Article Text

Abstract
Objective To determine the prevalence of, and risk factors associated with, Chlamydia trachomatis, Neisseria gonorrhoeae and Trichomonas vaginalis infection in pregnant women in Madang, Papua New Guinea (PNG).
Methods A cross-sectional survey was conducted among 400 pregnant women presenting to antenatal clinics. Sociodemographic and behavioural data were collected and real-time PCR diagnostic methods were used to detect the presence of chlamydia, gonorrhoea and trichomonas in self-collected vaginal swabs. The relationships between symptoms, sociodemographic and behavioural factors and infection were assessed.
Results The prevalence of C. trachomatis was 11.1%, N. gonorrhoeae was 9.7% and T. vaginalis was 21.3%. One-third of women (33.7%) had at least one infection. The most common symptom was abdominal pain (48.0%), but only abnormal vaginal discharge was consistently associated with infection (p<0.001). Women diagnosed with vaginal discharge syndrome were more likely to have at least one treatable infection (50.0% (47/94) vs 26.8% (68/254), p<0.001), yet 59.1% of women with infection would have been missed by the current clinically-based syndromic diagnosis. Risk factors included having a partner at perceived risk of infection, maternal extramarital intercourse, early sexual debut, lack of formal education, urban residence and smoking. 78.8% of women reported never using condoms.
Conclusions The prevalences of T. vaginalis, C. trachomatis and N. gonorrhoeae were high among pregnant women in coastal PNG. The poor performance of clinically based syndromic diagnosis suggests that alternative strategies are urgently required to improve detection and reduce the burden of sexually transmitted infections and their associated adverse pregnancy outcomes in this population.
- CHLAMYDIA INFECTION
- NEISSERIA GONORRHOEA
- REPRODUCTIVE HEALTH
- SEXUAL HEALTH
Statistics from Altmetric.com
Introduction
Bacterial and protozoal sexually transmitted infections (STIs) such as Chlamydia trachomatis, Neisseria gonorrhoeae and Trichomonas vaginalis are common in many resource-limited settings.1 The consequences of these infections include pelvic inflammatory disease, subfertility and infertility, miscarriage and ectopic pregnancy,2 premature rupture of membranes, chorioamnionitis, preterm birth, low birth weight and neonatal conjunctivitis1–3 and increased risk of HIV acquisition and transmission.4 Prompt diagnosis and treatment of STIs in pregnancy therefore has the potential to reduce adverse maternal and neonatal health outcomes in resource-limited, high burden settings.
Chlamydia, gonorrhoea and trichomonas infection have been found to be highly prevalent among women and men in a variety of different subpopulations within Papua New Guinea (PNG),5 ,6 but despite the known risks to the mother and baby, relatively little is known about the prevalence and risk factors associated with infection in pregnant women.5 In previous studies among rural women in PNG's Eastern Highlands Province, prevalences of asymptomatic infection with T. vaginalis, C. trachomatis and N. gonorrhoeae were 43%, 27% and 18%, respectively,7 ,8 whereas in antenatal women in Port Moresby, the capital city of PNG, C. trachomatis and T. vaginalis were common (C. trachomatis 18%, T. vaginalis 19%).9 ,10 In a recent survey, the tubal ectopic pregnancy rate at the Madang Provincial Hospital was 6.3 per 1000 deliveries, with 43% of these women having evidence of pelvic inflammatory disease.11
Antenatal care represents a unique opportunity to screen and treat women with STIs. Rapid diagnostic tests for HIV and syphilis are now available in antenatal clinics (ANC) in many developing countries, but simple, easy to use, affordable, highly sensitive and specific rapid diagnostic tests for C. trachomatis, T. vaginalis and N. gonorrhoeae are not yet widely available.12 Until quality diagnostic laboratory services, or suitable point-of-care diagnostics, become available for these pathogens, syndromic management remains the key strategy in developing countries to identify pregnant women at risk of infection.13 At present PNG, like many other developing countries, has adopted the syndromic management approach to the diagnosis and treatment of STIs. This approach relies on clinical symptoms and signs in the absence of laboratory confirmation14 and thus lacks sensitivity as up to 80% of women with chlamydia, gonorrhoea or trichomonas infection do not self-report symptoms, particularly in pregnancy.1 ,15
The evaluation of the infection burden and regional sociodemographic, behavioural and clinical risk identifiers is pivotal for the provision of tailored antenatal care to prevent the deleterious sequelae of STIs. Self-collected vaginal swabs have been previously identified as an acceptable sampling method and result in similar STI diagnostic performance to clinician-collected endocervical swabs or first-void urine.5 ,16
We determined the prevalence of C. trachomatis, T. vaginalis and N. gonorrhoeae among pregnant women in coastal PNG using self-collected vaginal swabs and assessed the association between STIs and clinical symptoms, sociodemographic and behavioural factors.
