Article Text

Abstract
Objectives To examine outcomes of a peer-led, community-based intervention providing rapid HIV testing and case management for linkage to care for untested men who have sex with men (MSM) in China.
Methods Rapid HIV testing was performed by trained peer volunteers of a community-based organisation (CBO) in three cities of Jiangsu province at MSM-oriented venues. MSM screened positive were referred and accompanied to local government health agencies (Centres for Disease Control and Prevention (CDC)) for confirmatory HIV testing and provided social support for up to 1 month. Data for the programme were compared with sentinel surveillance surveys of MSM conducted by the national and provincial CDC in the province during the same year to assess differences in the populations reached, in HIV positivity, and linkage to HIV care.
Results A total of 512 previously untested MSM were tested by the CBO programme in 6 months. Compared with those in the surveillance surveys, MSM tested by the CBO were significantly more likely to be younger, single, non-resident of the province, more educated and used condoms less frequently. Higher proportions of HIV-positive MSM screened by the CBO received their confirmatory test results (98.1% vs 72.6%, p<0.001) and linked to care (90.4% vs 42.0%, p<0.001).
Conclusions Trained peers providing rapid HIV testing with social support and case management through the early period following diagnosis can efficiently expand HIV testing and improve linkage to care among MSM in China.
- HIV
- CHINA
- TESTING
- GAY MEN
Statistics from Altmetric.com
Introduction
The proportion of men who have sex with men (MSM) in the HIV epidemic of China appears to be growing.1 Epidemiological studies of MSM suggest a national prevalence of HIV at 4.9%, continuing high incidence and high levels of risk behaviour.2–7
However, many MSM in China have never tested for HIV, with coverage estimated between 25% and 49%.8–11 As a consequence, few HIV-positive MSM are aware of their infection. For example, a study in Beijing found only 5 of 36 HIV-positive MSM (13.9%) detected in the survey were aware of their infection.11 Barriers included not knowing where to get tested and fear of discrimination if positive. Low HIV status awareness may drive transmission among MSM for behavioural and biological reasons. Persons with HIV who are aware of their status are more likely to take precautions to prevent transmission.12–16 One randomised controlled trial among heterosexual couples demonstrated reduction of HIV transmission to partners from persons on antiretroviral therapy (ART).17 Meanwhile, evidence indicates earlier treatment of HIV is beneficial to the individual.18
In order to maximise the benefits of ART, high levels of engagement in services are required at multiple steps.19 Figure 1 illustrates the ‘treatment cascade’ with adaptations for the Chinese context. In many provinces of China, initial HIV-positive ELISA tests require western blot confirmation by the Centres for Disease Control and Prevention (CDC) for diagnosis. Following a wait of 2–7 days for confirmatory results, patients require CDC follow-up for case management to HIV care. Linkage to care is made in the jurisdiction of diagnosis if the patient is an official/permanent resident; otherwise linkage is made through referral to their place of residence. Prescription of ART depends on the stage of HIV infection, in practice based on CD4 count. In 2012, the CD4 criterion for ART initiation in China was ≤350 cell/mm3.20 Viral load suppression (the final stage of the cascade) depends on adherence and drug resistance.
