Article Text

Abstract
Objective In three pilot regions of the Netherlands, all 16–29 year olds were invited to participate in three annual rounds of Chlamydia screening. The aim of the present study is to evaluate the cost-effectiveness of repeated Chlamydia screening, based on empirical data.
Methods A mathematical model was employed to estimate the influence of repeated screening on prevalence and incidence of Chlamydial infection. A model simulating the natural history of Chlamydia was combined with cost and utility data to estimate the number of major outcomes and quality-adjusted life-years (QALYs) associated with Chlamydia. Six screening scenarios (16–29 years annually; 16–24 years annually; women only; biennial screening; biennial screening women only; screening every five years) were compared with no screening in two sexual networks, representing both lower (‘national network’) and higher (‘urban network’) baseline prevalence. Incremental cost-effectiveness ratios (ICERs) for the different screening scenarios were estimated. Uncertainty and sensitivity analyses were performed.
Results In all scenarios and networks, cost per major outcome averted are above €5000. Cost per QALY are at least €50 000. The default scenario as piloted in the Netherlands was least cost-effective, with ICERs of €232 000 in the national and €145 000 in the urban sexual network. Results were robust in sensitivity analyses.
Conclusions It is unlikely that repeated rounds of Chlamydia screening will be cost-effective. Only at high levels of willingness to pay for a QALY (>€50 000) screening may be more cost-effective than no screening.
- CHLAMYDIA TRACHOMATIS
- COST-EFFECTIVENESS
- SCREENING
- MATHEMATICAL MODEL
Statistics from Altmetric.com
Introduction
Chlamydia trachomatis (Chlamydia) is the most commonly reported sexually transmitted infection in Western countries.1 Chlamydia is often asymptomatic but may cause serious health problems, such as pelvic inflammatory disease (PID), ectopic pregnancy and infertility. Several countries have therefore introduced some form of screening for Chlamydia, especially in the younger age groups where infection is most common. Screening can be performed either systematically (register based), by inviting sexually active people under a certain age, or can be offered as an opportunistic screening programme.2 A systematic review concluded that evidence of a beneficial effect of mass screening only applied to register-based approaches.3 No evidence for the effectiveness of opportunistic screening in the general population nor for multiple rounds of screening was found.3 Furthermore, a recent clinical trial in 2529 sexually active female students could not detect a significant reduction in PID 12 months after systematically screening women.4
Contrary to conclusions drawn from empirical evidence, most mathematical modelling approaches have been optimistic about the possibility that screening reduces the prevalence of Chlamydia in the population.5 Based on model output supporting the effectiveness of Chlamydia screening, most studies are positive on cost-effectiveness as well.5 Recent reviews critically assessed both methods and outcomes of economic evaluations in this field5 and the transmission dynamic models underlying economic evaluations.6 A large variation in important model parameters was found, for instance related to the association between Chlamydial infection and long-term sequelae,5 to the duration of asymptomatic infection and to the proportion of infections that is asymptomatic.6 Many published economic evaluations have used static models to estimate future spread of the infection while the standard has moved to dynamic modelling.5 Further, the use of intermediate outcome measures, such as cost per case detected or cost per major outcome averted (MOA), hampers a clear-cut interpretation of the results of economic and modelling studies in a healthcare policy-making environment, where cost per quality-adjusted life-year (QALY) is the preferred outcome parameter. In a context of scarce healthcare resources, any new screening programme should be evaluated for its relative efficiency compared with a situation without screening, that is, to usual care. In the Netherlands, small-scale pilot Chlamydia screening projects have been evaluated positively with regard to both effectiveness and cost-effectiveness.7–9 In 2004, the Health Council of the Netherlands advised positively on the introduction of a national Chlamydia screening programme, conditional upon additional evidence on feasibility, effectiveness and cost-effectiveness.10 Subsequently, large-scale pilot implementation projects in three Dutch regions (further referred to as Chlamydia Screening Intervention (CSI)) were planned to provide this additional evidence. In these regions, which differ with regard to degree of urbanisation and baseline prevalence, screening was rolled out in three consecutive rounds, following a stepped-wedge design.11 The aim of the present study is to evaluate the cost-effectiveness of Chlamydia screening by combining (extensions of) previously developed economic and mathematical models with empirical data as observed in the CSI project.