Methods
Study setting
In this cross-sectional survey we recruited a convenience sample of 400 pregnant women at their first visit to rural or urban ANCs in Madang, a province located along the North coast of PNG, between February 2011 and April 2012. All participants provided written informed consent for participation in a randomised controlled trial that investigated the efficacy of intermittent preventive treatment in pregnancy (IPTp) with azithromycin and sulfadoxine–pyrimethamine for the prevention of malarial infections and the control of STIs in pregnant women in PNG (IPTp study).17 Additional written informed consent was obtained from women who joined this substudy.
Eligibility criteria included age 16–49 years, gestation ≤26 weeks, singleton pregnancy, no known comorbidities and availability for follow-up until delivery. Baseline demographic and clinical data collected for the trial were supplemented with additional information obtained by the study clinician using a structured questionnaire regarding sexual history, symptoms and risk behaviour. Interviews were conducted in a private consultation room dedicated to this study.
At enrolment, women were tested for Treponema pallidum infection using a rapid serological test (Syphicheck-WB, Qualpro Diagnostics, India; sensitivity 84.5%, specificity 97.7%). When positive, confirmatory T. pallidum particle agglutination assays and rapid plasmin reagin (RPR) tests were performed (a reactive RPR, irrespective of titre, was used to define active syphilis). The hospital provided HIV counselling and testing: ethical approval for the study did not allow for collection of HIV data. Antenatal HIV prevalence at the main study site, Modilon General Hospital, was 1.1% during the study period (unpublished audit data, 2009–2012). Women with positive rapid tests for syphilis and/or symptoms and risk factors suggestive of an STI were referred to the nearest sexual health clinic, where counselling, detailed clinical examination, treatment and contact tracing were undertaken according to the PNG guidelines.14 Referral was preceded by an obstetric review if pregnancy-related causes of women's symptoms were suspected. Study participants found positive for chlamydia, gonorrhoea or trichomonas on subsequent laboratory analysis were notified by the study clinician and treated.
Sample collection
Following counselling, informed consent procedures and data collection, women were provided with a sterile single-tubed Dacron vaginal swab (Medical Wire and Equipment, UK) and advised to gently insert and advance the swab through the vaginal introitus until minimal resistance was felt, at which point the swab was slightly retracted, turned three times around its axis, removed from the vagina and immediately placed in the sterile sampling container. Women performed swab collection prior to receiving routine antenatal care and trial interventions. Following sample collection swab tips were clipped into sterile cryovials, stored at −20°C and subsequently transferred to the PNG Institute of Medical Research (PNGIMR) STI/HIV Research Laboratory in Goroka.
Laboratory procedures
To generate a suspension of sample material 1 mL of phosphate buffered saline was added to the swab tip and vortexed for 30 seconds. Two hundred microlitres of this suspension was used for DNA extraction with the NucleoSpin Tissue kit (Macherey-Nagel, Germany), performed according to the manufacturer's recommendations for extraction from cultured cells.
