in the NG-MAST data base. STs 3655, 3654, 3657, 3672, 3656, 3653, 3714, 3671 and 4585 were new STs and are unique to SK.
Significant associations were observed between individual STs and AMS profiles (table 1). Susceptible isolates were significantly associated with ST 25 (40/46, 87%, p<0.0001) and the remaining six isolates with the same ST were characterised as CMTR isolates (table 1). Interestingly, 58 of the 82 (70.7%) STs comprised isolates which were CMTR. The CMTR phenotype was significantly associated with STs 3655 (22/23, p=0.0002), 3672 (12/14, p=0.048) and 921 (12/13, p=0.0178). ST 3711 exclusively comprised TRNG isolates (table 1). The majority (9/13) of CMRNG were classified as ST 3654 (9/21, p<0.0001). Interestingly, STs 3656 and 508, isolates which were either susceptible, CMTR or CMRNG, shared the same NG-MAST porB allele (356) and had one base pair differences in their tbpB allele (821 and 28).
We examined whether there was any association between the 31 isolates having MICs of ≥0.03 mg/L to third generation cephalosporins (cefixime and ceftriaxone) and specific STs. These isolates were resolved into 19 STs including 3654 (32.2%; 10/31; p<0.0001), 3714 (n=2), 3655 (n=2), 3657 (n=2) and 15 single STs. Only ST 3654 was significantly associated with higher MICs to third generation cephalosporins.
Only a single isolate was identified with NG-MAST ST 1407, an ST which has been associated internationally with reduced susceptibility to third generation cephalosporins and resistance to ciprofloxacin.5 ,19 ,20 This isolate had MICs to cefixime and ceftriaxone of 0.125 and 0.06 mg/L, respectively, was resistant to ciprofloxacin, and was a TRNG isolate carrying the Dutch type tetM determinant (data not shown). The NG-MAST porB (908) and tbpB (110) alleles for the isolate typed as ST 1407 were not observed in any other ST observed in this study.
Combining NG-MAST STs into ST groups
NG-MAST STs which shared an identical porB or tbpB allele and which differed by ≤1% (≤5 bp difference in porB and ≤4 bp in tbpB) in the other allele were reclassified into NG-MAST groups.14 Each group was named after the predominant ST in that group.14 Based on this scheme (table 2), individual STs were classified into 18 groups, while 33 STs remained ungroupable. Of these 18 ST groups, over 50% (171/320) of the isolates belonged to six NG-MAST groups (25 (n=52, 16.3%), 3655 (n=35, 11%), 921 (n=27, 8.4%), 3654 (n=23, 7.2%), 3657 (n=20, 6.3%) and 3656 (n=14, 4.4%)). Associations between AMS and NG-MAST groups were identical to the associations observed with individual STs. For example, susceptible isolates were significantly associated with NG-MAST ST and NG-MAST group 25 (44/52, 84.6%, p<0.0001) (table 2). NG-MAST groups 3655 (32/35, 91.4%, p<0.0001), 921 (25/27, 92.6%, p=0.0002) and 3672 (12/14, 85.7%, p=0.048) were significantly associated with the CMTR phenotype. CMRNG were significantly related to NG-MAST group 3654 (9/23, 39.1%, p<0.0001). Isolates with phenotype CMTR/CipR (n=2, 0.6%) appeared as NG-MAST STs 3116 and 3668 but shared the same tbpB allele (25) and had a 1 bp difference in their porB alleles (2202 and 1884) (data not shown). These two isolates were grouped as NG-MAST group 3116 (table 2).
Neisseria gonorrhoeae multi antigen sequence typing (NG-MAST) groups based on porB and tbpB sequence similarity
Regional and temporal distribution of STs in SK
Significant regional distributions were detected with six predominant STs (figure 1) of which five were exclusive to SK. ST 25 (23/46, 50%, p<0.0001) and ST 3655 (12/23, 52.2, p=0.0018) had a significant presence in the northern city of Prince Albert. ST 3654 largely comprised isolates from Regina in southern SK (15/21, 71.4%, p<0.0001). In Saskatoon (central SK), STs 3656 (8/13, 61.5%, p=0.002) and 3657 (9/15, 60%, p=0.0042) predominated, while STs 3672, 3714 and 4585 were prevalent in La Ronge (6/14, 43%, p<0.0001), Moose Jaw (3/7, 43%, p<0.0001) and Nipawin (4/6, 67%, p<0.0001) (data not shown). NG-MAST groups 25 (23/53, 44.2%, p=0.0002) and 3654 (17/23, 74%, p<0.0001) were significantly associated with Prince Albert. NG-MAST groups 3656 (8/14, 57.1%, p=0.01) and 3657 (10/22, 45.5, p=0.04) had significant association with Saskatoon.