Methods
Modelling the CSI
The large-scale screening intervention was executed between 2008 and 2011 and has been extensively described elsewhere11 ,12 and is shortly described in the online supplementary annex. Schmid et al13 ,14 explored future transmission dynamics for a period of 10 years after start of the intervention (see the online supplementary annex for more details). The resulting age-specific incidences for a 10-year period served as input for an outcome tree, specifying disease consequences of an asymptomatic Chlamydial infection, separate for men and women (for all disease states included, see figure 1 of the online supplementary annex). Table 1 specifies the probabilities that certain disease states will occur. Probabilities were derived from the literature and, in case of PID and chronic pelvic pain (CPP), adapted after discussion in the CSI project group. All future disease states were counted in the year of asymptomatic infection, applying discounting to correct for the age-specific expected delay between infection and its consequences for pregnancy, infertility and offspring. The model was an updated version of a previously developed model,8 ,9 ,15 with two additions: (1) the option to perform probabilistic sensitivity analysis and (2) the inclusion of direct effects for treated persons. In order to define the total costs of Chlamydial infections detected in different scenarios, we multiplied the number of infections and sequelae by their estimated costs. We retrieved the number of major outcomes (MO, ie, infection sequelae, defined as PID, infertility, ectopic pregnancy and neonatal pneumonia) and computed the number of QALYs lost due to infection. For each screening strategy, this resulted in 10-year estimates of the total number of infections and the total number of MO and QALYs lost due to Chlamydial infection. The costs of screening were estimated based on the actual programme budgets of STI AIDS Netherlands, the central coordinating organisation for the CSI project, and the three regional Public Health Services involved in CSI. Costs for the treatment of Chlamydia and its sequelae, as well as costs associated with productivity losses, were updated and adapted from previous models8 ,9 ,15 or taken from recent literature. To calculate outcomes in terms of QALYs, we used data on the duration of MO and quality of life losses associated