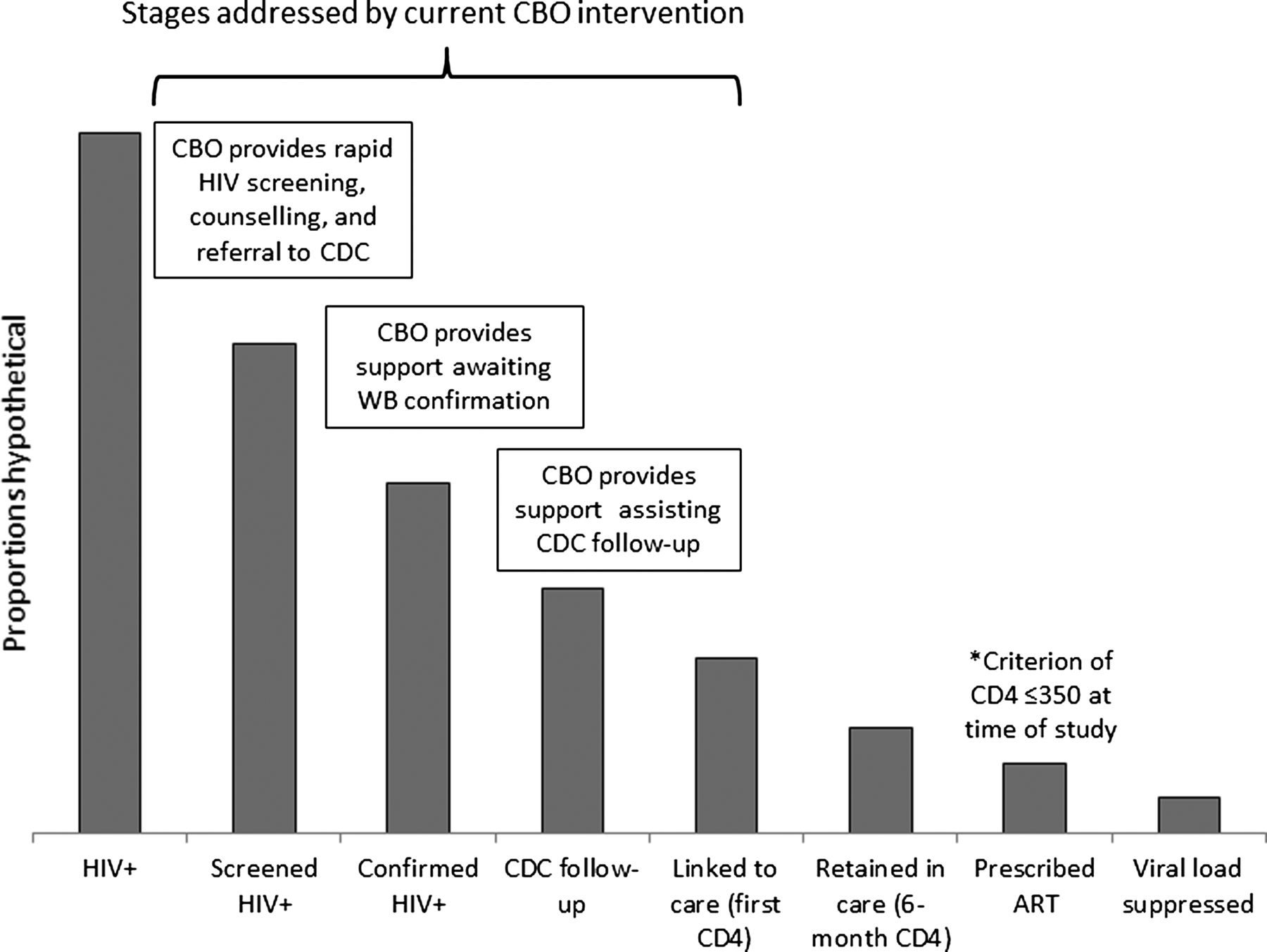
Stages of the HIV continuum of care and points of intervention of the community-based organisation peer counsellor/case manager programme for men who have sex with men, Jiangsu province, China, 2012.
In brief, there are formidable barriers to achieving a high level of treatment among MSM with HIV in China. While all steps need to be maximised, clarifying which steps produce the greatest losses will help efficiently target interventions. For Chinese MSM, data indicate great loss from the first to second step in that the majority of HIV-positive MSM have not tested.12–15 Confirmation of initial screen and follow-up to first CD4 test by the CDC affect losses to linkage to care. For example, results from China-Gates Foundation's HIV prevention programme found a 21% loss from initial HIV-positive screen to confirmatory testing and 34% loss from confirmation to first CD4.21
In 2011, the State Council of China issued the ‘Five Expands, Six Strengthens’ strategy,22 calling for increased HIV testing among populations at risk and care and support for those infected. During early implementation, particularly low coverage of HIV testing and linkage to and retention in care were notable for MSM. The present study therefore had the objective to assess an operational model to expand HIV testing and link HIV-positive individuals to care through a government–community-based organisation (CBO) collaboration. The provincial CDC and the Chinese Association of STD/HIV Prevention and Control, a professional group working with government and communities for HIV prevention, funded and provided technical support to four grass-root MSM CBOs in three cities of Jiangsu to implement the current intervention. The CBOs conducted a pilot rapid HIV testing programme with social support and case management facilitation by peer counsellors focusing on MSM who have never tested previously. The present report describes the intervention implementation and assesses the effectiveness of the CBO model.