Regional distribution of predominant Neisseria gonorrhoeae multi antigen sequence typing strain types (≥10 isolates) in Saskatchewan. Others: Canora, Fort Qu'Appelle, Grenhill, Ile a la Crosse, Laloche, Lanigan, Lloydminister, La Ronge, Macklin, Meadow Lake Melfort, Moose Jaw Nipawin, North Battleford, Preeceville, Red Earth, Turtleford Wollaston Reserve, Wynyard and Yorkton. Map redacted from.33 *p<0.05 was considered statistically significant.
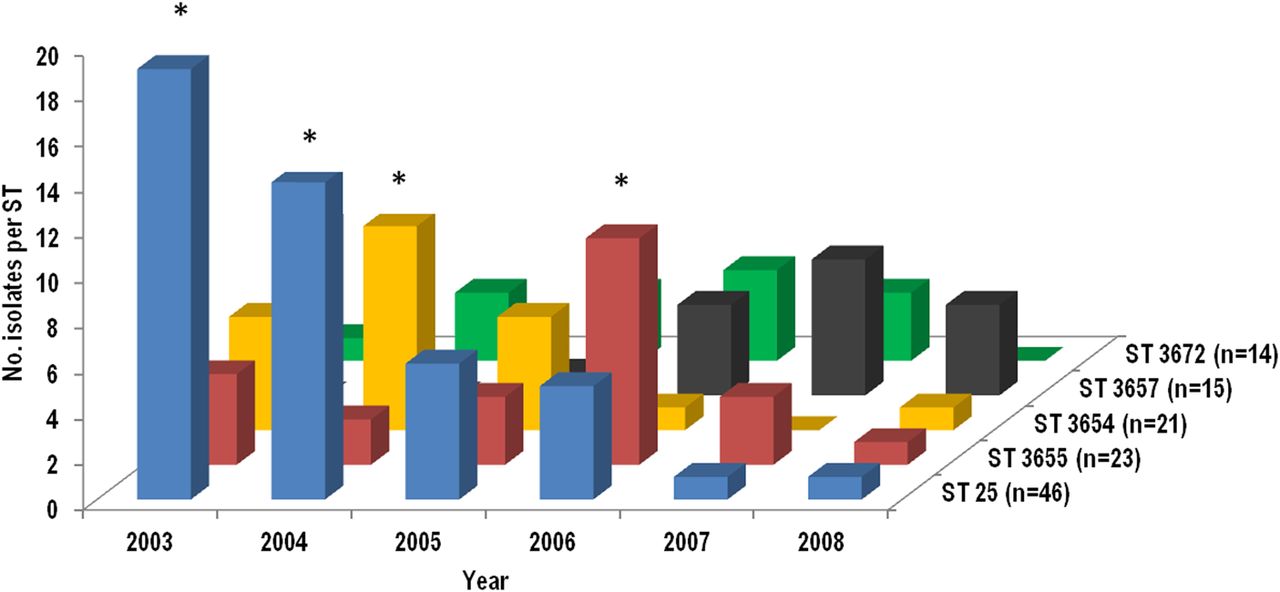
Only three STs (25, 3654 and 3655) were present throughout the entire study period (2003–2008; figure 2) and the numbers of gonococcal isolates with these STs varied over time. For example, the number of N gonorrhoeae isolates with ST 25 was significantly higher in 2003 (31.7%, 19/60, p<0.0001) and 2004 (23.7%, 14/59, p=0.032) and declined thereafter to only 2.43% (1/41) in 2008. Also, the incidence of ST 3654 was significantly higher (15.3%, 9/59, p=0.0071) in 2004 and the numbers of isolates with this ST decreased afterwards. Isolates with ST 3655 (10/23, 43.5%, p=0.0015) were highest in 2006. Other STs among the 10 most prevalent appeared only in some years; ST 3711 was observed in 2004 (5%, 3/59), 2005 (3.8%, 2/52) and 2006 (9%, 5/55, p=0.017). ST 3556 was present only in 2007 (11.3%, 6/53, p=0.023) and 2008 (12.2%, 5/41, p=0.016).