with MO, as provided by Stratton et al.16 Input data for the model are summarised in table 1. All future (ie, from year 2 onward) costs and effects were discounted at 4% and 1.5%, respectively, following Dutch guidelines for pharmacoeconomic research. The base year for the analysis was 2010. The perspective for the analysis was the societal perspective. More methodological details are given in the online supplementary annex.
Disease probabilities, probability distributions, durations of disease state, utility loss per case and treatment cost per case

{kind=link}
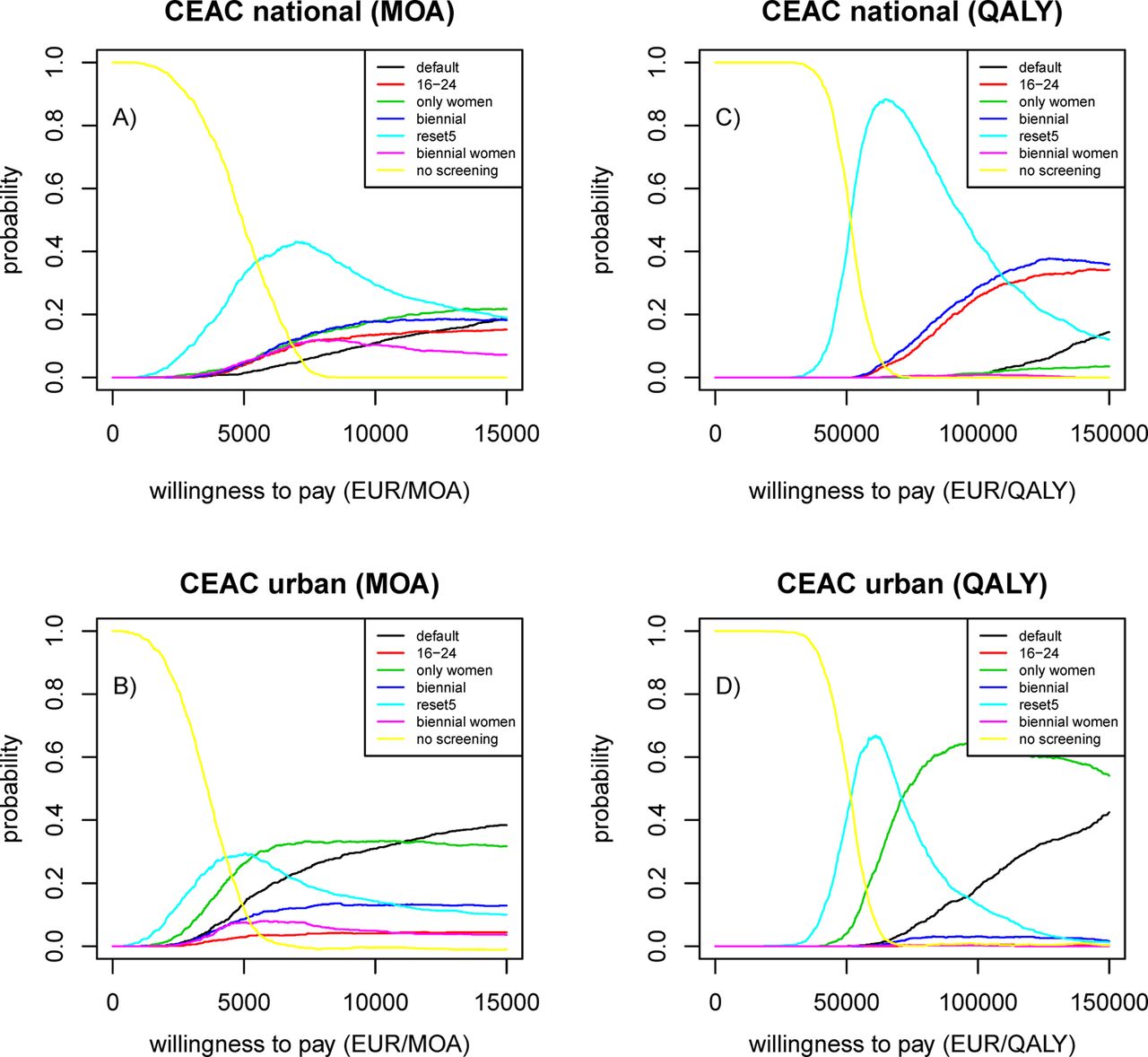
Cost-effectiveness acceptability curves (CEAC) showing the probability that a certain screening scenario is most cost-effective at different levels of willingness to pay per major outcome averted (MOA)/quality-adjusted life-year (QALY). Per value of willingness to pay (x-axis), different policy options have higher and lower probability to be the most cost-effective policy option. Per value of willingness to pay, the seven probabilities for seven policy options (six screening scenarios+no screening) accumulate to a probability of 1. EUR, euros.
Scenarios for Chlamydia screening
Six different scenarios for implementation were modelled, analogous to the transmission dynamics model:13
Default CSI: invite all 16-year-old to 29-year-old men and women annually (the strategy as implemented in the three CSI regions in 2008–2011).
Women only: invite all women aged 16–29 years for annual screening.
Young persons only: invite all men and women aged 16–24 years for annual screening.
Biennial: same as default scenario, but only sending invitations every two years.
Biennial women only: sending invitations every two years to women only.
Screening every five years: same as default scenario, but only sending invitations every five years, assuming people do not remember previous invitations (ie, uptake as in year 1 and no declining participation rates).
By comparing the numbers of incident cases in the different scenarios, we estimated the number of averted infections when one scenario for implementation is chosen compared with another scenario or no screening at all. Analogous to Schmid et al,13 ,14 we differentiated between the average national Chlamydia baseline prevalence (2%, ‘national sexual network’) and a higher, urban prevalence (3.4%, ‘urban sexual network’).