A Bio-Rad CFX96 Real Time PCR Detection System with CFX Manager software (V.2.1; Bio-Rad, Hercules, USA) was used for real-time PCR and analysis, respectively. Samples were tested for the presence and integrity of an adequate amount of human DNA through amplification of a 268 bp region of the β-globin gene using the primer pair GH20/PC04 published by Saiki et al.18
T. vaginalis was detected using published primers targeting a 102 bp of the A6p region of the genome (TVA5/A6).19 Detection of N. gonorrhoeae and C. trachomatis used previously published primer and probe sets targeting the opa gene and multicopy cryptic plasmid, respectively.20–23 A detailed description of laboratory procedures has been previously published.6
External quality assurance for C. trachomatis and N. gonorrhoeae PCR was provided through the Royal College of Pathologists of Australia. Samples with no amplification of the so-called housekeeping gene, β-globin, but positive by PCR result for one or more STIs were included in the analyses.24
Statistical analysis
Analyses were performed using Stata 12.0 (Stata Corporation, USA). We examined potential risk factors and symptoms for four different infection groupings: (1) one or more of the three STIs, (2) C. trachomatis, (3) N. gonorrhoeae and (4) T. vaginalis.
Univariate comparisons of variables were performed using the χ2 test or Fisher's exact test for categorical data, the Student t test for parametric data, and the Mann–Whitney U test for nonparametric data. ORs and 95% CIs were calculated. Results were considered statistically significant if p<0.05. To adjust for confounding, all factors with a tendency for association with infection on univariate analysis (p<0.1) were included in a multivariable logistic regression model as a starting model for a backward stepwise elimination model