{kind=link}
{kind=link}
Temporal distribution of predominant Neisseria gonorrhoeae multi antigen sequence typing (NG-MAST) strain types (STs) (≥10 isolates) in Saskatchewan. NG-MAST STs 25, 3655 and 3654 has shown declining trend in the prevalence after 2003, 2006 and 2004 respectively. *p<0.05 was considered statistically significant.
Discussion
This study describes the unique strain distribution of N gonorrhoeae isolates from SK. It appears that the strain population in SK as determined by NG-MAST is quite unique; nine of the 15 predominant NG-MAST STs were new to NG-MAST database. The most frequently (≥10 isolates) observed gonococcal STs in this study have not been reported as predominating in previously conducted studies in Canada.21–25 None of the gonococcal STs identified in various Canadian studies predominated in the isolates in the present study and, except for ST 3556 (4%, 13/320), they appeared only as sporadic isolates (eg, ST 2 (1.25%, 4/320); 51 (0.6%, 2/320); 225 (0.3%, 1/320); 1407 (0.3%, 1/320) and 3116 (0.3%, 1/320).21–25 Further, except for the report examining cephalosporin susceptibility,24 in most of these Canadian studies, associations between NG-MAST STs and various AMS profiles were not analysed. It would be important to determine these associations to develop a more comprehensive overview of the diversity of STs and their AMS profiles from different Canadian regions. Such an analysis would provide a better understanding of the transmission of antibiotic resistant N gonorrhoeae strains across the country permitting the development of specific public health preventive measures and interventions based on both regional and aggregated national data.
Internationally, a number of studies have shown an association between N gonorrhoeae STs and resistance to ciprofloxacin (ie, STs 147 (Wales, Scotland, France);26–28 225 (Canada, Scotland, Wales, France);23 ,26–28 338 (Scotland);29 404, 597 and 1636 (Wales);27 and 1407 and 3550 (Europe, Canada)).6 ,19 ,23 ,25 The five ciprofloxacin resistant isolates in our study all had dissimilar STs, one of which was 1407. Two azithromycin resistant isolates were noted in our study and they had different STs from those previously reported as being associated with azithromycin resistance, that is, NG-MAST STs 470, 649 and 2992 (Scotland) and 668 and 7199 (Canada).23 ,25 ,30 Gonococcal isolates with reduced susceptibility to third generation cephalosporins have been reported to be associated with NG-MAST STs 225 (Canada, France),23–25 ,28 1407 (Canada, San Francisco, the USA, Europe),14 ,19 ,21–25 ,31 3158 (Canada),23–25 3307 (Canada)23 ,25 and 3550 (Canada, France, San Francisco).23–25 ,31 Whiley et al reported 13 different NG-MAST STs in gonococcal isolates with ceftriaxone MICs ranging between 0.016 and 0.125 in Australia.32 Only STs 225 (n=1) and 1407 (n=1) in our study were similar to those reported in other regions. Few international studies have reported associations between gonococcal penicillin or tetracycline resistance and NG-MAST STs. Penicillin resistant and TRNG isolates reported in other Canadian studies were associated with NG-MAST STs 1407, 3307, 3550, 3158 and 4266 while tetracycline resistance alone was observed in isolates with STs 63, 147, 225, 470 and 766. These STs differ from the ST associations with penicillin and tetracycline resistance found in the present study.23 ,25 Palmer et al also reported high levels (92%–99.5%) of concordance between NG-MAST STs and different AMS phenotypes including susceptibility to penicillin and tetracycline, but these STs were different from those reported in Canadian studies.23–26 Although it has been suggested that NG-MAST STs might be used to predict gonococcal AMS,26 both Canadian and international variability in the association of a particular ST with a specific AMS phenotype suggests otherwise. Because STs vary considerably around the world, a more comprehensive analysis of individual STs and their association with a particular AMS phenotype should be undertaken in order to ascertain whether a particular NG-MAST ST is useful for predicting AMS internationally or only regionally. All the associations between NG-MAST STs and N gonorrhoeae AMS phenotypes observed in this study, especially the significant association of susceptibility with ST 25, TRNG with ST 3711, CMRNG with ST 3654, and CMTR with STs 921, 3655 and 3672, have never been previously reported.