Methods
Intervention
Our study evaluates an MSM peer-led, CBO-based, mobile rapid HIV testing programme on the outcomes of reaching previously untested MSM, linkage to care of those confirmed HIV positive, and, for Jiangsu residents, retention in care to 6 months.
For the purpose of this pilot intervention, the Jiangsu provincial CDC authorised MSM community members be trained to provide counselling with HIV rapid testing at gay-oriented venues in three cities. The programme required the CBO to refer MSM initially screened HIV positive to the local CDC for repeat and confirmatory testing by western blot. The programme also provided social support and case management up to the point of initiating their enrolment in HIV care with the CDC if a Jiangsu resident or to referral if their residence is elsewhere.
The study was conducted from 1 January to 30 June 2012. Seven teams were established in three cities, consisting of 28 MSM peer volunteers trained for 2 days on HIV knowledge, administering rapid testing, pretest and post-test counselling, maintaining confidentiality and procedures for referral and follow-up for HIV-positive individuals according to national guidelines.23 The programme's services were publicised to the MSM community through gay-oriented websites, posters and leaflets distributed at venues, mobile phone messages and word of mouth along social networks.
Study subjects
Men who ever engaged in anal or oral sex with a man, 18 years or older, but never tested for HIV were eligible. Participants were recruited through snowball sampling by peers at venues frequented by the community, including gay bars, clubs, bathhouses, cruising areas and hotels. Working with owners and managers, the team conducted HIV testing in a private room within the venue, a room at a venue nearby or in a mobile van. Peers approached men at venues, screened for eligibility, explained the procedures and offered rapid HIV testing. Those interested provided verbal consent. Subsequent participants were referred at the venues by previous participants. A target of 512 MSM was set for the study.
HIV counselling, testing, referral and linkage
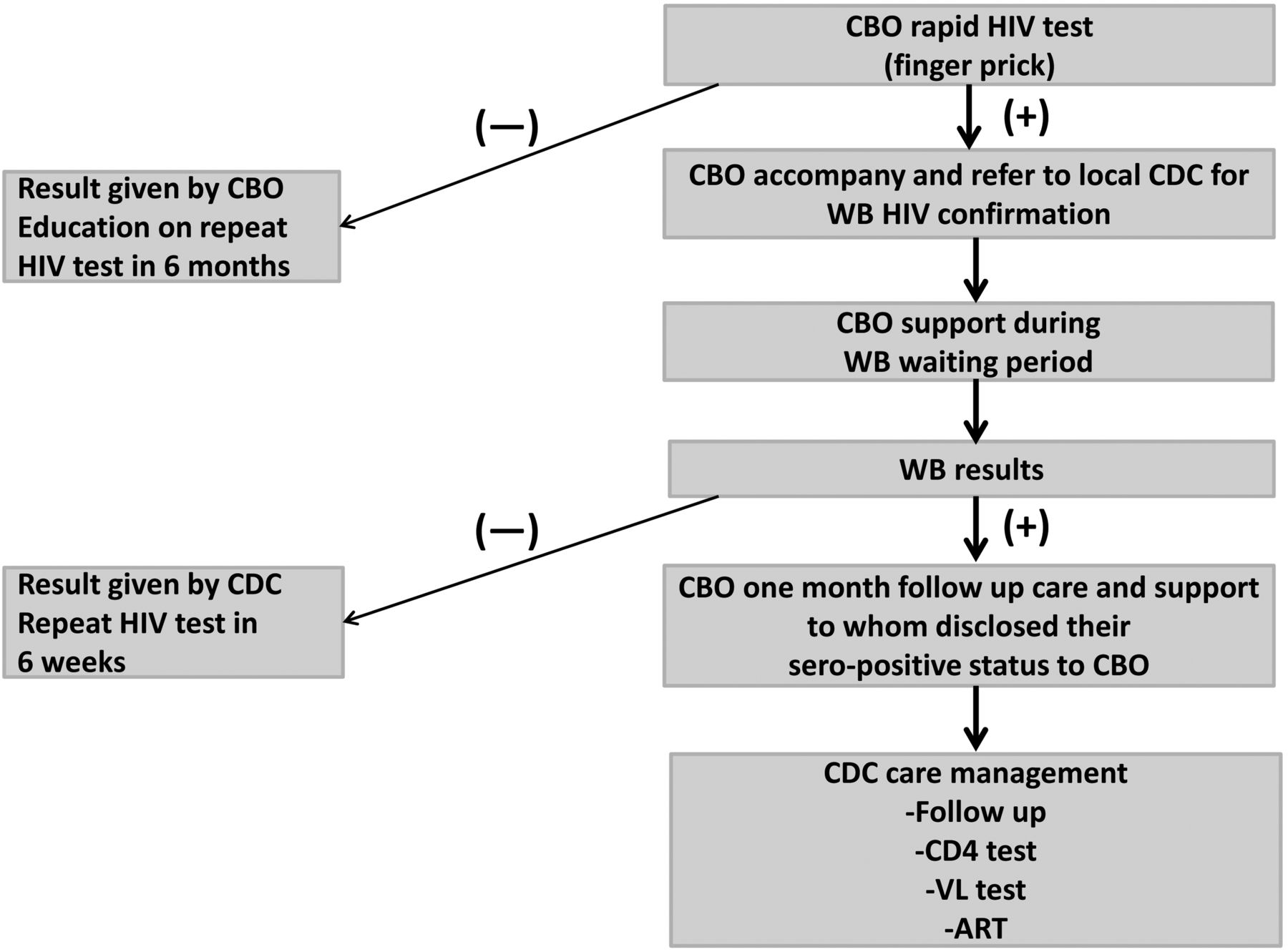
MSM peers were trained and certified in HIV counselling for pretest and post-test sessions according to national standards.23 After discussing the means of acquiring and preventing HIV infection and the clients’ behaviour, individualised risk reduction counselling was done. Clients were screened for their readiness for receiving results and plans if positive. The window period and the need for repeat testing for recent risk and periodic testing with on-going risk were explained as well as the potential for false positive test results and the need for further repeat testing and follow-up by the CDC. Following pretest counselling, a finger-prick rapid HIV test was performed by the peer in the private room or van and screening test results were disclosed with post-test counselling. Participants with negative results were informed by the peer counsellors directly and no further follow-up was required, apart from encouraging repeat testing if risk was recent (ie, potential window period) in 6 weeks and future regular testing if risk continued. For