Cost-effectiveness estimates
For each scenario, total costs and total number of effects for a 10-year implementation scheme were calculated. Total costs were calculated by adding 10-year programme costs, variable costs for invitations and screening (depending on actual uptake of programme in three years of CSI screening and assumptions on uptake in years 4–10, in correspondence with mathematical modelling), total direct healthcare costs and indirect costs (productivity losses) associated with Chlamydia and its sequelae. Cost-effectiveness of the six different scenarios of Chlamydia screening implementation was compared with the usual care scenario (ie, no systematic screening) by calculation of the total incremental discounted costs for a 10-year implementation scheme divided by incremental discounted number of MOAs/QALYs. In addition, scenarios were compared among each other to estimate incremental cost-effectiveness.
Sensitivity and scenario analyses
We employed univariate sensitivity analyses with regard to critical assumptions in our natural history model, particularly with regard to the inclusion of CPP as MO. We also employed a model that included preterm delivery as MO, as a study observed that a maternal Chlamydial infection may be associated with an increased risk of preterm delivery.20 Another sensitivity analyses related to the health state utility values as used in our model.16 A recent review summarised all published utility values for Chlamydia-related health states PID, tubal infertility and ectopic pregnancy.21 We employed sensitivity analyses using the highest utility values for these three health states and using the lowest possible utility values (more details in the online supplementary annex). To explore the influence of the main uncertainties in our model, we employed a probabilistic sensitivity analysis. Results are plotted on the cost-effectiveness plane and as a cost-effectiveness acceptability curve (CEAC). CEAC shows the probability that a certain screening scenario is cost-effective at different threshold levels of willingness to pay for a QALY. Furthermore, in a scenario analysis, we looked at the influence of participation in the programme, as uptake of the screening offer appeared to be far less with CSI than in previous Dutch pilots. A hypothetical increase of participation in year 1 from the observed average of 16–30%, with reductions in uptake of the programme in the following years at a speed as observed in the CSI project, was assumed for this scenario analysis.
Results
Cost-effectiveness of different scenarios
Table 2 shows the costs, effects and cost-effectiveness ratios for six scenarios and two sexual networks. Related to the higher baseline prevalence, outcomes are somewhat more favourable for the urban sexual network than for the countrywide network. When compared with no screening, the default scenario of annual screening of both sexes has a cost-effectiveness ratio of €79 239 (urban sexual network) and €117 529 (national sexual network) per QALY, while the cost per MOA is €7980 and €9705, respectively. Of the six different scenarios tested, screening every five years appeared most cost-effective. However, cost per QALY are relatively high with ratios of at least €61 214 (national sexual network) and €51 556 (urban sexual network). If we consider the data in table 2 incrementally, the biennial women and 16-year to 24-year screening scenarios are always dominated (less effective and more expensive than alternatives or overruled by an alternative that generates more outcomes at a lower cost/outcome rate) in both sexual networks. Although the default scenario is the most effective in terms of MO averted and QALYs gained, the extra effects of the default scenario come at a cost of €232 143 per QALY in the lower baseline prevalence situation. Also in the urban sexual network, the default scenario of inviting all men and women is least efficient as the incremental gains of 40 QALYs compared with the women-only scenario can only be realised at an incremental cost of €5.8 million, yielding a ratio of €145 000 per QALY. The CEACs (figure 1) and the corresponding cost-effectiveness planes (see the online supplementary annex and online supplementary figure 3) show that screening has a low probability to be cost-effective, both in the national and in the urban network. Only if the willingness to pay for a QALY exceeds €50 000 screening may become more cost-effective than no screening.
Costs, effects and cost-effectiveness ratios, 10-year cumulative discounted results
Sensitivity and scenario analyses
Table 3 shows the results of the univariate sensitivity analyses for the inclusion of additional outcomes averted in the disease model (preterm delivery and CPP), as well as for the utility values for QALY calculations. For both preterm delivery and CPP, there is a small increase of the number of MO, corresponding with somewhat more favourable cost per MO averted. When analysing QALY outcomes, the impact of including CPP on cost-effectiveness of Chlamydia screening is huge. The number of QALYs gained increases more than tenfold, with corresponding decreases in the cost per QALY gained, now reaching levels around €6000–€7500 per QALY gained. The use of different utility values has substantial impact on the cost per QALY, especially if higher values are used, resulting in a 35% upward difference from the baseline results. When we inserted the lowest reported utility values from literature in our model, the cost per QALY was reduced by 11–14%. However, the cost per QALY remains high. A hypothetical increase of participation in year 1 from the observed average of 16% to 30% will not impact on cost-effectiveness levels importantly (table 3).