The small number of NG-MAST groups formed by combining individual NG-MAST STs revealed that the gonococcal population in SK is highly related, an observation made earlier on the basis of multi-locus sequence typing (MLST) analysis.33 More than 50% gonococcal isolates were clustered as six NG-MAST groups compared with 10 individual NG-MAST STs. These findings clearly show that minor variations in hyper-variable genes used in NG-MAST, particularly porB, result in the assignation of new STs to gonococcal isolates which are largely similar. The STs identified by typing methods based on hyper-variable loci, that is, porB or tbpB, gradually diminish from the population and appear as new STs often owing to minor variations in these loci,8 ,33 as observed for STs 508 and 3656 and 3116 and 3668 in this study. Owing to the high diversity of STs generated by NG-MAST, these findings support the conclusion that NG-MAST is a better scheme for molecular epidemiological studies of N gonorrhoeae isolates collected over short periods of time.8
Some of the predominant STs observed in this study showed significant association with specific time periods (eg, ST 25 (2003 and 2004), 3655 (2006), 3556 (2007 and 2008)) and localities (eg, STs 25 (Prince Albert), 3654 (Regina), 3656 (Saskatoon) and 3714 (Moose Jaw)), as reported previously in other regions.21–32 These results suggest that these gonococcal STs were most likely circulating in localised sexual networks. Furthermore, some of the predominant STs identified in this study can be designated as outbreak strains (eg, Prince Albert, ST 25, 2003, 61.1% of isolates). Such molecular findings, coupled with approaches such as contact tracing, might be used for the better identification of sexual networks and outbreaks to prevent the spread and transmission of gonorrhoea.8 ,9 ,29
NG-MAST ST 1407 is now one of the most successfully distributed N gonorrhoeae STs worldwide and is especially notable because of its association with resistance to penicillin, tetracycline (TRNG), ciprofloxacin and reduced susceptibility to third generation cephalosporins and treatment failures to third generation cephalosporins.5 ,19 ,20 We identified only one isolate with this ST during our 6-year study period. Interestingly ST 1407 was first identified in Scotland in 200720 and the isolate characterised with this ST in the present study was recovered in 2006 suggesting that this ST may have been circulating earlier than first thought.
The N gonorrhoeae isolates tested for NG-MAST and AMS in this study represented about 5% of cases reported over the period.10 Although culture is required for AMS testing, nucleic acid amplification testing is the method most used for identifying gonococcal isolates in SK. Thus, the exact NG-MAST distribution in the province may differ from our results which reflect only cultured isolates. The inclusion of validated, non-culture methods for NG-MAST determination would provide a better overview of N gonorrhoeae ST distribution. Further, since the association of AMS and NG-MAST ST may differ regionally, it would be appropriate for each region to test the hypothesis that NG-MAST ST predicts AMS. In cases where gonococcal isolates might be susceptible to antibiotics which are no longer recommended for treatment, the association of NG-MAST ST and susceptibility may support the rationale use of these antibiotics in the treatment of gonococcal infections.
Key messages
-
A total of 320 isolates of Neisseria gonorrhoeae from Saskatchewan were typed by Neisseria gonorrhoeae multi antigen sequence typing (NG-MAST) into 88 strain types (STs) of which 55 were new to the NG-MAST data base.
-
Certain STs were significantly associated with antimicrobial susceptibility phenotypes—for example, ST 25 and susceptibility; ST 3654 with third generation cephalosporin minimum inhibitory concentrations ≥0.03 mg/L.
-
Different STs had significant temporal and geographic associations.
References
Footnotes
-
Handling editor Jackie A Cassell
-
Acknowledgements The authors thank Cherise Hedlin (University of Saskatchewan) and Evelyn Nagle (SDCL) for technical assistance.
-
Contributors This work comprises part of the PhD thesis of SDT who produced and analysed the data, drafted the paper and participated in all revisions; JRD is the corresponding author, collaborated with the SDCL, supervised the research of SDT and had primary, editorial and analytical input into each draft of the manuscript; GBH and PNL provided identified Neisseria gonorrhoeae isolates and epidemiological and clinical information and critiqued and approved the manuscript.
-
Funding This work was supported by the Saskatchewan Health Research Foundation (Grant# 9127) and University of Saskatchewan funding to JRD.
-
Competing interests None.
-
Ethics approval University of Saskatchewan.
-
Provenance and peer review Not commissioned; externally peer reviewed.