MSM screening positive, the peer counsellors made a referral to the local CDC for repeat and confirmatory testing and an appointment to accompany the participant to the site. During the period of waiting for confirmatory results, typically 2–7 days, at least one contact method (phone, face-to-face or website chat) was offered by peers to help reduce participants’ anxiety, answer questions related to HIV, and provide behavioural change education. In the study, no false positives were observed; however, if they were to occur participants would be given the negative results by CDC and recommended to take another HIV test in 6 weeks. For MSM confirmed HIV positive, an additional 1 month of contacts were offered by the CBO to those who were willing to disclose their confirmed seropositive status. These sessions addressed the concerns of those newly diagnosed and helped navigate the CDC system. These contacts also included further HIV-related information, psychological and social support, suicide prevention and STD referrals. CDC staff undertook follow-up care thereafter, including free CD4 testing and when appropriate ART. Figure 2 describes the procedures of the rapid HIV test, referral and follow-up care provided by the CBO.

Operational model for a peer community-based organisation intervention, including rapid HIV screening, linkage to care and case management for men who have sex with men, Jiangsu province, China, 2012.
Measures
Prior to pretest counselling, a brief standardised questionnaire was administered to participants face-to-face to collect demographics, condom use in the last 6 months, and history of STD in the past year. For HIV-positive men engaging peer case management, a quick survey including follow-up by the CDC and CD4 testing were collected by the CBO at 6 months. Participants did not receive incentives.
Comparison population
Although the study was not designed as a randomised control trial or quasi experiment, HIV serological surveys of the MSM population conducted for the purpose of surveillance provided a comparison group to see differences in which MSM were reached, which were detected as positive, and subsequent linkage outcomes. These ‘sentinel surveillance surveys’ were conducted by provincial and local CDC staff between April and June 2012 at 14 sites in Jiangsu. The surveillance surveys followed a uniform protocol across China.24 In brief, sampling and procedures resembled the CBO rapid HIV testing pilot programme in several aspects. MSM were recruited at diverse gay-identified venues using snowball sampling. Eligibility criteria were men who have ever engaged in anal or oral sex with a man and age 18 years or older. Newly diagnosed HIV-positive MSM in the surveillance surveys were referred and reported to the central HIV case reporting and management system where data on their linkage to care and retention at 6 months were available. In the surveillance surveys, no previously diagnosed HIV-positive MSM were noted. Beyond in the procedures of the surveillance surveys, the CBO pilot study used peer rather than CDC staff counsellors, accompanied MSM personally to confirmatory testing, and provided social support and case management facilitation through engagement in HIV care.