Univariate sensitivity analyses
Discussion
The current study concludes that large-scale Chlamydia screening most likely is not cost-effective if screening is unsuccessful in attaining high uptake in consecutive screening rounds, as was found to be the case in the Netherlands. Both in a situation of lower prevalence of Chlamydia (national sexual network, baseline prevalence 2.0%) and higher prevalence of Chlamydia (urban sexual network, baseline prevalence 3.4%), screening every five years has the most positive cost-effectiveness ratio compared with no screening. However, incremental cost-effectiveness ratios (ICERs) are high, starting at >€50 000 per QALY in the urban sexual network and €60 000 in the national network. The actual implementation of CSI, employing annual screening of all 16–29 years old, is most effective but highly cost-ineffective. When compared with the more cost-effective screening scenarios, ICERs are €145 000 per QALY (urban network) and €232 000 per QALY (national network). An extension of the sequelae of Chlamydial infection incorporated in our model to preterm delivery and CPP does not have a large impact on the cost per MOA but cost per QALY appeared to be extremely dependent on the assumptions made for CPP. The present study showed that only at high levels of willingness to pay for a QALY screening may be more cost-effective than no screening. Given the current uptake (16% in round 1), it is unlikely that repeated rounds of Chlamydia screening will be cost-effective in the Netherlands in the near future.
In the current study, the absolute level of cost per MOA is much higher than found in most previous research, which showed ratios <€1000 per MOA, or even cost-savings alongside better health outcomes.7 ,8 However, one other recently published Irish study reported similar high ratios of cost per MOA and cost per QALY.22 The relatively high levels of cost per MOA in our study are a reflection of the low participation rates as seen in the three consecutive screening rounds of the CSI project. Participation in three repeated rounds of screening was low after the first invitation (16%) and further declined over time (to 9% in the third round).11 Previous research appeared to be overly optimistic on long-time willingness to participate, with assumptions of constant annual uptake rates of 47% in women and 33% in men7 ,23 or acceptance of an annual screening test offered by the general practitioner of 91–96%.8 However, even a hypothetical increase of the uptake of screening to 30% in year 1, with similar declines in participation as observed in the CSI programme afterwards, would not change the conclusion that Chlamydia screening is not cost-effective. The largest part of our total cost estimate is related to the annual programme costs. Those costs have to be made irrespective of the uptake of the programme, implying that the total cost per invitation, the total cost per test and the total cost per case of Chlamydia found is relatively high.
Besides the limited uptake of the screening offer, as discussed above, assumptions on identification of Chlamydia in usual care, on baseline prevalence of Chlamydia in the population and on the probability of developing complications after Chlamydial infection are important factors that contribute to differences in outcomes between the current and previous studies.24 The relatively high background level of identifying and treating asymptomatic Chlamydia in regular healthcare13 influenced these results. This was not taken into account in earlier models. Furthermore, a much higher baseline prevalence in the population of 4.2% was assumed in previous Dutch research.8 By modelling cost-effectiveness of screening for two different sexual networks with different baseline Chlamydia prevalence, we have shown that (assumptions on) baseline prevalence impacts on cost-effectiveness. In a situation of high(er) baseline prevalence, it is easier to organise screening programmes in an efficient manner. As was described extensively in previous reviews,5 ,17 economic models tend to incorporate high estimates of Chlamydia-related complications. When compared with previous research, we were somewhat more conservative in our estimate of the probability of Chlamydia developing into PID (10% vs 20% in previous research). As future disease sequelae largely depend on the probability to develop PID, this conservative estimate also has consequences for the total number of MO averted by screening. As appears from our sensitivity analysis, the choice of MO to be included in analyses contributes heavily to conclusions on cost-effectiveness of screening. Previous models have included CPP,7 ,8 ,15 and our sensitivity analysis showed that CPP would be responsible for >90% of the total number of QALYs to be gained by screening. As the evidence base for CPP as Chlamydia-related outcome is extremely weak, we have chosen not to incorporate this outcome in our base case. The major uncertainties with regard to occurrence of disease sequelae of Chlamydia will not be resolved in the near future.17 Therefore, outcomes of different Chlamydia models have to be compared among each other and those models using high probabilities of occurrence of complications have to be reviewed with more caution when it comes to their conclusions on cost-effectiveness of Chlamydia screening.6