selection procedure. Variables significant at p<0.05 in the final model were considered independent risk factors. Only women with complete data for both infection and potential risk factors were included in multivariable analyses. Age at enrolment and age at sexual debut were dichotomised as <21 and ≥21 years and <16 and ≥16 years, respectively, as these cut-offs demonstrated the strongest association with infection and were deemed most useful for potential clinical use.
Ethical approval
This study was approved by the PNGIMR Institutional Review Board (1011), and the PNG Medical Research Advisory Council (MRAC; 10.40). The parent clinical trial received approval from IRB (0815), MRAC (08.01) and Melbourne Health Human Research Ethics Committee (2008.162). The clinical trial registration number is NCT 01136850.17
Results
Sociodemographic, reproductive and behavioural characteristics
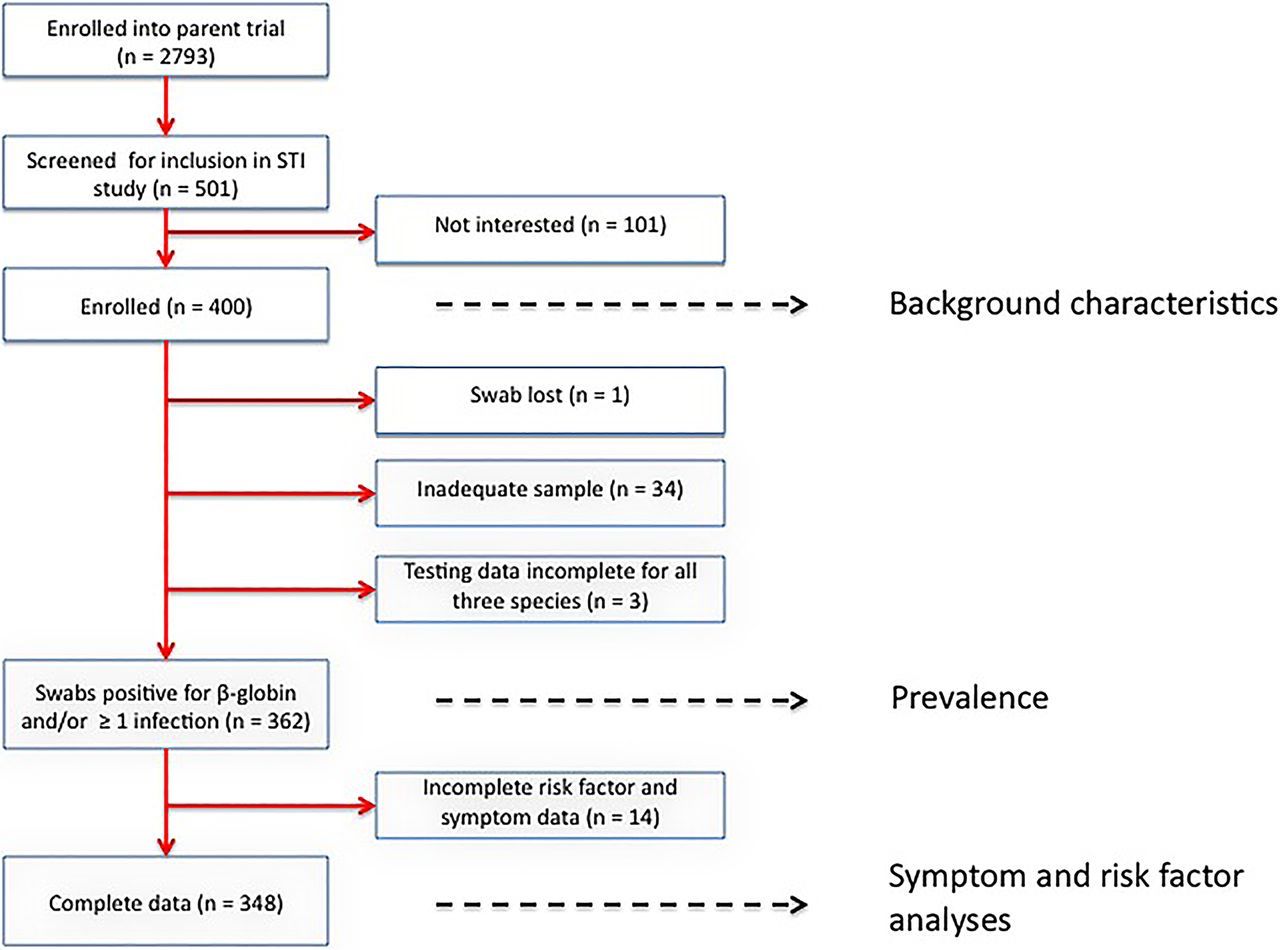
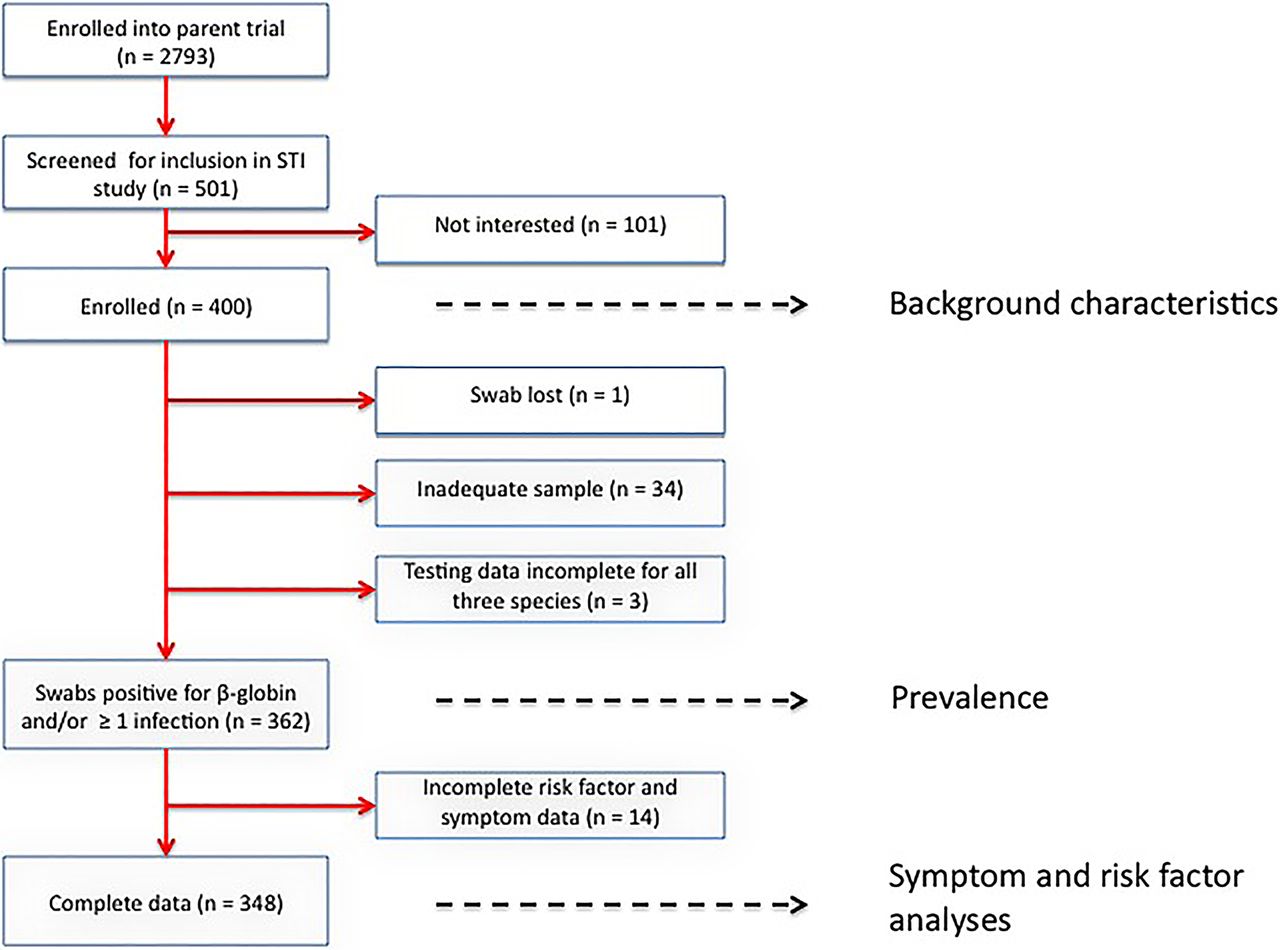
A total of 501 women enrolled in the parent clinical trial were screened and 400 were ultimately included in this study (figure 1). The mean age of participants was 24.6±5.4 years (range 16–39) and 27.5% (110/400) of women were <21 years of age. Other characteristics are summarised in table 1.
Baseline sociodemographic, behavioural and clinical characteristics of study participants (n=400)
{kind=link}
Participant flow chart. STI, sexually transmitted infection.
Seventy-nine per cent of women (315/400) had never used a condom, and similar levels were observed among women who had previously presented to an STI clinic (75.0%, 43/57), engaged in extramarital sex (76.0%, 63/83) or had knowledge of their partners engaging in extramarital sex (78.9%, 71/90). Maternal extramarital sexual intercourse (defined as having male intercourse with someone