Laboratory methods
Initial HIV fingerprick rapid testing was performed using the Diagnostic Kit for Antibody to Human Immunodeficiency Virus (1+2) assay (Colloidal Gold, NewScen Coast Bio-pharmaceutical Co. Ltd, Tianjin, China). An ELISA (Beijing Wantai Biological Pharmacy Enterprise Co., Ltd) was used for repeat HIV antibody testing. Confirmatory testing was performed by western blot (MP Biomedicals Asia Pacific., Ltd, Singapore).
Analysis
Questionnaire-based data and laboratory results were recorded, double entered and compiled with Epi Data (The Epi Data Association Odense, Denmark). SPSS V.16.0 (SPSS Inc) was used for statistical analysis. χ2 tests were conducted to compare characteristics of MSM in the intervention study to those in the surveillance surveys.
Results
Table 1 presents characteristics of MSM recruited and screening HIV positive through the CBO programme and surveillance surveys. A total of 512 MSM received HIV rapid testing from the CBO during the 6-month pilot period. Most (70.1%) were under the age of 30 years, 71.1% were unmarried, 65.2% were official Jiangsu residents and 90.4% had education above senior middle school. Only 21.9% reported consistent condom use in the last 6 months. Compared with MSM in the surveillance surveys, MSM reached by the CBO were more likely to be younger, unmarried, migrant, better educated and have engaged unprotected anal intercourse (p values <0.001). By design and eligibility, none of the MSM recruited by the CBO programme had tested previously while 54.0% in the surveillance surveys had tested in the last year. HIV seropositivity among CBO-recruited MSM (10.2%) was comparable to the surveillance surveys (9.4%, p=0.652). As for MSM screening HIV positive, those detected in the CBO programme were more likely to be younger, unmarried, migrant, having engaged unprotected anal intercourse and having syphilis than those detected in the surveillance surveys.
Characteristic of men who have sex with men (MSM) recruited and screening HIV-positive through a peer-led community-based organisation (CBO) testing programme and through sentinel surveillance surveys, Jiangsu province, China, 2012
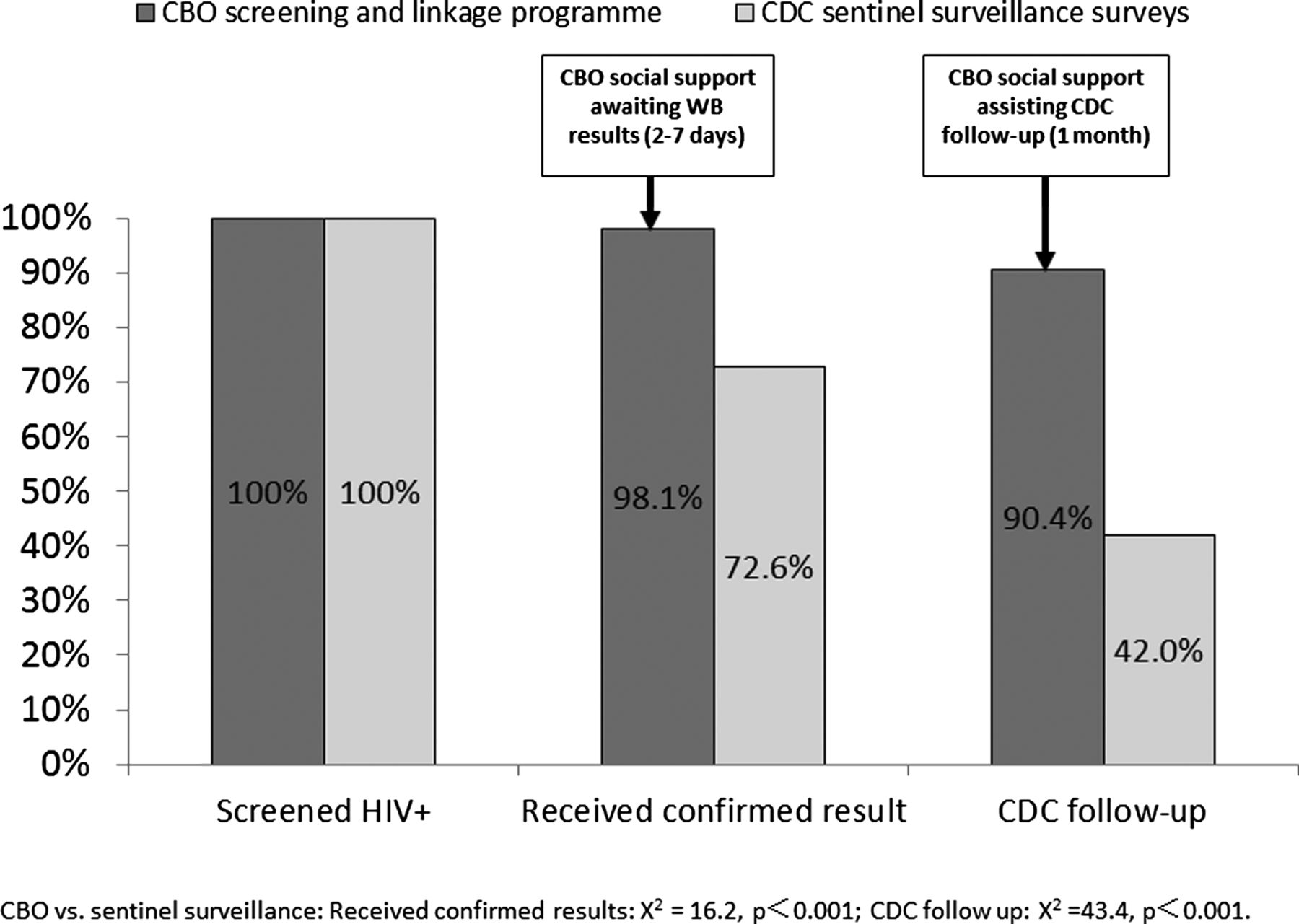
Figure 3 shows the proportion of MSM screened HIV positive who received confirmatory results and the proportion linked to care by the CBO programme compared with the surveillance surveys. Of the 52 MSM screened HIV positive by the CBO, 51 (98.1%) were accompanied, supported and referred to the local CDC and received their confirmatory results. During the 1-month period prior to or after entering CDC follow-up for linkage to care, 47 of the 52 (90.4%) were provided further social support and care and retained successfully in case management. By comparison, fewer MSM (304 of 419, 72.6%, vs 98.1%, p<0.001) received their confirmatory results after initial screening in the surveillance surveys fewer still were successfully contacted by the CDC to initiate or refer to care (176 of 419, 42.0%, vs 90.4%, p<0.001).