To estimate QALYs associated with Chlamydial infection and its sequelae, both utility values for Chlamydia-related disease outcomes and reliable estimates of the average duration of all Chlamydia-related disease outcomes are needed. Besides, if we want to compare utilities for different health states among each other, they have to be elicited using a similar instrument and a similar elicitation procedure. Despite the fact that five primary studies attempted at eliciting utilities for individual Chlamydia outcomes, Jackson et al21 concluded in a recent review that none of these studies can be used in economic evaluations without reservations. We used values from the Institute of Medicine (IOM) Committee to Study Priorities for Vaccine Development.22 Many details about the elicitation of utilities lack from the IOM report and have not been published elsewhere. However, in the absence of better data, we have used these utility values for QALY calculations, as was done by at least 11 other authors evaluating Chlamydia screening.22 Our sensitivity analyses showed that even the lowest utility values would not have changed our conclusion on the cost-effectiveness of screening. However, given the limitations of the utility values we used, combined with the uncertainty about the natural history of Chlamydia, our cost per QALY estimates should be viewed as an indication of cost-effectiveness of screening only.
One important lesson from the CSI project is that nationwide public health programmes preferably should be extensively piloted before an implementation decision is taken. Based on the pilot projects executed before, the Ministry of Health decided on nationwide implementation of Chlamydia screening in 2006, but not before some further questions were answered in large pilot studies. These further questions were of more operational character and did not concern the cost-effectiveness of screening, as ample evidence appeared to be present at the time. Based on actual experiences from the 3-year CSI project, we conclude that the real-life evidence base for cost-effectiveness of Chlamydia screening is less strong than appeared from previous Dutch and foreign research. In combination with limited evidence on the effects of screening on population prevalence of Chlamydia,11 it was decided by the Ministry of Health not to implement population screening in its present form. Other approaches targeted at risk groups within the population, such as free access to Chlamydia tests via internet, could be piloted and studied in order to identify more cost-effective ways of preventing adverse outcomes of Chlamydia transmission than population-based screening.
Our study results point at the fact that participation rates are crucial for reaching or maintaining cost-effectiveness of Chlamydia screening. Countries that have implemented national Chlamydia screening programmes may want to critically review their annual participation rates over time and put maximum effort in keeping participation as high as possible. Should countries be confronted with lowering participation over time, it may be relevant to evaluate the cost-effectiveness of screening once again.
Key messages
Register-based Chlamydia screening in the Netherlands was found to have relatively unfavourable cost-effectiveness ratios.
Unfavourable cost-effectiveness was related to low uptake rates of the screening offer and further declining participation in consecutive rounds of screening.
Only at high levels of societal willingness to pay for a quality-adjusted life-year screening may be more cost-effective than no screening.
Acknowledgments
We would like to acknowledge the contributions of Anita Suijkerbuijk, MSc, for help in updating the cost-estimates to 2010 cost levels. Furthermore, we also thank all members of the CSI study group, notably Johan S.A. Fennema, Hannelore M. Götz and Christian J.P.A. Hoebe, for expert advice on the disease progression estimates to be used in the model and for discussing the results of our study on several occasions.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Handling editor Jackie A Cassell
Contributors All authors were involved in the conception, design and execution of this work and interpreted the results. GAdW and MEK designed the study. BVS and MEK designed the mathematical model. RW, GAdW and ELMOdC designed the economic model. IB, EC and JB contributed to the design of the study and interpreted the results. GAdW wrote the first draft of the manuscript. All authors provided feedback on earlier drafts and read and approved the final manuscript.
Funding The Chlamydia Screening Implementation project was carried out on request of the Ministry of Health, Welfare and Sport. The Dutch Organisation for Health Research and Development (ZonMW, project number 12.400.001) funded the project.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.