other than the father of the index pregnancy since falling pregnant) was not uncommon (20.9%, 83/398). Nearly a quarter of women (22.7%, 90/397) knew that their current partners were sexually involved with another woman (since falling pregnant). Women aged ≤25 years were less likely to have extramarital partners compared with older women (15.4% (39/253) vs 30.3% (44/145), p<0.001) and partners of women engaging in extramarital sex were more likely to have extramarital relationships themselves (45.1% (37/82) vs 16.6% (52/314), p<0.001).
Women who had extramarital relationships (27.7% (23/83) vs 10.8% (34/314), p<0.001) or who had knowledge of their partners being sexually involved with another woman (21.1% (19/90) vs 12.4% (38/306), p=0.039) were more likely to have attended health facilities for STI-related symptoms.
Symptoms
The most common symptoms participants experienced at any stage during the index pregnancy were lower abdominal pain (48.2%, 192/398) and vulval or perianal itchiness (35.8%, 143/400; table 1). A total of 26.5% (106/400) of women reported an abnormal vaginal discharge; 28.6% of women (114/398) were asymptomatic, 53.3% (212/398) reported up to three symptoms, and 18.1% (72/398) reported ≥4 symptoms.
Women with an abnormal vaginal discharge or abdominal pain were more likely to perceive their current partner as being at risk of an STI (vaginal discharge: 51.9% (55/106) vs 26.8% (78/291), p<0.001; abdominal pain: 41.6% (79/190) vs 25.9% (53/205), p<0.001). Women who had engaged in extramarital sex, or had knowledge of their partner doing so, were more likely to report an abnormal vaginal discharge (37.4% (31/83) vs 23.8% (75/315), p=0.013 and 35.6% (32/90) vs 23.8% (73/307), p=0.026).
None of the symptoms were due to an acute clinical cause (e.g. rupture of membranes, preterm labour).
