Article Text

Abstract
Background General paresis (GP) is a late form of parenchymal neurosyphilis causing dementia and neuropsychiatric disorders. The diagnosis is often difficult since the clinical signs are protean. So far, neuroimaging has played a minor role as radiological findings are not specific.
Methods We studied three immunocompetent patients, admitted to hospital for cognitive impairment. The diagnosis of neurosyphilis was formulated on the basis of serological texts and cerebrospinal fluid analysis. The patients underwent a 3 T MR examination including susceptibility-weighted imaging (SWI) sequence before and after the initiation of penicillin therapy.
Results In all patients, SWI revealed cortical hypointensity, mostly distributed in frontal and temporal lobes. In drug-naive patients, the hypointensity extended over the whole cortical thickness, from the cortical/subcortical junction to the pial surface. After starting the penicillin therapy, the cortical hypointensity partially reversed, involving only the deep cortical layers.
Conclusions The MRI pattern at SWI observed in patients with GP was not reported in other infectious or inflammatory disease of the central nervous system, thus we suggest it could be a peculiar radiological finding of the disease. On the basis of previous pathological data, we hypothesise that cortical SWI hypointensity could be expression of iron deposits within activated microglia.
Statistics from Altmetric.com
Introduction
In the course of syphilis, the central nervous system (CNS) is early invaded by Treponema pallidum; however, neurological symptoms occur in a minority of patients. Neurosyphilis is usually divided into early forms, occurring within months or few years from the primary infection and involving blood vessels and meninges (ie, acute meningeal syphilis and meningovascular syphilis), and late forms that present with a latency of several years or decades and involve brain parenchyma and spinal cord (ie, general paresis (GP) and tabe dorsalis).1 ,2
GP is often misdiagnosed as primary neuropsychiatric or neurodegenerative disorder.1 Symptoms of GP mimic dementia and consist in insidious onset of memory and other cognitive function impairment, irritability and decline in personal appearance. Psychiatric symptoms may be present, while neurological examination could be entirely normal.3 Accurate diagnosis remains problematic as the signs are protean and there is not a gold standard among the supportive laboratory tests.4
Neuroimaging has played a minor role in recognising GP. In the largest retrospective studies, the most common radiological sign was brain atrophy, mainly affecting frontal and temporal lobes, with concomitant small white matter lesions. Since such findings were not specific, the authors concluded that neuroimaging is of limited value in supporting the diagnosis.5 ,6
Further radiological signs recently observed in a minority of patients with GP are represented by mesiotemporal hyperintensity or diffuse cerebral white matter hyperintensity on T2-weighted images. The differential diagnosis is either with herpes encephalitis, paraneoplastic encephalitis and mesial temporal sclerosis (MTS) or cerebral autosomal-dominant arteriopathy with subcortical infarcts and leukoencephalopathy and HIV encephalitis,6–9 respectively.
In this study, we report for the first time susceptibility-weighted imaging (SWI) findings in three cases of GP treated with penicillin therapy and propose a new reversible radiological finding of the disease.
Subjects and methods
Subjects
From March 2012 to June 2014, we investigated three immunocompetent men (age 38–43 years) admitted for slowly progressive cognitive decline and neuropsychiatric symptoms.
Patient 1was hospitalised after a 4-month history of ideomotor slowdown and ingravescent fluent aphasia, causing job loss and social isolation. He also had a 3-year history of focal temporal seizures with secondarily generalised tonic–clonic seizures.
Symptomatology of patient 2 started 8 months before the admission with personality changes (depression, apathy and irritability) and memory impairment. The patient then experienced progressive ideomotor slowdown, dysgraphia and dysarthria. He had nothing relevant in his medical history.
Patient 3 was admitted after a 4-month history of slurred speech and memory impairment, followed by the onset of fine tremors and impairment in motor coordination, with a bike fall immediately prior to hospitalisation. He had nothing relevant in his medical history.