{kind=link}
{kind=link}
{kind=link}
Attrition of HIV-positive men who have sex with men (MSM) from diagnosis through confirmation and linkage to care; community-based rapid HIV screening, linkage to care and case management programme compared with MSM recruited through sentinel surveillance surveys, Jiangsu province, China, 2012.
Comparisons of retention in care to 6 months could be made for residents of Jiangsu province who were successfully contacted and initially linked to care. Of HIV-positive MSM, 32 identified by the CBO programme compared with 172 in the surveillance surveys were Jiangsu residents and initially linked to care. Of the CBO-identified HIV-positive residents, 29 (90.6%) had a CD4 test at 6 months compared with 163 (94.8%, p=0.361) recruited through the surveillance surveys.
Discussion
A government-supported pilot project that authorised, trained and mobilised CBOs to recruit MSM for rapid HIV testing in China reached a large number of never-tested MSM and increased linkage to HIV care for those newly diagnosed. The intervention informed over 500 MSM of their HIV serostatus, ensured confirmatory results were received for all but one and linked over 90% of new diagnoses to care. Our data support the operational model for the effective expansion of HIV testing and linkage to care for Chinese MSM.
We perceive other advantages of the programme. Peers providing convenient, fast services in a MSM-friendly manner in familiar community settings reduced many barriers. The approach may particularly lessen anxiety for MSM who have never tested before, easing the current test and subsequent tests sought elsewhere. Satisfied clients were willing to refer peers, reaching several hundred untested MSM. Thus, the intervention was able to circumvent several important barriers to HIV testing among Chinese MSM, including lack of awareness where to test, the perceived stigma and discrimination associated with government-supported clinics and inconveniences such as longer wait time for standard blood test results and limited after work hours.9 ,11 ,25 ,26 The peer-based strategy also reached demographically different populations, including younger and migrant MSM, and MSM less likely to use condoms compared with those accessed through surveillance surveys.