Prevalence of infection
Of 399 vaginal swabs available for laboratory analysis, 34 (8.5%) were PCR-negative for both the housekeeping gene and all STIs, and three had incomplete testing data. Thus, 37 women were excluded from further analysis (figure 1). Demographic and clinical characteristics (table 1) did not differ significantly between women who were PCR-negative (n=34) and those who were not (n=365; data not shown).
One-third of women (33.7%; 122/362) had swabs that were positive for at least one STI. T. vaginalis was found in 21.3% (77/362), C. trachomatis in 11.1% (40/362) and N. gonorrhoeae in 9.7% (35/362). A total of 26.5% (n=96) had single infections, 6.1% (n=22) had 2 concurrent infections and 1.1% (n=4) had all three pathogens present. Sixty-two women (17.1%) had C. trachomatis and/or N. gonorrhoeae. Women with C. trachomatis were more likely than other women to also have N. gonorrhoeae infection (30.8% (13/40) vs 6.8% (22/322), p<0.001). Of 391 women tested for T. pallidum infection, four were positive for active syphilis (1.0%), but did not have any of the other STIs.
Association of symptoms and participant characteristics with infection
A total of 348 women had complete data for infection status, potential risk factors and symptoms.
On univariate analysis, all three infections (on their own and combined) were associated with an abnormal vaginal discharge (abnormality of smell, colour and/or quantity; table 2). N. gonorrhoeae infections were also associated with lower abdominal pain (p=0.036) and dysuria (p=0.021). Compared with uninfected women, women with one or more STI (80.9% (93/115) vs 66.5% (155/233); p=0.005) and women with N. gonorrhoeae (90.6% (29/32) vs 69.3% (219/316), p=0.011) were more likely to report at least one symptom (table 2). Fifty per cent of women (47/94) who were diagnosed with, and treated for, vaginal discharge syndrome (VDS) had at least one STI, compared with 26.8% (68/254) of women without VDS (p<0.001; sensitivity 40.9%, specificity 79.8%, positive predictive value 50.0%, negative predictive value 73.2%). Women <21 years of age were more likely to have C. trachomatis and less likely to have T. vaginalis infection (table 2), but maternal age did not remain significantly associated with infection in adjusted analyses.
Symptoms and factors associated with Chlamydia trachomatis, Neisseria gonorrhoea and Trichomonas vaginalis infection (n=348)
Behavioural risk factors associated with infection in multivariable analyses included early age at sexual debut and maternal extramarital sex (for C. trachomatis); women perceiving their partner at risk of infection (T. vaginalis); and maternal smoking (N. gonorrhoeae; table 2). Demographic and socioeconomic risk factors that remained significantly associated with infection in multivariable analyses included urban residence (N. gonorrhoeae) and lack of formal education (C. trachomatis and T. vaginalis). Other factors assessed (table 1) were not associated with infection.
Discussion
One third of pregnant women attending ANC in Madang Province, PNG, were infected with C. trachomatis, N. gonorrhoeae and/or T. vaginalis. Our figures are similar to earlier findings in pregnant women in Port Moresby and Goroka5 ,9 ,10 and to results of ongoing research in antenatal populations in four provinces of PNG (A. Vallely, unpublished observations).
However, higher prevalences of C. trachomatis were reported a decade ago in a population of low-risk non-pregnant rural women in the Eastern Highlands Province of PNG,8 in whom syphilis, T. vaginalis and N. gonorrhoeae infection were also more prevalent compared with the North Coast of PNG. In 2009, antenatal records revealed an HIV and a syphilis prevalence of 2.0% and 8.4%, respectively, at the Goroka hospital in the Eastern Highlands Province and 0.0% and 0.7%, respectively, at Madang Hospital on the North Coast of PNG.25 Together, these findings suggest that the burden of STIs among pregnant women in PNG has changed little in the past two decades, despite widespread implementation of the syndromic management approach to STI diagnosis and treatment.