All patients underwent conventional MR examinations at 1.5 T, which disclosed diffuse cortical atrophy, prevalent in frontal, temporal and insular lobes. In addition, hippocampal alterations resembling an MTS pattern (patient 1) and subcortical white matter lesions with neither mass effect nor contrast enhancement (patient 2) were observed.
Routine blood tests were normal. Laboratory tests performed in serum and cerebrospinal fluid (CSF) excluded several CNS infections (HIV I and II, herpes simplex virus type I and II, human herpesvirus VI, Epstein–Barr virus, cytomegalovirus, Borrelia burgdorferi). The diagnosis of neurosyphilis was formulated on the basis of positive Treponema pallidum haemagglutination assay in serum and CSF.10 CSF examinations revealed pleocytosis and increased protein content. The patients were treated with penicillin G (24 million units/day for 21 days). The clinical and laboratory evaluations at 1–3 months after starting penicillin treatment revealed improvement of memory deficit and neuropsychiatric symptoms, and normalisation of CSF tests in all subjects.
Demographic and clinical data and laboratory tests are summarised in table 1.
Demographic and clinical data of the three patients with general paresis at first evaluation
MR acquisitions at 3 T
All patients underwent brain MR examination at 3Tesla (SIGNA-350-MR-scanner, General Electric, Milwaukee). The MRI protocol included 3D-Fluid Attenuated Inversion Recovery, 3D-T1-weighted BRAin VOlume imaging, diffusion-weighted images (DWI), 2D gradient-echo (GRE) and SWI sequences (namely susceptibility-weighted angiography). Furthermore, 2D T1-weighted images were acquired after contrast medium administration. The time interval between the start of penicillin therapy and 3 T examination varied among patients. In detail, 3 T MRI was performed before the treatment in patient 1, 2 weeks after starting treatment in patient 2 and 3 months after in patient 3. The first two patients repeated 3 T MR examination 7 months later. One patient (patient 1) underwent also a 2-year MR follow-up.