In addition to convenience and trust placed in MSM peers to test, we believe positive effects on linkage to services can be attributed to the social support provided throughout the critical period following initial test through CDC confirmation and engagement in care. Unlike conventional testing programmes, the CBO provided instant referral and accompanying to the CDC after positive rapid screening, social support while awaiting confirmatory results, and a 1-month period of support to assist case management by the CDC system. Receiving social support at the early stage following diagnosis can reduce individuals’ stress and anxiety and better prepare them for entry into care. Within the Chinese context, peer counsellors might be the only immediate support MSM are able to access and willing to accept, particularly if they are reluctant to disclose HIV and MSM status to family, friends or health providers for fear of rejection and discrimination.27 A lesson from our pilot project is that support needs to be continuously available to newly diagnosed MSM until they are fully engaged in care.
Our data also reveal potential weaknesses in the cascade of engagement in HIV care for MSM in China. While the CBO programme linked a higher proportion of newly diagnosed men to care, once in care the CBO intervention may not improve subsequent retention as compared with MSM entering through the surveillance surveys. Further peer support or alternative interventions, such as HIV-positive peer groups, are needed. By analogy, peer interventions may also be needed to help locate and encourage defaulters to return to care and to maximise ART adherence. Another potential weakness is the linkage to care of non-Jiangsu residents. While we cannot verify if referrals to out-of-province jurisdictions were completed, returning to areas that may be at great distance from Jiangsu and disruption of employment are likely to be substantial barriers. Loss to follow-up is also likely to occur before ART prescription. The CD4 criterion for ART initiation at the time of the study was ≤350 cell/mm3. While the criterion was subsequently raised to ≤500 cell/mm3, losses may occur in comparison to offering treatment to all persons with HIV as in the USA.28 As of writing, several cities of China, including Nanjing in Jiangsu province, are pilot testing the offering of ART to MSM regardless of CD4 count.
We recognise limitations of our data. While MSM recruited through the surveillance surveys were used for comparison to assess characteristics of the community reached and outcomes for linkage to care through an alternate approach, the design did not have a random or truly comparable control group. Rather, the outcomes highlight that different MSM are reached by different approaches. Moreover, we have no gold standard for generalisation to the wider population of MSM. The focus of this demonstration pilot was on reaching MSM who have never previously tested. While this group is a priority, MSM and other persons at risk are recommended to test more frequently, such as annually,29 in order to achieve the earliest possible diagnosis and the maximum benefits of treatment.
Despite limitations, our pilot project provides evidence in favour of a commonsensical approach to expanding HIV testing among MSM in China: place the tools in the hands of trusted community members who can efficiently bring the technology to them and individually walk HIV-positive persons through the early steps of their lifelong engagement in care. The CBO-based rapid testing and case management approach operationalises key components of the HIV response strategy of ‘Five Expand, Six Strengthen’ and is consistent with the established Chinese stance of national government leading policy, local health departments implementing policy and the full participation of society to maximise benefits. Community-based, non-judgemental, gay-positive rapid HIV test services have been accepted by MSM in other parts of the world.26 ,29 ,30 The present study translates and quantifies the contribution of such a programme in the Chinese context.
Key messages
-
A programme of trained peer volunteers to conduct venue-based HIV testing effectively reaches previously untested men who have sex with men (MSM) in China.
-
A peer-based social support and case management programme substantially improves linkage to HIV care over standard referral among newly diagnosed MSM in China.
-
There is need for MSM peer-based interventions to support retention in HIV care.
References
Supplementary materials
Abstract in Chinese
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Abstract in Chinese - Online abstract
Footnotes
-
Handling editor Jackie A Cassell
-
Contributors HY and RZ led the research design. HY, CW and HY composed the first draft of the manuscript. JL and JX implemented data collection and conducted the statistical analysis. WM contributed to the design, interpretation of data and made the final edits of the manuscript.
-
Funding (1) Outstanding Medical Academic Leader Programme of Jiangsu Provincial Centre for Diseases Control and Prevention (JKRC2011003); (2) Scientific Research Programme of Health Department of Jiangsu Province (H201330); and (3) National Social mobilisation Programme on HIV/AIDS prevention in 2011.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Ethical approval has been obtained from Jiangsu Provincial Centre for Diseases Control and Prevention Ethical Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.