Syndromic diagnosis had suboptimal performance in our study with nearly 60% of antenatal women with a laboratory-confirmed chlamydia, gonorrhoea or trichomonas infection not detected on clinical grounds alone. This study suggests that additional risk markers to those currently included in the PNG syndromic management guidelines could improve the sensitivity of this approach in this setting. These include women's perception of their partner being at risk of infection, extramarital sex, urban residence, low educational status and early age of sexual debut.26 ,27 Young maternal age, a risk factor included in the PNG national guidelines, was associated with C. trachomatis infection, but T. vaginalis infections were more common in older women. Condom use (ever since sexual debut) was very low, even among women who had previously attended an STI clinic. The low use of condoms in this cohort may relate to poor availability, lack of adequate counselling at STI clinics, lack of awareness and perceived risk and sociobehavioural factors, e.g. women's limited ability to negotiate condom use within marriage which may be exacerbated during pregnancy when their use can no longer be justified for family planning purposes. A low threshold for the diagnosis and treatment of STIs, coupled with improved awareness among health workers, pregnant women and their partners, could result in more appropriate and effective care. A more optimal approach to the diagnosis and treatment of STIs in pregnancy would be the use of highly sensitive and specific, easy to use point-of-care diagnostic tests, as recommended by other STI in pregnancy studies.1 An evaluation of newly available molecular technologies for the point-of-care diagnosis of C. trachomatis, N. gonorrhoeae and T. vaginalis among pregnant women is being conducted by the PNGIMR in three sites in PNG and is expected to be completed in 2015.
When interpreting the findings of this research, a number of study limitations need to be considered. First, study inclusion criteria and placement within a parent clinical trial may have resulted in selection bias, and the true prevalence of STIs may have been overestimated or underestimated. Second, older women were under-represented in our cohort, with more than half of the women <26 years of age, so that our findings are not broadly representative of the wider adult female population. Equally, young adolescents (<16 years) were not eligible for the study for consent reasons, yet may represent an important at risk group, given nearly 15% of participants reported a sexual debut at or below 16 years of age. Third, although adequate for prevalence estimates and the evaluation of key risk factors, numbers were small for some risk factors, precluding the accurate quantification of their impact. Furthermore, we may have underestimated the true prevalence of infection by self-sampling. The absence of β-globin in a number of samples that were excluded from analysis suggests inadequate sample collection in some women (figure 1). Finally, we opted to present associations between symptoms/risk factors and infection without adjusting for multiple comparisons, given the exploratory nature of this study and the ongoing debate regarding the value, role and type of such adjustments.28 ,29 This demands careful interpretation and further, hypothesis-driven evaluation of factors and symptoms found to be associated with infection in this study.
In summary, prevalences of C. trachomatis, N. gonorrhoeae and T. vaginalis were high among antenatal women in Madang Province, PNG. The poor performance of clinically-based STI syndromic diagnosis suggests that alternative strategies are urgently required to reduce the burden of these infections and their associated adverse pregnancy outcomes in this population.
Key messages
-
Chlamydia trachomatis, Neisseria gonorrhoeae and Trichomonas vaginalis infections were common in pregnant women in Papua New Guinea.
-
The current national syndromic diagnosis approach missed nearly two thirds of women with infection.
-
The majority of women reported never using a condom.
-
There is an urgent need for alternative strategies to reduce the burden of sexually transmitted infections and associated adverse pregnancy outcomes in this population.
Acknowledgments
We are very grateful to all the participating women and their families; the PNGIMR clinical, administrative, logistics and laboratory staff; the staff at the various participating health centres and hospitals; particular thanks go to Paula Samol, Selina Silim, Joy Paniu, Pauline Peng and Stephan Karl.
References
Supplementary materials
Abstract in Tok Pisin
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Abstract in Tok Pisin - Online abstract
Footnotes
Handling editor Jackie A Cassell
Contributors Conceived and designed the study: RAW, SJR and IM. Supervised enrolment of patients: RAW, MO and PS. Supervised and conducted laboratory procedures: SS, CS, NN, JW, CR, RAW and AV. Verified, analysed and interpreted the data: RAW, HWU, CSNLWS, IM, SJR and AV. Drafted original version of the manuscript: RAW and HWU. All authors participated in the writing of the manuscript, and read and approved the final draft.
Funding This work was supported by the Malaria in Pregnancy Consortium, through a grant from the Bill and Melinda Gates Foundation (grant number 46099).
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Papua New Guinea Institute of Medical Research (PNG IMR) Institutional Review Board and the PNG Medical Research Advisory Council (MRAC).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement All the data for this substudy was included in the paper.