Results
MRI findings at 3 T
Conventional sequences provided similar information at 3 and 1.5 T MRI and confirmed diffuse cortical atrophy prevalent in frontal, temporal and insular regions in all patients, associated with an MTS-like pattern in patent 1 and to multiple subcortical white matter lesions in patient 2. Subcortical white matter lesions showed partial reversibility after the initiation of penicillin therapy, while the other findings were unchanged.
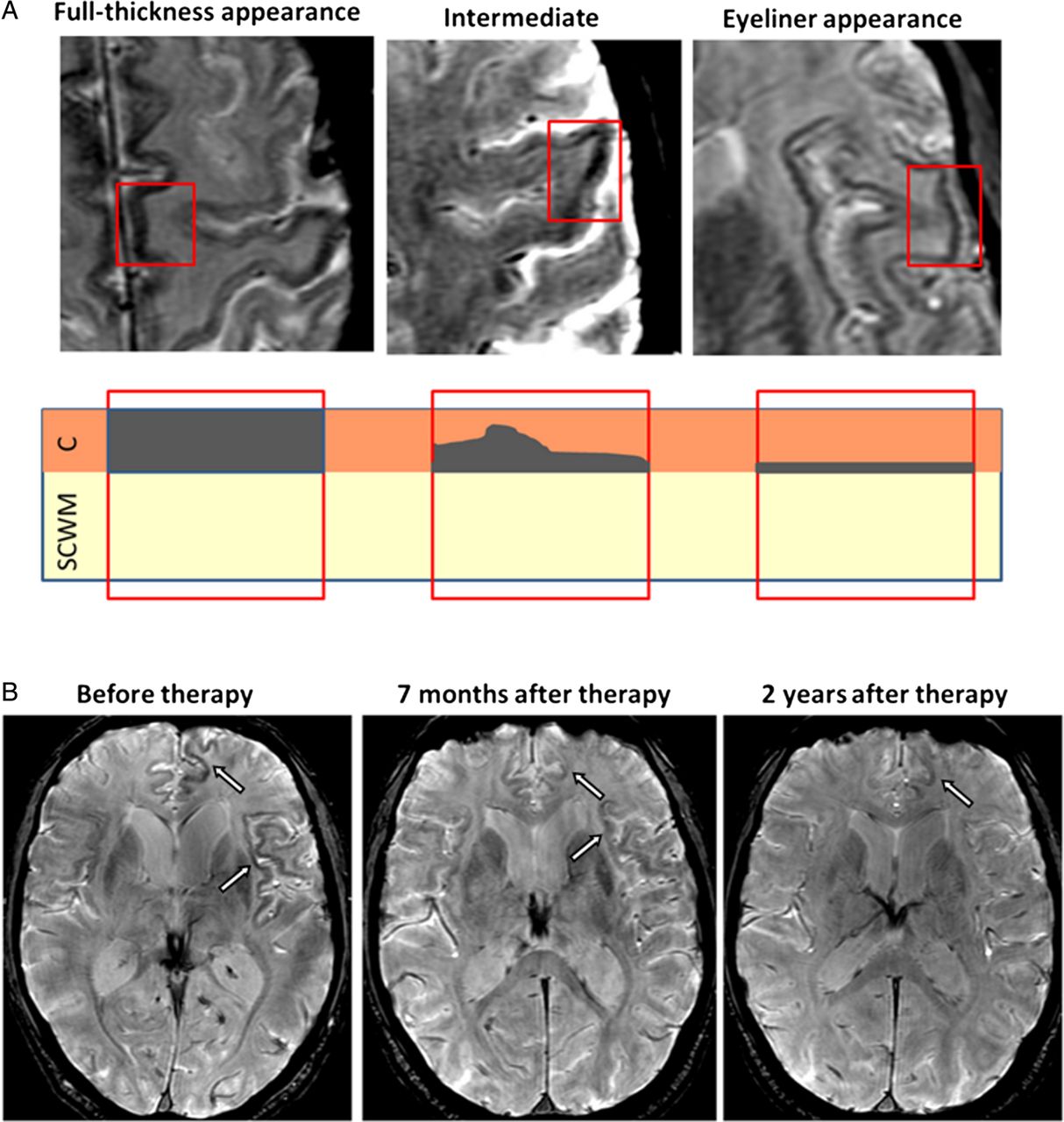
In all subjects, SWI sequence demonstrated a widespread cortical hypointensity involving frontal, temporal, parietal and insular lobes with asymmetric bilateral distribution. Such hypointensity did not correspond to signal alterations on conventional sequences (including 2D-GRE and DWI) and contrast enhancement. Before the initiation of therapy, the SWI hypointensity tended to extend across the whole cortical mantle, from the cortical/subcortical junction to the pial surface (‘full-thickness’ appearance; figure 1A). After the initiation of penicillin, the hypointensity demonstrated a partial regression, becoming fainter and fainter. Hypointensity progressively reduced its thickness and became confined to the deep cortical layers, and assumed the appearance of a thin dark line at the cortical/subcortical junction (‘eyeliner’ appearance; figure 1A, B). The ‘full-thickness’ and ‘eyeliner’ appearances of SWI hypointensity coexisted in the same patient; however, the first aspect prevailed before the initiation of therapy and the second one was predominant after therapy. In patent 1, a subtle hypointense line was still recognisable at the cortical/subcortical junction at 2-year MR follow-up (figure 1B).
{kind=link}
Patient 1. The patterns of cortical susceptibility-weighted imaging (SWI) hypointensity observed in patients with neurosyphilis at 3 T are reported in (A). The ‘full-thickness’ appearance is predominant before the initiation of penicillin therapy while the ‘eyeliner’ appearance becomes prevalent after treatment. The partial regression of cortical alterations is shown in (B). SWI on axial plane reveal cortical hypointensity prevalent in left frontal and insular lobes (arrows). Follow-up MR examinations demonstrate the progressive regression of the alterations. A thin dark line at the cortical/subcortical junction is still appreciable in the left frontal lobe at 2-year MR follow-up. SCWM, sub-cortical white matter.
MRI findings revealed by conventional sequences and SWI in the three patients and the available follow-up are reported in the online supplementary figure.
Discussion
Statement of principal findings
In the three patients with neurosyphilis who participated in this study, SWI sequence was able to disclose peculiar cortical hypointensity not visible with conventional sequences.
Strengths and weaknesses of the study
This is the first study in which SWI was employed in the investigation of neurosyphilis. So far no similar findings have been reported in any radiological study on infectious or inflammatory diseases. A major weakness of the study is represented by the small number of patients, which preclude generalisation of the results without additional evidences.
Meaning of the study
The MRI findings in patients with GP could reflect specific pathological data. On the basis of the distribution of spirochetes in the brain, GP can be divided into an ‘infiltrative form’ with prominent perivascular lymphoplasmocytes infiltrates and few spirochetes, and an ‘atrophic form’ with more accentuated cortical loss, hyperplastic microglia and a high number of spirochetes accumulated in the cerebral cortex.11 Both forms are characterised by the accumulation of iron in the infected brain tissue, in the walls of cortical vessels and in the cytoplasm of microglial cells.12 Microglial cells show a distinct activation state in neurosyphilis since they assume a bipolar form and align with nerve cells perpendicularly to the dural surface across cortical layers (microglial rod cells).11 ,13
The SWI sequence is particularly sensitive to detect the presence of paramagnetic products such as iron, providing useful information in numerous diseases, particularly in inflammatory disorders.14 ,15
We hypothesise that the cortical hypointensity seen in patients with GP is due to the iron accumulation in activated rod cells.
According to this hypothesis, the transition from the ‘full-thickness’ appearance of T2*-hypointensity to the ‘eyeliner’ appearance could reflect the transition from an activated state to a quiescent state of microglia in response to penicillin. Indeed, the reversion of hypertrophic cells to normal size and the regression of cellular alignment may be the basis of the partial reversibility of the SWI alterations. The persistent hypointensity in the deepest cortical layers requires a cautious approach. It could be the expression of persistent iron deposits within quiescent microglial cells after the resolution of the infectious injury; alternatively, it might represent iron accumulation within macroglia, which is known to proliferate in response to Treponema infection.13
Unanswered questions and future research
SWI is able to reveal the cortical damage in patients affected by neurosyphilis and to demonstrate its regression after proper therapy. We suppose that SWI might represent a valuable tool for the diagnosis and follow-up of the disease; however, further evidence is needed to determine whether the reported cortical alterations represent a specific radiological finding or is present also in other pathological conditions.
We suggest that SWI might allow new insights into the activated states of microglia in vivo, improving our comprehension of several inflammatory and neurodegenerative diseases.
Key messages
Susceptibility-weighted imaging (SWI) is able to identify cortical alterations in patients with general paresis.
The MRI findings could be expression of iron accumulation in activated microglia.
Further evidence is needed to determinate if the alterations revealed by SWI are specific radiological findings for neurosyphilis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figure
Abstract in Italian
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Abstract in Italian - Online abstract
Footnotes
Handling editor Jackie A Cassell
Contributors MS, IP and MC: study design and manuscript preparation. MS and IP: literature research. MS, IP and ID: MR data acquisition. RD, MG and FSG: clinical data acquisition. All authors: manuscript revision.
Competing interests None.
Patient consent Obtained.
Ethics approval 3 T MR acquisition was authorised by the Ethics Committee of Azienda Ospedaliera Universitaria Pisana (AOUP).
Provenance and peer review Not commissioned; externally peer reviewed.